Non-melanoma skin cancers (NMSC) are the most common type of skin malignancies among humans (particularly fair-skinned populations of European descent) and its incidence rates have been on the rise globally for decades [1]. The best defined role of vitamin D in humans is in supporting the normal development and maintenance of bone tissues and in regulating calcium metabolism [7,8]. Furthermore, there is growing evidence that vitamin D plays a role in many fundamental biological processes (e.g., cell proliferation, angiogenesis, and modulation of the immune system) [9] implicated in carcinogenesis.
- vitamin D
- dietary intake
- blood concentration
- gene polymorphism
- vitamin D receptor
- vitamin D binding protein
- non-melanoma skin cancer
- basal cell cancer
- squamous cell cancer
- risk
1. Introduction
2. Vitamin D and Non-Melanoma Skin Cancer
2.1. Vitamin D Blood Concentration and NMSC Risk
2. Vitamin D and Non-Melanoma Skin Cancer
2.1. Vitamin D Blood Concentration and NMSC Risk
Ten studies reported a RR estimate comparing NMSC risk among those in the highest vs. lowest category of serum/plasma 25(OH)D concentration (Table 1) [10,11,12,13,14,15,16,17,18,19][10][11][12][13][14][15][16][17][18][19]. Of these, five were conducted in the USA, two in Denmark, and one each in Australia, Brazil, and Poland. In terms of study design, three were case-control studies [13,17,19][13][17][19], two were nested case-control studies [10[10][11],11], and five were cohort studies [12,14,15,16,18][12][14][15][16][18]. The ten studies encompassed a total of 3899 NMSC cases, of which 1569 (40.2%) were contributed by Winsløw et al. [18]. Vitamin D concentration was measured in serum in all studies except in Liang et al. [14]. The studies differed greatly both in the categories that were used to calculate the RR for the highest vs. lowest vitamin D concentration comparison, and in the degree of statistical adjustment. In particular, for three studies an unadjusted OR was calculated using data provided in the paper [13,17,19][13][17][19].
2.2. Vitamin D Dietary Intake and Supplements Use and NMSC Risk
2.2. Vitamin D Dietary Intake and Supplements Use and NMSC Risk
| Author, Year | Country | Study Design | Skin Cancer Type | N Cases | N Controls/Cohort Size | % Males | Age at NMSC (yrs) | Years of Diagnosis | Exposure | Comparison | RR | 95% CI | Adjusting Variables |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Davies, 2002 [20 |
| Author, Year | Country | Study Design | Skin Cancer Type | N Cases | N Controls | VDR Polymorphisms | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Apa1 | Fok1 | Bsm1 | Cdx2 | Taq1 | ||||||||||||||||
| ] | UK | NCC | BCC | 109 | 247 | 52.3% | mean 66, range 46–79 | 1993–1998 | intake from food | linear increase by 2.08 microg/d | 1.07 | 0.84–1.35 | ||||||||
| Han, 2007 [30] | USA | NCC | BCC | 295 | age, sex, phenotype, other | |||||||||||||||
| 853 | x | x | x | Asgari, 2011 [21] | USA | CC | SCC | 415 | 415 | 61.9% | mean 72.5, range 43–85 | 2004 | supplement use ≥3 months in the past 10 years | any vs. none | 0.78 | 0.46–1.32 | age, sex, phenotype, other | |||
| SCC | 281 | x | x | x | Tang, 2011 [22] (a) | USA | RCT | NMSC | 3338 | 36,282 | 0.0% | ns | 1995 | 200 IU twice daily (intervention arm) | supplementation vs. placebo | 1.02 | 0.95–1.07 | age | ||
| Park, 2016 [23] (b) | USA | cohort | BCC | 20,840 | 109,290 | 38.0% | ||||||||||||||
| Lesiak, 2011 [13] | Poland | hCC | BCC | 142 | 142 | x | x | x | x | ns | 1984–2010 | intake from food + supplements | 5th vs. 1st quintile | 1.10 | 1.05–1.15 | age, sex, phenotype, phototype, UV exposure, other | ||||
| Köstner, 2012 [31] | Germany | hCC | BCC | 87 | 50 | SCC | 2329 | 1.02 | 0.89–1.17 | |||||||||||
| Passarelli, 2020 | USA | RCT | BCC | 200 | 2259 | 63.0% | ns | 2004–2016 | 1000 IU/day (intervention arm) | supplementation vs. placebo | 0.96 | 0.73–1.26 | age, sex, UV exposure, other | |||||||
| SCC | 68 | 0.79 | 0.49–1.27 | |||||||||||||||||
2.3. VDR and VDBP Genes Polymorphisms and NMSC Risk
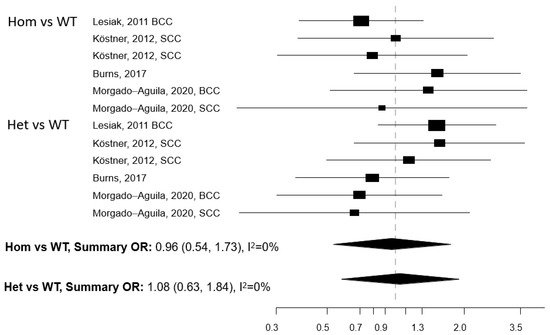
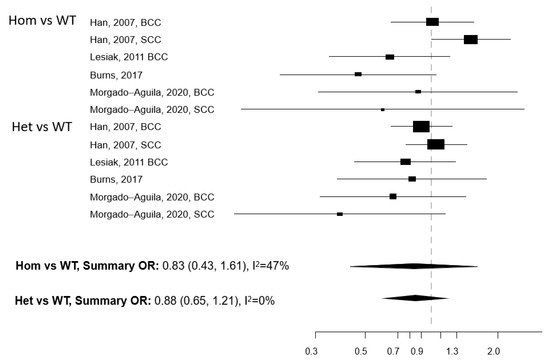
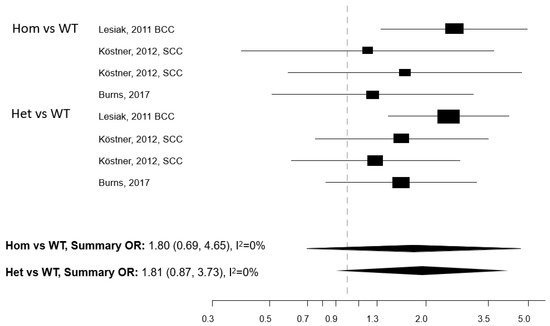
Five papers reported on the association between any of five polymorphisms of the VDR gene (Apa1, Bsm1, Cdx2, Fok1, and Taq1) and NMSC risk [13][25][26][27][28]. The studies were conducted in the USA (n = 2) and Europe (n = 3) (2.3. VDR and VDBP Genes Polymorphisms and NMSC Risk
Five papers reported on the association between any of five polymorphisms of the VDR gene (Apa1, Bsm1, Cdx2| Author, Year | Country | Study Design | Skin Cancer Type | N Cases | N Controls/Cohort Size | % Males | Age at NMSC (yrs) | Years of Diagnosis | Exposure | Comparison | RR | 95% CI | Adjusting Variables |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Asgari, 2010 [10] | USA | NCC | BCC | 220 | 220 | 51.8% | mean 54.9, range 28–78 | 1968–1989 | serum 25(OH)D | 5th vs. 1st quintile (>29.8 vs. <14.7 ng/mL) | 2.09 | 0.95–4.58 | age, sex, season of sampling, phenotype, UV exposure, other |
| Skelsey, 2010 [19] (a) (b) | USA | CC | KSC | 50 | 14 | ns | range 18–65 | ns | serum 25(OH)D | ≥30 vs. <30 ng/ml | 0.16 | 0.004–1.30 | none (c) |
| Tang, 2010 [11] | USA | NCC | NMSC | 178 | 930 | 100.0% | mean 73.6 | 2000–2007 | serum 25(OH)D | 5th vs. 1st quintile (≥29.9 vs. <16 ng/mL) | 0.54 | 0.31–0.96 | age, season of sampling, other |
| Eide, 2011 [12] | USA | cohort | KSC | 240 | 3223 | 10.7% | ns | 1997–2009 | serum 25(OH)D | 4th vs. 1st quartile (≥31 vs. <19 ng/mL) | 1.6 | 1.1–2.3 | age, sex |
| Lesiak, 2011 [13] | Poland | CC | BCC | 142 | 142 | 50.0% | mean 56, range 45–78 | 2007–2008 | serum 25(OH)D | >30 vs. <20 ng/ml | 0.18 | 0.08–0.37 | none (c) |
| Liang, 2012 [14] | USA | cohort | BCC | 510 | 4641 | 0.0% | ns | 1976–2008 | plasma 25(OH)D | 4th vs. 1st quartile | 2.07 | 1.52–2.80 | age, season of sampling, UV exposure, phenotype, phototype, other |
| SCC | 75 | 3.77 | 1.70–8.36 | ||||||||||
| van der Pols, 2013 [15] | Australia | cohort | BCC | 300 | 1191 | 50.0% | mean 58 | 1996–2007 | serum 25(OH)D | ≥75 vs. <75 nmol/L | 1.51 | 1.10–2.07 | age, sex, UV exposure, phenotype, phototype, other |
| SCC | 176 | 56.0% | mean 63 | ≥75 vs. <75 nmol/L | 0.67 | 0.44–1.03 | |||||||
| Skaaby, 2014 [16] | Denmark | cohort | NMSC | 398 | 12,204 | 48.1% | ns | 1993–2011 | serum 25(OH)D | 4th vs. 1st quartile | 1.43 | 1.05–1.93 | age, sex, season of sampling, other |
| Soares, 2018 [17] (b) | Brazil | CC | KSC | 41 | 200 | 56.1% | mean 67, range 21–87 | 2016–2017 | serum 25(OH)D | ≥30 vs. <20 ng/ml | 50.00 | 11.11–100.0 | none (c) |
| Winsløw, 2018 [18] | Denmark | cohort | NMSC | 1569 | 35,298 | 43.0% | ns | 1981–2012 | plasma 25(OH)D | ≥50 vs. <25 nmol/L | 3.76 | 2.58–5.48 | age, sex, season of sampling, other |
A single study that considered polymorphisms in the VDBP gene and NMSC risk [33][29]. The study relied on 7983 participants, of which 235 developed BCC during follow-up. BCC was not associated with the two polymorphisms of the VDBP gene (rs7041 and rs4588) that were investigated, despite some limited evidence of an age-specific effect.
3. Conclusions
References
- Apalla, Z.; Lallas, A.; Sotiriou, E.; Lazaridou, E.; Ioannides, D. Epidemiological trends in skin cancer. Dermatol. Pract. Concept. 2017, 7, 1–6.
- Mudigonda, T.; Pearce, D.J.; Yentzer, B.A.; Williford, P.; Feldman, S.R. The economic impact of non-melanoma skin cancer: A review. J. Natl. Compr. Cancer Netw. 2010, 8, 888–896.
- Savoye, I.; Olsen, C.M.; Whiteman, D.C.; Bijon, A.; Wald, L.; Dartois, L.; Clavel-Chapelon, F.; Boutron-Ruault, M.C.; Kvaskoff, M. Patterns of Ultraviolet Radiation Exposure and Skin Cancer Risk: The E3N-SunExp Study. J. Epidemiol. 2018, 28, 27–33.
- Belbasis, L.; Stefanaki, I.; Stratigos, A.J.; Evangelou, E. Non-genetic risk factors for cutaneous melanoma and keratinocyte skin cancers: An umbrella review of meta-analyses. J. Dermatol. Sci. 2016, 84, 330–339.
- Gandini, S.; Palli, D.; Spadola, G.; Bendinelli, B.; Cocorocchio, E.; Stanganelli, I.; Miligi, L.; Masala, G.; Caini, S. Anti-hypertensive drugs and skin cancer risk: A review of the literature and meta-analysis. Crit. Rev. Oncol. Hematol. 2018, 122, 1–9.
- Dominguez, L.J.; Farruggia, M.; Veronese, N.; Barbagallo, M. Vitamin D Sources, Metabolism, and Deficiency: Available Compounds and Guidelines for Its Treatment. Metabolites 2021, 11, 255.
- Bikle, D.D. Vitamin D and bone. Curr. Osteoporos. Rep. 2012, 10, 151–159.
- Khammissa, R.A.G.; Fourie, J.; Motswaledi, M.H.; Ballyram, R.; Lemmer, J.; Feller, L. The Biological Activities of Vitamin D and Its Receptor in Relation to Calcium and Bone Homeostasis, Cancer, Immune and Cardiovascular Systems, Skin Biology, and Oral Health. Biomed. Res. Int. 2018, 2018, 9276380.
- Toner, C.D.; Davis, C.D.; Milner, J.A. The vitamin D and cancer conundrum: Aiming at a moving target. J. Am. Diet. Assoc. 2010, 110, 1492–1500.
- Asgari, M.M.; Tang, J.; Warton, M.E.; Chren, M.M.; Quesenberry, C.P., Jr.; Bikle, D.; Horst, R.L.; Orentreich, N.; Vogelman, J.H.; Friedman, G.D. Association of prediagnostic serum vitamin D levels with the development of basal cell carcinoma. J. Invest. Dermatol. 2010, 130, 1438–1443.
- Tang, J.Y.; Parimi, N.; Wu, A.; Boscardin, W.J.; Shikany, J.M.; Chren, M.M.; Cummings, S.R.; Epstein, E.H., Jr.; Bauer, D.C.; Osteoporotic Fractures in Men (MrOS) Study Group. Inverse association between serum 25(OH) vitamin D levels and non-melanoma skin cancer in elderly men. Cancer Causes Control 2010, 21, 387–391.
- Eide, M.J.; Johnson, D.A.; Jacobsen, G.R.; Krajenta, R.J.; Rao, D.S.; Lim, H.W.; Johnson, C.C. Vitamin D and nonmelanoma skin cancer in a health maintenance organization cohort. Arch. Dermatol. 2011, 147, 1379–1384.
- Lesiak, A.; Norval, M.; Wodz-Naskiewicz, K.; Pawliczak, R.; Rogowski-Tylman, M.; Sysa-Jedrzejowska, A.; Sobjanek, M.; Wlodarkiewicz, A.; Narbutt, J. An enhanced risk of basal cell carcinoma is associated with particular polymorphisms in the VDR and MTHFR genes. Exp. Dermatol. 2011, 20, 800–804.
- Liang, G.; Nan, H.; Qureshi, A.A.; Han, J. Pre-diagnostic plasma 25-hydroxyvitamin D levels and risk of non-melanoma skin cancer in women. PLoS ONE 2012, 7, e35211.
- Van der Pols, J.C.; Russell, A.; Bauer, U.; Neale, R.E.; Kimlin, M.G.; Green, A.C. Vitamin D status and skin cancer risk independent of time outdoors: 11-year prospective study in an Australian community. J. Invest. Dermatol. 2013, 133, 637–641.
- Skaaby, T.; Husemoen, L.L.; Thuesen, B.H.; Pisinger, C.; Jørgensen, T.; Roswall, N.; Larsen, S.C.; Linneberg, A. Prospective population-based study of the association between serum 25-hydroxyvitamin-D levels and the incidence of specific types of cancer. Cancer. Epidemiol. Biomarkers. Prev. 2014, 23, 1220–1229.
- Soares, A.M.; Szejnfeld, V.L.; Enokihara, M.Y.; Michalany, N.; Castro, C.H. High serum 25-hydroxyvitamin D concentration in patients with a recent diagnosis of non-melanoma skin cancer: A case-control study. Eur. J. Dermatol. 2018, 28, 649–653.
- Winsløw, U.C.; Nordestgaard, B.G.; Afzal, S. High plasma 25-hydroxyvitamin D and high risk of nonmelanoma skin cancer: A Mendelian randomization study of 97 849 individuals. Br. J. Dermatol. 2018, 178, 1388–1395.
- Skelsey, M.; Janicic, N.; Mendu, R.; Moshell, A.; Colombo, M.; Soldin, S. Hypovitaminosis D and non-melanoma skin cancer. Conference: Annual Meeting of the Society for Investigative Dermatology. Atlanta, Georgia, 5–8 May 2010. J. Invest. Dermatol. 2010, 130, S25.
- Davies, T.W.; Treasure, F.P.; Welch, A.A.; Day, N.E. Diet and basal cell skin cancer: Results from the EPIC-Norfolk cohort. Br. J. Dermatol. 2002, 146, 1017–1022.
- Asgari, M.M.; Chren, M.M.; Warton, E.M.; Friedman, G.D.; White, E. Supplement use and risk of cutaneous squamous cell carcinoma. J. Am. Acad. Dermatol. 2011, 65, 1145–1151.
- Tang, J.Y.; Fu, T.; Leblanc, E.; Manson, J.E.; Feldman, D.; Linos, E.; Vitolins, M.Z.; Zeitouni, N.C.; Larson, J.; Stefanick, M.L. Calcium plus vitamin D supplementation and the risk of nonmelanoma and melanoma skin cancer: Post hoc analyses of the women’s health initiative randomized controlled trial. J. Clin. Oncol. 2011, 29, 3078–3084.
- Park, S.M.; Li, T.; Wu, S.; Li, W.Q.; Qureshi, A.A.; Cho, E. Vitamin D Intake and Risk of Skin Cancer in US Women and Men. PLoS ONE 2016, 11, e0160308.
- Passarelli, M.N.; Karagas, M.R.; Mott, L.A.; Rees, J.R.; Barry, E.L.; Baron, J.A. Risk of keratinocyte carcinomas with vitamin D and calcium supplementation: A secondary analysis of a randomized clinical trial. Am. J. Clin. Nutr. 2020, 112, 1532–1539.
- Burns, E.M.; Guroji, P.; Ahmad, I.; Nasr, H.M.; Wang, Y.; Tamimi, I.A.; Stiefel, E.; Abdelgawwad, M.S.; Shaheen, A.; Muzaffar, A.F.; et al. Association of Vitamin D Receptor Polymorphisms With the Risk of Nonmelanoma Skin Cancer in Adults. JAMA Dermatol. 2017, 153, 983–989.
- Han, J.; Colditz, G.A.; Hunter, D.J. Polymorphisms in the MTHFR and VDR genes and skin cancer risk. Carcinogenesis 2007, 28, 390–397.
- Köstner, K.; Denzer, N.; Koreng, M.; Reichrath, S.; Gräber, S.; Klein, R.; Tilgen, W.; Vogt, T.; Reichrath, J. Association of genetic variants of the vitamin D receptor (VDR) with cutaneous squamous cell carcinomas (SCC) and basal cell carcinomas (BCC): A pilot study in a German population. Anticancer. Res. 2012, 32, 327–333.
- Morgado-Águila, C.; Rey-Sánchez, P.; Gil-Fernández, G.; Costa-Fernández, M.C.; Rodríguez-Velasco, F.J. Vitamin D Receptor Polymorphisms and Non-Melanoma Skin Cancer Risk: A Case-Control Study. J. Clin. Med. 2020, 9, 3819.
- Flohil, S.C.; de Vries, E.; van Meurs, J.B.; Fang, Y.; Stricker, B.H.; Uitterlinden, A.G.; Nijsten, T. Vitamin D-binding protein polymorphisms are not associated with development of (multiple) basal cell carcinomas. Exp. Dermatol. 2010, 19, 1103–1105.
- Zhang, X.; Niu, W. Meta-analysis of randomized controlled trials on vitamin D supplement and cancer incidence and mortality. Biosci. Rep. 2019, 39, BSR20190369.
- Boughanem, H.; Canudas, S.; Hernandez-Alonso, P.; Becerra-Tomás, N.; Babio, N.; Salas-Salvadó, J.; Macias-Gonzalez, M. Vitamin D Intake and the Risk of Colorectal Cancer: An Updated Meta-Analysis and Systematic Review of Case-Control and Prospective Cohort Studies. Cancers 2021, 13, 2814.
- Sun, K.; Zuo, M.; Zhang, Q.; Wang, K.; Huang, D.; Zhang, H. Anti-Tumor Effect of Vitamin D Combined with Calcium on Lung Cancer: A Systematic Review and Meta-Analysis. Nutr. Cancer 2020, 1–10.
- Gnagnarella, P.; Raimondi, S.; Aristarco, V.; Johansson, H.; Bellerba, F.; Corso, F.; De Angelis, S.P.; Belloni, P.; Caini, S.; Gandini, S. Ethnicity as modifier of risk for Vitamin D receptors polymorphisms: Comprehensive meta-analysis of all cancer sites. Crit. Rev. Oncol. Hematol. 2021, 158, 103202.