Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Anna Yordanova and Version 2 by Vivi Li.
Peptide receptor radionuclide therapy (PRRT) is a successful targeted radionuclide therapy in neuroendocrine tumors (NETs). However, complete responses remain elusive. Combined treatments anticipate synergistic effects and thus better responses by combining ionizing radiation with other anti-tumor treatments. Furthermore, multimodal therapies often have a balanced toxicity profile. To date, few studies have evaluated the effect of combination therapies with PRRT, some of them phase I/II trials.
- PRRT
- NET
- combination therapies
- personalized medicine
- somatostatin analogues
- chemotherapy
- molecular targeted treatment
- liver radioembolization
- Lutetium-177
- Yttrium-90
1. Introduction
Neuroendocrine tumors (NETs) are heterogeneous neoplasia that are often diagnosed in the metastasized stage (range 40 to 76%), making them challenging to manage [1][2][3][1,2,3]. Guideline-oriented treatment options normally target only one specific pathway of the cell cycle. Such options are not always suitable for heterogeneous clones and can eventually result in treatment resistance [4][5][6][4,5,6].
Peptide receptor radionuclide therapy (PRRT) is proven to be an effective and safe treatment (EMA 2017 and FDA 2018 approved) that significantly prolongs survival and improves quality of life. However, according to prospective phase III study data, it has a limited response rate of only 18% [7][8][9][7,8,9]. Furthermore, since PPRT is not a curative treatment, patients eventually relapse. If recurrent tumors still have adequate somatostatin receptor (SSTR) expression, there is a good chance that salvage PRRT [10][11][10,11] will be beneficial. On the contrary, dedifferentiated NETs with loss of SSTR expression have a poor outcome with short survival following monotherapy [12]. Thus, combined treatment is a promising option for targeting heterogeneous tumors and avoiding accumulated toxicity. However, the data on combined treatment is still limited.
This review summarizes current data from clinically proven combination treatments with PRRT and aims to help physicians choose a tailored treatment approach for patients with NETs. Combination partners with possible synergistic therapeutic effects seem to be dual-PRRT radiolabeling, liver radioembolization, “non-radiolabeled” somatostatin analogues (SSAs), chemotherapy (e.g., capecitabine/temozolomide), molecular targeted treatment (e.g., everolimus), [131I]I-metaiodobenzylguanidine (MIBG), and external beam radiotherapy (EBRT).
Combination Treatment Decision Making
As represented in Figure 1, before starting a treatment, physicians should not only prioritize maximizing tumor response and patient survival but also minimize adverse events and patient morbidity. Substantial factors to consider in this decision-making are the age and health condition of the patient; genetic factors, tumor characteristics such as the origin, localization, size, and immunohistochemical proliferation marker Ki67; and tumor uptake in molecular imaging such as SSTR-positron emission tomography (PET) and [18F]F-Fluorodeoxyglucose (FDG). Furthermore, an institution’s access to multidisciplinary medical care and medical center experience are important features for treatment planning [13][14][15][13,14,15]. Figure 2 represents the various antitumor effects of combination partners of PRRT. The objective response rates, PFS, OS and adverse events of combination partners of PRRT are listed in Table 1.
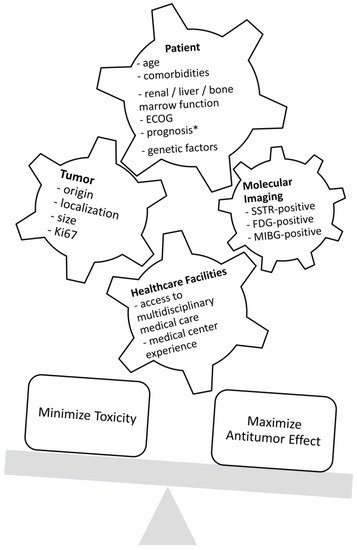
Figure 1. Factors that influence decision-making regarding treatment. ECOG = Eastern Cooperative Oncology Group Performance Status; SSTR = somatostatin receptor; FDG = fluorodeoxyglucose; MIBG = metaiodobenzylguanidine; * life expectancy of at least 3 months.
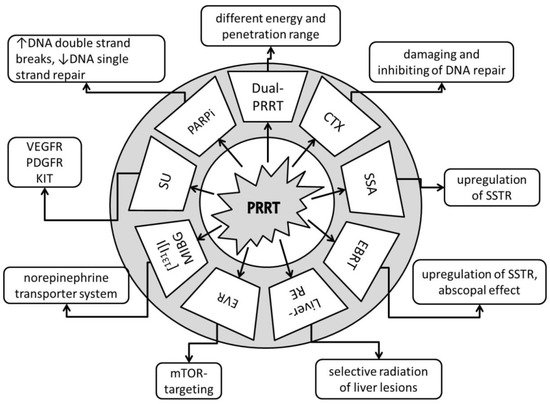
Figure 2. Anti-tumor effects of combination partners of PRRT. Dual-PRRT = dual-radionuclide peptide receptor therapy: a combination of different energy and penetration range levels to better target metastatic lesions with different sizes and nonhomogeneous somatostatin receptor (SSTR) distributions [16][17][19,20]. CTX = chemotherapy: damaging and inhibiting DNA repair, cell proliferation arrest, tumor cell reoxygenation, and synchronization of the cell cycle or apoptosis [18][21]. SSA = somatostatin receptor analogues: upregulation of SSTR, increasing number of targets for PRRT [19][22]. EBRT = fractionated external beam radiotherapy: upregulation of SSTR, increasing number of targets for PRRT, potential abscopal effect with triggering of immuno-mediated antitumor effects [20][21][23,24]. Liver-RE = liver radioembolization: selective radiation of liver tumor lesions; potential abscopal effect with triggering of immuno-mediated antitumor effects [22][23][25,26]. EVR = everolimus: targets the mammalian target of rapamycin (mTOR), with growth-inhibitory and anti-angeogenic effects [24][25][27,28]. [131I]I-MIBG = [131I]I-metaiodobenzylguanidine: targets the norepinephrine transporter system [26][29]. SU = sunitinib: tumor growth arrest via targeting of the vascular endothelial growth factor receptor (VEGFR), platelet-derived growth factor (PDGFR), and receptor tyrosine kinase KIT [27][30]. PARPi = poly (ADP-ribose) polymerase-1 inhibitors: increases DNA double-strand breaks; blocks DNA single-strand repair [28][31].
Table 1. Efficacy and safety of combination treatment with PRRT.
| Combination Partner | ORR (%) | OS (Month) |
PFS (Month) |
SAE (%) | Ref |
|---|---|---|---|---|---|
| Dual PRRT Lu-177 and Y-90 | 42 | 66–127 | - | 2% MDS, 2% nephrotoxicity, 7% hematotoxicity |
[17][29][30][31][32][33][34][20,32,33,34,35,36,37] |
| Capecitabine | 24–30 | not reached | 31 | <15% anemia/thrombocytopenia/neutropenia 5% fatigue/diarrhea |
[35][36][37][38,39,40] |
| CAPTEM | 53–70 | not reached | 22–48 | 6% neutropenia, 3% nausea | [38][39][40][41,42,43] |
| 5-fluorouracil | 25 | not reached | - | - | [41][44] |
| SSA | 37 | 91 | 48 | 3% hepatotoxicity | [42][43][45,46] |
| EBRT | 0 | not reached | 108 | 0% | [44][47] |
| Liver embolization | 16 (Y-90) 43 (Ho-166) |
42–68 | - | 10% abdominal pain, 3% fatigue/nausea, >20% lymphocytopenia, 5% radiation-induced gastric ulceration, 2% radiation pneumonitis, 2% liver abscess, 2% cholangitis, 50% liver enzyme elevation, <5% liver failure (2–3% fatal) |
[45][46][47][48,49,50] |
| Everolimus | 44 | not reached | not reached (63% at 24 months) | mainly hematotoxicity (thrombocytopenia, anemia) in the 10 mg/d everolimus dose group 100%, one case (6%) hepatotoxicity | [48][51] |
| [131I]I-MIBG | 0 | - | - | one case of three (33%) thrombocytopenia | [49][52] |
ORR = objective response rate; OS = overall survival; PFS = progression-free survival; SAE = serious adverse events according to CTCAE; Cave! In the table are listed collective SAE from different references. These SAE correlate only with the studied cohort in the particular investigation; Ref = references; MDS = myelodysplastic syndrome; CAPTEM = capecitabine and temozolomide; SSA = somatostatin receptor analogues; [131I]I-MIBG = [131I]I-metaiodobenzylguanidine; EBRT = fractionated external beam radiotherapy.
Dual-imaging SSTR-PET and FDG-PET can help clinicians plan individualized treatments [50][16]. Chan et al. developed a scoring system (NETPET grade) to distinguish between tumors with both SSTR- and FDG-positive lesions, only SSTR- or FDG-positive lesions, and both SSTR- and FDG-negative lesions. The NETPET grade is prognostic for survival and can help to determine which patients are likely to benefit from combination therapy, such as PRRT and chemotherapy [51][52][17,18].