Preterm infants have long-term healthcare needs. Oral feeding competency in preterm infants is deemed an essential requirement for hospital discharge. Despite achieving discharge readiness, feeding problems persist into childhood and can have a residual impact into adulthood. The early diagnosis and management of feeding problems are essential requisites to mitigate any potential long-term challenges in preterm-born adults.
1. Introduction
Oral feeding readiness in preterm infants is a concern often towards the tail-end of hospitalization. This only comes into the spotlight after other major medical concerns have been resolved or are manageable. While the evidence for the adult outcomes of preterm infants is increasing, the long-term impact of the altered development of oral neuromotor skills and abnormal oral feeding remains unclear, primarily due to a paucity of studies on adults born preterm. Given the diversity of underlying etiologies and clinical presentations of feeding problems, the lack of standardized definitions and assessments by which to identify and document oral feeding problems adequately is frustrating [1][9]. There is an urgent need for a two-pronged approach to feeding problems in infants born preterm in order to standardize diagnostic criteria and to develop individualized therapeutic strategies using a comprehensive multidisciplinary approach.
2. Oral Feeding and Feeding Problems in Preterm Infants
2.1. Development of Normal Swallowing in the Fetus
The precursors to oral feeding skills emerge in the early second trimester of pregnancy with evidence of sucking and swallowing in the developing fetus. Early evidence of fetal swallowing is seen at 11–12 weeks of gestation by the swallowing of amniotic fluid, followed by evidence of early sucking at 18–20 weeks
[2][3][10,11]. As the fetus enters the third trimester, the sucking and prefeeding skills are further refined, resulting in a mature sucking by term gestation. In an infant born preterm, the mature sucking–swallowing coordination is preceded by non-nutritive sucking (NNS) at around 28–33 weeks, which refers to repetitive sucking on a pacifier or a closed nipple without resulting in the delivery of a liquid bolus for swallowing
[4][5][12,13]. NNS occurs in short rapid bursts, which slows down as the sucking matures into a 1Hz sucking–swallowing–breathing pattern of nutritive sucking (NS) by week 32–34 of gestation with improved rhythmicity, amplitude, and volume expression
[3][5][6][11,13,14].
Mature swallowing occurs broadly in three phases
—the oral phase, the pharyngeal phase, and the esophageal phase
[7][8][15,16]. The oral phase in infancy is synonymous with the sucking that creates a vacuum followed by the expression of milk by the tongue compressing on the bottle or breast. Normal sucking is tied to receiving the appropriate sensory input from food, followed by a coordinated oral motor response. In the neonatal period, this is thought to be regulated by bilateral brainstem neural networks in the pontine and medullary reticular formation, called the suck central pattern generator (CPG). The CPG is responsive to stimulation and can be trained using oral stimulation with pacifiers, nipples, breastfeeding, and olfactory, tactile, or thermal stimulation
[5][9][10][11][13,17,18,19]. Sucking is reflexive in neonates and becomes more voluntary as the infant grows and learns to masticate
[7][15].
As the food bolus is pushed to the back of the oral cavity, a largely involuntary swallowing reflex is triggered in the pharyngeal phase. This leads to a sequence of events from the elevation of the velum leading to nasopharyngeal closure, followed by the pharyngeal swallowing reflex with the contraction of superior, middle, and inferior constrictors (resulting in pharyngeal closure). A brief respiratory pause with the closure of the vocal cords from the glottic closure reflex and laryngeal chemoreflexes help protect the airway during this phase. As the bolus moves to the esophageal phase, this activates a series of actions from hyoid elevation, relaxation of the cricopharyngeal muscle, opening of the esophagus, and the eventual peristaltic contraction of the esophagus (upper esophageal sphincter (UES) relaxation, primary peristalsis of the esophageal body, and lower esophageal sphincter (LES) relaxation) that moves the food bolus into the stomach, thus concluding the swallow
[2][10].
2.2. Feeding Problems in Preterm Infants in the Neonatal Period
The phrase “feeding problems” is often used to describe a diverse group of etiologies resulting in inadequate nutritional intake orally and could range from oral feeding difficulties (described in more detail below), gastroesophageal reflux (GER), dysmotility, and even systemic illnesses, unfortunately contributing to the lack of a uniform definition for feeding problems. The maturation of a normal feeding pattern can be interrupted in a preterm infant by extrauterine influences resulting in dysphagia or abnormal swallowing, with impaired sucking, swallowing, or airway protection, thus compromising the efficacy, adequacy, and, most importantly, the safety of oral feeding. Dysphagia can be a sign of underlying anatomical or neurological abnormality or injury, or merely functional immaturity altered by external sensory input, as seen in a preterm infant
[8][16]. Infants with dysphagia are phenotypically heterogeneous and have diverse etiologies, pathophysiology, and management.
Preterm infants, especially those born <32 weeks, are exposed to multiple life-saving interventions during their NICU stay that contribute to noxious orofacial sensory stimulation during a time of physiologic maturation. Additionally, during such a vital period of brain development, prolonged oxygen supplementation due to respiratory illnesses (respiratory distress syndrome (RDS) and bronchopulmonary dysplasia (BPD)), brain injury (intraventricular hemorrhage (IVH), periventricular leukomalacia (PVL) or hypoxic injury), complex medical illnesses such as necrotizing enterocolitis (NEC), surgeries, and underlying craniofacial abnormalities can further alter oral sensory and motor experiences impacting normal sucking and swallowing development. There exists a complex interplay between prematurity, pulmonary, neurological, and feeding problems independently linked to neurodevelopmental delays.
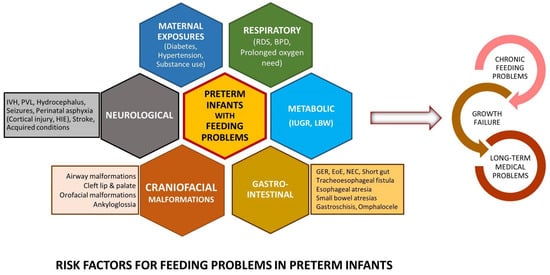
Figure 1 shows a selected list of common conditions linked to dysphagia. Dysphagia can also be mechanistically categorized by phases of swallowing with overlapping mechanisms.
Figure 1. Risk factors: Common clinical conditions associated with feeding problems in preterm infants. (BPD: bronchopulmonary dysplasia, EoE: eosinophilic esophagitis, GER: gastroesophageal reflux, HIE: hypoxic ischemic encephalopathy, IUGR: intrauterine growth restriction, IVH: intraventricular hemorrhage, LBW: low birth weight, NEC: necrotizing enterocolitis, PVL: periventricular leukomalacia, RDS: respiratory distress syndrome).
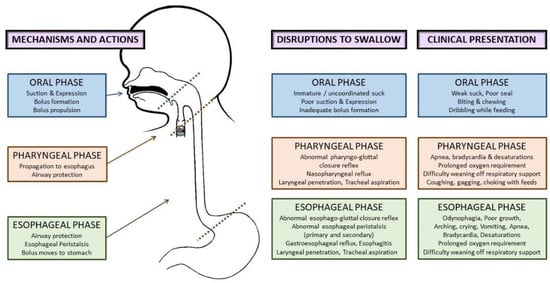
Aspiration during swallowing can occur broadly in three scenarios—anterograde aspiration in the oropharyngeal phase as bolus travels into the pharynx, retrograde aspiration (refluxed food bolus travels up the esophagus with failure to protect the airway), and silent aspiration (asymptomatic aspiration anytime during swallowing). Additionally, an abnormal pharyngoglottal closure reflex and esophagoglottal reflex associated with prematurity also contribute to abnormal airway protective mechanisms.
Figure 2 shows the phases of swallowing, normal actions in each phase, disruptions to swallowing, and their clinical presentation. In the neonatal period, feeding problems can present with diverse clinical manifestations, as shown below, leading to inadequate nutritional intake, increased length of hospitalization, and compromised airway safety
[1][2][8][9,10,16].
Figure 2. Etiopathophysiology of dysphagia in preterm infants: phases of normal swallowing, disruptions to swallowing, and clinical presentation in the neonatal period.
3. Feeding Problems in Preterm Infants beyond the NICU
Feeding problems in childhood and adults among preterm born infants have been described inconsistently. While previous studies have suggested that up to 1% of the pediatric population can present with feeding problems, the prevalence is likely to be significantly higher in preterm infants, proportional to the degree of prematurity [7][15]. Residual feeding problems in growing preterm infants span a broad spectrum of phenotypes, including feeding tube dependency [12][30], non-specific feeding difficulties, oral aversion [1][13][14][9,31,32], feeding aversion, poor progression to solid foods, challenges with eating specific food types (e.g., solids), and subtle swallowing difficulties.
Outcomes in Preterm Infants with Potential Link to Feeding Problems
3.3. Outcomes in Preterm Infants with Potential Link to Feeding Problems
Intrauterine growth restriction (IUGR) is linked to nutritional compromise in a fetus, preventing it from reaching its full genetic potential, and it is principally a vascular disorder with short-term and long-term consequences
[15][16][17][56,57,58]. There is a considerable void in the data on feeding problems in this cohort of preterm, low birth weight infants and their long-term outcomes. Feeding problems in these infants could signal functional immaturity of the central nervous system but can also be a sign of neurological injury or adaptability to being born preterm. Feeding problems impact more than nutrition in children and adults born preterm, often presenting with subtle difficulties. Specific signs are usually absent, and the subtlety of these minor signs makes it more challenging to identify and intervene timely and to potentially offer a chance to improve outcomes.
Preterm infants are also prone to higher rates of anoxic brain injury and IVH, with increased incidence of cerebral palsy often manifesting as subtle dysphagia. While the data on the long-term outcomes of preterm infants discharged home on tube feedings are sparse, term infants with congenital cardiac disease who are discharged home on an artificial mode of providing nutrition such as orogastric tubes or GT have poorer mental and psychomotor developmental indices
[18][59]. It would suffice to hypothesize that infants born preterm will more than likely have at least similar or worse neurodevelopmental issues when compared to their term peers.
4. Addressing Oral Feeding Issues Early
Feeding problems are dynamic and continue to evolve as the infant grows, requiring an ongoing assessment, intervention, and re-evaluation to optimize management. Early diagnosis and treatment of feeding problems involve a holistic approach to the individual’s specific feeding difficulties in order to decrease potential long-term challenges
[8][11][16,19].
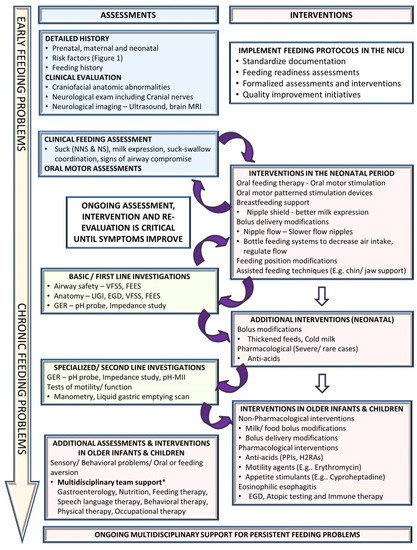
Figure 3 suggests an algorithmic approach for managing feeding problems in the neonatal period continuing into childhood.
Figure 3. Approach to a preterm infant with feeding problems. (EGD: esophagogastroduodenoscopy, FEES: fiberoptic endoscopic evaluation of swallowing, GER: gastroesophageal reflux, H2RA: H2-receptor antagonists, MRI: magnetic resonance imaging, NICU: neonatal intensive care unit, NNS: non-nutritive suck, NS: nutritive suck, pH-MII: pH monitoring multichannel impedance, PPIs: proton pump inhibitors, UGI: upper gastrointestinal fluoroscopy, VFSS: videofluoroscopic swallow study).
.1. Clinical Assessment
4.1. Clinical Assessment
A detailed history includes prenatal history, maternal medical problems and exposures, birth history, neonatal course by systems, and a description of the signs and symptoms. Physical examination should evaluate the anatomy of the oropharyngeal structures and identify craniofacial anomalies and neurological status, including cranial nerves. The quality and maturity of the sucking, milk expression, and sucking–swallowing coordination are assessed. Abnormalities during a bedside feeding, such as wet voice, gagging, choking, and drooling, could suggest a possible airway compromise that may require targeted instrumental assessment. However, it is essential to note that the pediatric population is suspected of having a high prevalence of silent aspiration of unknown significance and may not be identified accurately on clinical assessments alone.
4.2. Non-Pharmacological Interventions
Multidisciplinary feeding teams including neonatology, speech pathology, and occupational and physical therapy are integral to understanding the intricacies of feeding issues related to prematurity and the complex interplay of other comorbidities. Neonatal interventions for dysphagia are primarily conservative, involving non-pharmacological management. Feeding readiness assessments for maturity and respiratory safety—informal or structured—are essential to guide the initiation of oral feeds in a preterm infant. Oral motor therapy is an essential element for the improvement of readiness to start feeding
[3][9][11,17]. The pace of transition from tube feeds to oral feeds varies by the level of maturity of the infant. Feeding modifications using changes in feeding position, chin, cheek, or jaw support, and changes in nipple flow rates are frequently used in the neonatal period
[7][19][20][15,64,65]. Breastfeeding support using nipple shields can aid in improved milk expression.
4.3. Instrumental Assessment
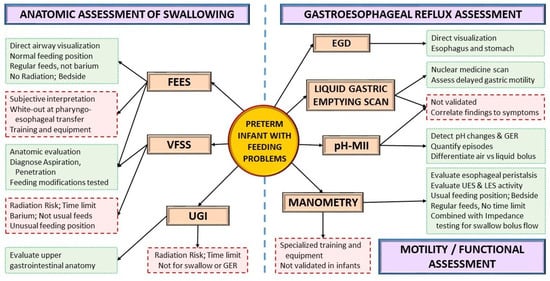
Instrumental assessments can be used to evaluate the anatomy or function of aerodigestive structures and the presence of GER as the infant grows (
Figure 4). A VFSS or modified barium swallow study provides a fluoroscopic view of the swallow while the infant is fed barium at different consistencies. VFSS is one of the most widely used instrumental assessments for dysphagia in neonates and infants
[21][22][70,71]. Conversely, fiberoptic evaluation of swallowing (FEES) provides a direct view of the airway during actual feeding, without the risk of ionizing radiation, but with a momentary white-out period at the pharyngo-esophageal transfer. Introduced in the 1980, FEES has only recently gained popularity in the neonatal population due to the development of smaller neonatal-sized endoscopes
[23][24][25][26][27][28][29][72,73,74,75,76,77,78].
Figure 4. Instrumental assessment for feeding problems. Green boxes with dotted outlines depict advantages; red boxes with dashed outlines depict disadvantages. (EGD: esophagogastroduodenoscopy, FEES: fiberoptic endoscopic evaluation of swallowing, GER: gastroesophageal reflux, LES: lower esophageal sphincter, pH-MII: pH monitoring multichannel impedance, UES: upper esophageal sphincter, VFSS: videofluoroscopic swallow study, UGI: Upper Gastrointestinal Fluoroscopy).
4.4. Pharmacological Interventions
Pharmacological interventions are often the last resort in the neonatal period and are frequently limited to treating GER symptoms. The role of anti-acids is limited and recommended to treat GER only after optimizing non-pharmacological measures, including thickening feeds, modifying feeding volume and frequency, and positional therapy
[30][85]. The American Academy of Pediatrics Committee of Fetus and Newborn clinical report on GER recommends using pharmacological interventions sparingly in neonates due to limited evidence and risk of potential harm with gastric acid blockade
[30][85]. However, in older infants, GER tends to be a significant concern as the immaturity-related sucking–swallowing incoordination improves. The pediatric GER clinical practice guidelines from the NASPGHAN recommend using a 4–8-week course of either histamine receptor antagonists (H2RA) such as Famotidine or proton pump inhibitors such as Omeprazole or Lansoprazole (if H2RAs are unavailable or contraindicated) to treat reflux-related erosive esophagitis in infants and do not recommend their use in treating crying, distress, or visible regurgitation in otherwise healthy infants
[26][75].
Motility agents such as erythromycin have been used in severe cases of feeding intolerance with dysmotility. Erythromycin is not recommended in preterm infants <32 weeks
[31][86], while its role >32 weeks for feeding intolerance is debated with mixed results in previous studies
[32][33][87,88]. Additionally, the adverse effects of erythromycin include alteration of the gut microbiome, antibiotic resistance, and infantile hypertrophic pyloric stenosis
[34][89]. Overall, given the limited evidence and adverse effect profile, the benefits and risks of using erythromycin should be carefully weighed and discussed with parents or caregivers before using erythromycin. Cyproheptadine, a histamine H1 and serotonin 5HT2 antagonist is another medication used in refractory feeding problems in children as it increases appetite, weight, and height; acceptance to more food varieties; and improved self-feeding
[35][36][90,91]. The use of these medications is reserved for infants with severe aversion and failure to thrive.
5. Future Directions
Feeding problems encompass diverse interlinked etiologies often grouped together. There is an urgent need to subcategorize feeding problems based on underlying etiology to provide targeted diagnostic and therapeutic support. The diagnosis of dysphagia is limited by available techniques and expertise, and, when diagnosed, there are few reliable treatment options in this delicate population. Parents and caregivers are often frustrated with a lack of a quick fix for feeding problems in infancy. Nevertheless, with patience and perseverance, many interventions show results in due time with delayed gratification. A multidisciplinary team approach to feeding in the NICU with established algorithms for early oral motor stimulation, initiation, and advancement of oral feeds using quality improvement methodologies is vital for the mitigation of future feeding problems
[37][92]. Furthermore, predicting feeding problems in infants based on risk factors, instrumental assessments, and novel technologies such as salivary transcriptomics
[11][19] can potentially target interventions before feeding problems become overtly apparent. Research in this area with large-scale, randomized control trials is highly warranted.
Additionally, as more preterm infants survive into adulthood, the long-term effects and healthcare costs of feeding problems are also expected to increase tremendously in the coming decades
[38][4]. Standardizing definitions for feeding problems is vital to understanding the future prevalence of feeding problems in adults born preterm. Management strategies should consider equitable access to investigations, treatments, services following hospital discharge, and continued care of infants and children with feeding problems, as this is a particular concern for lower socioeconomic status groups
[39][2]. More research is warranted to study the impact of social determinants such as race, ethnicity, and socioeconomic status on feeding problems in adults born preterm.