1. Introduction
Chronic kidney disease (CKD) is a highly prevalent disease. Prevalence of renal insufficiency (i.e., CKD Stages 3–5) in Germany is about 10% in a population aged ≥40 years which is comparable to the prevalence of coronary heart disease, diabetes or depression
[1][2][3][4][1,2,3,4]. However, CKD is widely unrecognized in its relevance for personal health consequences and its impact on societal health systems’ spending. CKD can lead to terminal renal failure (end stage renal disease, ESRD) which affects about 90,000 patients in Germany. Costs for renal replacement therapy as consequence of ESRD, such as dialysis and renal transplantation, are disproportionally high
[1][5][6][1,5,6]. Moreover, CKD is associated with a higher risk for non-renal health outcomes such as cardiovascular diseases, hospitalizations, cognitive decline and premature mortality
[5]. Kidney function is assessed by the estimated glomerular filtration rate (eGFR) using equations that incorporate serum creatinine, sex, age and race such as the CKD-Epi, Equation
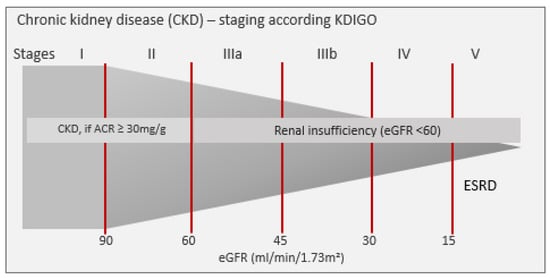
[7]. According to the Kidney Disease Improving Global Outcomes (KDIGO) Guideline, CKD is staged (Stages I to V) using cut points of eGFR and albuminuria (
Figure 1). Patients with CKD Stage 5 (=eGFR < 15 mL/min/1.73 m
2, (ESRD)) require renal replacement therapy.
Figure 1. CKD staging according to decreasing renal function defined by albuminuria and estimated glomerular filtration rate (eGFR). ACR = albumin/creatinine ratio, CVD = cardiovascular disease, ESRD = end stage renal disease, KDIGO = Kidney Disease Improving Global Outcomes (=Guideline).
Timely start of treatment and monitoring of CKD risk factors such as hypertension can decelerate the decrease of renal function
[8]. CKD remains asymptomatic throughout a long time leading to late diagnosis in advanced stages defined by severely reduced renal function. Regarding renal insufficiency in elderly patients, discussions in the medical community whether a decline of renal function in older age should be regarded as normal physiologic aging process or be labelled as ‘disease’ are still ongoing
[9].
Contrasting to diseases similarly prevalent as coronary heart disease or diabetes, for CKD, a high public and patient unawareness has been reported: unawareness was about 80% in early stages, and about 30% in later stages in populations from USA, Australia or Taiwan
[10], even in patients with markers for renal dysfunction
[11]. In the German Health Interview and Examination Survey for Adults (DEGS), 72% of participants—drawn from the general population—with a decreased renal function (defined as eGFR < 60 mL/min/1.73 m
2), did not know about their condition
[12]. CKD unawareness was even high in German patients hospitalized due to cardiovascular diseases
[13]. Public knowledge about CKD is scarce
[14]. Screening for CKD among patients and populations at higher risk was shown to be cost-effective
[15], but is lacking on routine basis —resulting in late diagnosis and delayed treatment. Although eGFR should be calculated and printed automatically on patients’ laboratory reports that include measurement of serum creatinine, this seems not to lead to a routine ascertainment of kidney function and diagnosis of CKD. Physician–patient communication about CKD and its relevance for health seems to be more difficult in CKD than in other chronic diseases with negative impact on patients’ involvement and compliance to treatment
[16][17][16,17].
CKD unawareness can result from either not yet being diagnosed or not being told about by a physician or not fully grasp the meaning of CKD information.
We wanted to estimate CKD unawareness focusing on patients with CKD related risk factors, as these patients can be expected to be targeted in primary health care for monitoring renal function according to guidelines. Among these patients, we wanted to identify demographic and clinical factors that are associated with low CKD awareness.
2. Current Insights
In a population of patients with high prevalence of CKD risk factors, CKD unawareness was 80% in early CKD Stages 1 and 2 and still about 30% in patients with CKD Stage 4. Unawareness for CKD was seen even in the elderly or patients with hypertension or diabetes. In these patients, guidelines for treatment and drug prescribing recommend a routine monitoring of renal function. Therefore, the extent of CKD unawareness was unexpected in these subgroups and may reflect a low adherence or knowledge of guidelines. A gender gap in CKD awareness with a higher unawareness in women increased distinctly with increasing stages of CKD and was visible independently of other CKD risk factors.
2.1. Unawareness in Patients, Physicians and Public
Information on CKD awareness was derived from the participants’ answer to the question whether they had ever been told by their physician that they had a renal disease or kidney stones. Therefore, patients’ unawareness could either derive from a lack of understanding of the physicians’ information about their CKD or from their physicians’ unawareness of their CKD. Wagner et al. showed that hospital patients’ informational status regarding a prevalent CKD directly depended on physicians awareness
[13].
In 2009, in a report on the prevalence of patients with chronic diseases in general practice, the authoring physicians did not select CKD as one of 20 relevant diseases and conditions
[18][24], although CKD prevalence in this setting is estimated to be about 30%
[19][25]. Guidelines on treatment of hypertension or diabetes are much more familiar in general practice than those dealing with CKD
[20][26]. It has been shown that interventions to increase CKD knowledge and awareness in primary care physicians can lead to better CKD diagnoses and risk factor management
[21][27].
In about 80% of the records of patients in general practice
[22][28] and in hospitalized patients due to cardiovascular events
[13], a prevalent CKD was not mentioned in their record, less so in patients with diabetes or obese patients. Even patients treated for CKD are often unaware. In patients from a nephrological outpatient clinic, unawareness of CKD Stage 1 or 2 was 40%, and in later stages about 12%
[23][29]. In UK, 41% of patients with CKD Stage 3 that are documented in their GPs CKD registry were unaware of their disease
[24][30].
The high CKD unawareness in patients at higher age (≥70 years) is disturbing. Age-related physiological changes in pharmacodynamics along with decreasing glomerular filtration require renal monitoring and adjustment of prescription and dosing of drugs. About 90% of the older patients in our study reported intake of antihypertensive medication. Therefore, they should regularly visit their GP. In our cohort, with increasing age, in CKD Stages 3b and 4 unawareness increased also. Physicians seem reluctant to disclose CKD related laboratory findings to their patients. As it is still discussed when to define CKD as a ‘disease’ in the elderly
[9], physicians do not want to alarm their patients needlessly, when CKD is still not causing any trouble and worry about over-medicalization. However, an eGFR < 30 mL/min/1.73 m
2 defining CKD Stage 4 should be generally regarded as pathologic. On the other hand, if physicians inform their patients about a renal dysfunction, patients may not grasp the meaning and impact it has on their health
[25][31]. Cognitive decline which has found to be linked to CKD might negatively affect patients’ awareness
[26][32]. However, in an analysis of primary care encounters, CKD was less often discussed than other conditions and information about CKD was given mostly about technical details as laboratory values
[17][27][17,33], although better health information facilitates success in patients’ adherence to treatments
[16][28][16,34].
2.2. CKD Unawareness and Additional CKD Related Risk Factors
In our cohort, in 97% of all patients, at least one condition was present which should prompt screening of renal function. However, even patients already treated or with diagnostic markers for CKD were often unaware. Albuminuria as marker for CKD seem to trigger renal screening, as unawareness was lower in these patients in our—as well as in other—cohorts
[11].
Diabetes, hypertension or cardiovascular diseases were more prevalent in our cohort than in CKD patients in general
[29][35]. Diabetic patients are at higher risk for diabetic nephropathy or other renal function disorders. Known diabetes as well as hypertension should trigger monitoring renal function. Nonetheless, unawareness was about 70% in diabetic or hypertensive patients with CKD Stage 3a and 50% in CKD Stage 3b. A German study found a similar CKD unawareness in patients with coronary heart disease
[13]. US studies reported even higher CKD unawareness in patients with diabetes or hypertension
[30][36]. In our data, still 36% of patients with diabetes and CKD Stage 4 were unaware of their CKD. A finding that is difficult to explain, as metformin, an anti-diabetic drug, is contraindicated in CKD Stage 4.
2.3. Unawareness and High Risk of Renal Failure
In our cohort, 21% of patients with a risk for renal failure within five years ≥15% according to the KFRE risk score were not informed about the critical state of their disease. These patients might lack necessary time for preparation for renal replacement options. In patients from NHANES with CKD Stages 3–4, unawareness was even higher among those with a KFRE risk of ≥15% (50%)
[31][37].
2.4. Gender Gap in CKD Awareness
The gender gap in CKD awareness was unexpected, especially the strong increase with decreasing renal function. As unawareness for CKD in higher stages can be associated with higher probability of non-treatment or non-adherence to a treatment, women will have a higher risk for CKD-related adverse health outcomes such as cardiovascular diseases, hospitalizations, and premature mortality. In 187 participants with CKD from a German population, sex differences in CKD awareness were not visible
[12]. A recent analysis of NHANES data found a higher CKD unawareness in women compared to men, but only in the Caucasian participants. Sex differences were smaller than in our cohort
[32][38]. It is difficult to explain why women are more often unaware about a potentially critical CKD stage. Women were similarly affected by comorbidities which should require renal monitoring by a physician. Then, they would be informed about a CKD in the same manner as men. Women have been shown to be more interested in health and are more actively seeking health-related information than men
[33][39]. Men, independent of educational attainment, are less engaged in healthy lifestyles than women
[34][40], including exhibiting less proactive and preventive behavior
[35][41]. Sex differences in treatment and disease outcome could be related to physicians’ bias and unconscious attitudes towards female and male patients
[36][42].