CTCs as a potential biomarker of response to systemic therapies but also the technical challenges for their implementation in clinical practice, including the role of free circulating DNA and new approaches based on the isolation of CTCs from body fluids. New approaches focusing on isolation CTCs in other body fluids such as cerebrospinal or ascitic fluid are necessary to increase the opportunities of circulating tumor cells in the practice clinic as well as to study the promising role of CTC clusters and their prognostic value in metastatic breast cancer.
1. Introduction
The concept of tumor heterogeneity defines the existence at the same time of cellular subpopulations that differ from each other in their genetic and phenotypic characteristics, etc. This heterogeneity is also present between the primary tumor and its metastases. Among the causes that lead to this diversity are genetic and epigenetic factors and mechanisms such as adaptive responses, among others [1][6]. Techniques such as cytogenetic analysis, chromosomal analysis and microarray-based comparative genomic hybridization (CGH) have been used to demonstrate intra-tumor genetic heterogeneity in breast cancer [1][6]. Among the characteristics which conditionate the different subtypes, the expression of specific biomarkers, such as estrogen receptor (ER), progesterone receptor (PR) and human epidermal growth factor receptor 2—HER2, as well as different molecular profiles and tumor morphology are the most relevant [2][7]. Similarly, data suggest the existence of heterogeneity not only spatially (different subpopulations in different regions of the tumor) but also temporally (differences between the primary tumor and its recurrence) [1][6]. Thus, it should be taken into consideration that the sample obtained in a biopsy does not represent the totality of the composition of the tumor. The tumor is composed of different tumor cells that differ in their properties and drug resistance [2][7].
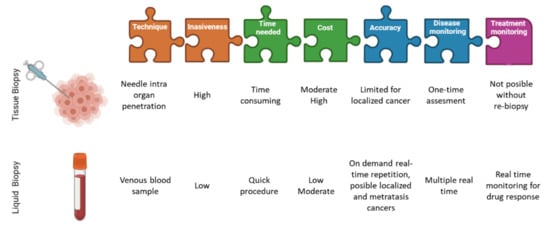
For this key reason, circulating tumor cells (CTCs) in peripheral blood provide the most objective way to assess intra tumor heterogeneity, facilitating the determination of single cell genotypes, cancer cell origin, differences among the CTCs and the solid tumor as well as those mutations which could address to the potential drug resistances ( Figure 1 ). Thus, the CTCs detection together with optimized analyses methods are very helpful in the clinic for determining intra tumor heterogeneity [2][7].
Figure 1. Differences between liquid biopsies and conventional tissue biopsies. Image partially created with BioRender.com and modified from Eslami-S et al.
[3][14].
TEPs are now considered to be local and systemic responders to the presence of cancer. They exert their effect both on tumor cells present in the tumor and on circulating tumor cells. Their mechanism of action is divided into several phases, first platelets generate an appropriate environment for neovascularization by providing the tumor with different proangiogenic factors such as VEGF, PDGF and FGF. Subsequently, platelets can induce epithelial-mesenchymal change in tumor cells by direct physical interaction and release of TGF molecules and have also been shown to reduce apoptosis and programmed cell death of local tumor cells. Once in the bloodstream, platelets are likely to protect circulating tumor cells from the immune response, favoring the metastatic process. Thus platelets are a fundamental component of the tumor microenvironment as they participate in tumor initiation, progression and response to therapy [4][20].
In the past few years, several clinical studies in breast and prostate cancer patients have highlighted the prognostic value of the detection and characterization of CTCs, suggesting they could even be categorized as follow-up markers and guide personalized treatment decisions. The idea of replacing tumor tissue biopsies to obtain diagnostically and therapeutically relevant information makes CTCs an essential contribution to non-invasive “real-time liquid biopsies” [5][21]. The next step in translating CTCs as liquid biopsy into clinical practice is to demonstrate the utility of these biomarkers. Observational clinical trials have already shown that CTCs and ctDNA are clinically relevant for different types of cancer. However, interventional clinical trials are needed to demonstrate their utility and to include liquid biopsies in clinical guidelines. Many clinical trials already include these determinations as part of specimen testing. However, the extent to which liquid biopsy could eventually replace tissue biopsies remains to be clarified. We know that for diagnosing primary tumors or staging metastatic lesions in tissues that are difficult to sample, liquid biopsy could be a reliable alternative [6][22]. Focusing on breast cancer, the biopsy of metastatic tissue is sometimes not clinically possible due to its location (lung) complicating the correctly determination of the molecular profile of a tumor by the limitation of taking biopsies from different tumor sites [6][22].
2. New Approaches
2.1. Optimize the Standardization of Protocols
Liquid biopsy is a non-invasive methodology, which serves to obtain key tumor information, and it is rapidly transforming the cancer patient’s clinical management. The assessment of the tumor circulating components in the early and advanced setting is very well documented
[7][53]. However, more efficient CTC detection and enrichment technology are needed, including validation of CTCs before they can be incorporated into oncology laboratories. In recent years, the number of clinical trials aimed at assessing the value of CTCs as biomarkers in the treatment of cancer patients has been increasing. That is due to the high demand for minimally invasive diagnostics and an evidence-based medicine approach to treatment selection and monitoring
[8][54]. Despite the numerous platforms developed for CTC analysis, the translation into the clinical practice is still limited
[9][55].
The wide variety of CTC separation technologies and products makes the evaluation and comparison of techniques with each other to establish a standard technique for their study a very tedious task
[10][56]. For future use and approval by health authorities, it is strictly necessary to obtain clinical data to support the standardization of CTC technologies
[10][56]. The importance of reproducibility in CTC detection processes should also not be forgotten, where very few techniques have demonstrated intra- and inter-laboratory reproducibility
[11][37].
In this regard, public-private partnerships have been launched to achieve the standardization of methods and technologies for the analysis of circulating nucleic acids and rare cells. One example is the Innovative Medicines Initiative (IMI) CANCER-ID program (
www.cancer-id.eu) (accessed on 15 September 2021). So far, this consortium has evaluated different technologies for the analysis of blood biomarkers and has developed a set of guidelines for the proper conduct of technology comparison studies. These criteria include best practice recommendations for sample collection, protocols for sample storage and shipping to enable biobanking, as well as comparative data on different methods for molecular analysis of CTCs, ctDNA and miRNAs
[12][32].
In summary, although the most standardized method for CTCs isolation is based on immunomagnetic and fluorescence imaging technology other technologies based on microfluidic technologies are breaking into the liquid biopsy scenario
[13][14][15][16][57,58,59,60] there is a clear need for greater specificity, standardization and transparency in the reports to incorporate the detection of CTCs as another tool in clinical practice focused on individualised therapy
[17][61]. Concerning standardisation, this should be implemented in all steps of the process, sample extraction procedures, isolation of ciculating tumor material, etc., so that the use of the different circulating molecules can be extrapolated to the “real world” in clinics. Similarly, the method should be more ambitious with a multi-omic approaches to demonstrate the great clinical utility of liquid biopsy in cancer patients
[7][53].
2.2. Isolation of CTCs in Other Body Fluids
There are many other body fluids that can provide a source of tumor-derived molecular information, increasing the value of liquid biopsy as a relevant tool in clinical diagnosis to be explored.
The term liquid biopsy is therefore used in contraposition to the traditional surgical tumor biopsy and represents the analysis of cancer biomarkers in tumor-derived material
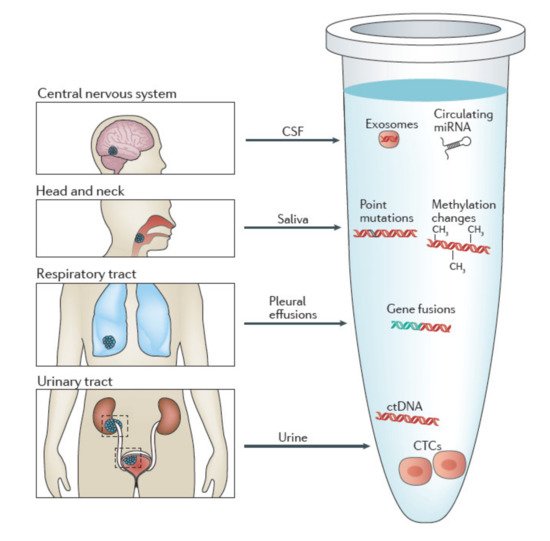
[9][55]. Even though the “standard” concept of liquid biopsy comprises the sampling of blood, almost all body fluids are suitable for liquid biopsy. Common bodily fluids include urine, saliva, sputum, stool, bile, cerebrospinal fluids (CSF) and pleural effusions (
Figure 23)
[18][62].
Figure 23. Body fluids as a source of tumor-derives molecular information. Schematic representation of different body fluids (other than blood) that can contain tumor-derived molecular information. Specifically cerebrospinal fluid (CSF), pleural effusions, saliva, urine. Image created with BioRender.com, and modified from Siravegna et al.
[19][74].
However, there are hardly any studies where isolation of CTCs from other body fluids is performed; most of the investigations are aimed at isolation of ctDNA. Some of the studied body fluids are listed below.
One of the major advantages of using urine is its non-invasive nature of collection compared to tissue or blood, especially in patients requiring repeated sampling to monitor cancer progression and/or therapeutic effects
[20][63].
Currently, there is one clinical trial evaluating urine as a source for liquid biopsy. NCT04432909 is a prospective multicenter, single-blinded study to evaluate the utility of UroCAD for urothelial carcinoma diagnosis and follow-up in 500 participants.
During the past decades, many researchers have performed studies to confirm urine ctDNA as a powerful biomarker not only in urological cancers but also in NSCLC
[21][64], colorectal
[22][65], gastric tumors
[23][66] and breast cancer
[24][67].
Concerning extracellular vesicles (EVs), these cellular elements have become of increasing interest as a potential source of biomarkers due to their role in intercellular communication and the affinity of their molecular content with that of the releasing cells
[25][68].
Several studies have characterized the proteomic profile of urinary EV from urological cancer patients and identified potential biomarkers for bladder cancer and prostate. One of the many studies performed identified urinary EV derived alpha 1-antitrypsin and histone H2B1K as diagnostic and prognostic biomarkers for bladder cancer. When the results were verifying by immunohistochemistry, this confirms significantly higher expression of these markers in bladder cancer tissues than in normal tissues
[26][69].
Depending on the type of cancer different biomarkers can be isolated from saliva, being ctDNA from this source the best biomarker for head and neck squamous cell carcinoma, while miRNAs alone or in association with EVs play a relevant role in the early detection of potentially malignant oral cancers
[18][62].
In 2005, Streckfus, C. et al. showed that C-erb-b2 a breast cancer marker was produced by the salivary glands and detected in the saliva of breast cancer patients
[27][70].
In vitro studies with breast cancer samples have shown that exosomes interact with salivary glands by altering the transcriptome and proteome composition of salivary gland-derived macrovesicles
[28][71].
The results derived from the study by Zhang et al. reveal that transcriptomic and proteomic signatures in saliva can serve as biomarkers for the non-invasive detection of breast cancer. These biomarkers have high specificity and sensitivity, which provide a prediction model validation study for next clinical validation
[29][72].
In the case of cancers restricted to the central nervous system (CNS), there is a shortage of circulating biomarkers (ctDNA). For this reason, CSF, due to its direct contact with the CNS, is a relevant source of biomarkers. Studies to date indicate that CSF-derived ctDNA represents the genetic alterations of brain tumors better than plasma ctDNA
[18][62].
In the case of HER2-positive metastatic breast cancer, the CSF DNA has been reported to provide value and additional information to radiological probes.
It has been described in a study comparing CSF and plasma cDNA molecular profiles, a HER2 positive breast cancer patient with leptomeningeal and extracranial metastases, that the clinical and radiological response of each were different to T-DM1 treatment. The CSF cDNA revealed enrichment of ERBB2 amplification, MYC amplification and mutations of the driver genes PIK3CA and TP53, justifying progression in the CNS, while the decrease reflected a partial clinical response in the extracranial compartment
[30][73].
So, ctDNA has two main diagnostic applications in patients with leptomeningeal metastases: (1) completion of the diagnostic profile in patients with negative titration and (2) identification of actionable genomic alterations with the potential to define optimal targeted therapy
[30][73].
In the case of colorectal cancer (CRC), DNA derived from stool is a powerful diagnostic tool. In lung cancer, sputum protein content and DNA from pleural effusions are highly relevant biomarkers for the diagnosis of lung cancer and malignant pleural mesothelioma
[18][62].
The findings of the case published by Husain et al. in 2017 in a patient with metastatic breast cancer with cytologically active ascites. They highlight the usefulness of cfDNA present in ascitic fluid as a source of additional information that is not detected in free tumor cells and plasma
[21][64].
2.3. Promising Role of CTC Clusters
Circulating tumor cells are disseminated by the primary tumor and metastases into the bloodstream. We know that different subpopulations exist and that they are responsible for the origin of metastases. It is also accepted that CTCs can be found in the blood as single cells or in clusters
[31][16]. There are two theories about the origin of CTC clusters: (1) the clusters may derive directly from the primary tumor in a process where tumor cells cooperate and migrate collectively; and (2) the CTC cluster arises in the bloodstream by aggregation of individual CTCs
[32][19]. A third theory has now been proposed, called “cell-jamming”. According to this theory, higher extracellular matrix (ECM) density may promote cell clustering and thus facilitate the formation of CTC clusters. Thus, it has been observed that mesenchymal tumor cells show a tendency for collective invasion under conditions of high ECM density
[32][19]. The number of CTC clusters are less than single CTCs, but metastasis is 23–50 times more potent than single CTCs
[33][13]. Studies on the molecular profile of CTC clusters have shown a high expression of the desmosomal binding protein plakoglobin, which may be due to its function in maintaining strong cell-cell contacts in tumoral processes and metastasis
[34][24]. Several studies have also shown the importance of keratin 14+ in the mechanism of cluster metastasis. Keratin 14+ may regulate cell-cell adhesion, cell-matrix adhesion and immune evasion. Moreover, transcription factor binding sites for stem and proliferation, including OCT4, NANOG, SOX2 and SIN3A are exactly hypomethylated in CTC clusters
[33][13]. In contrast, transcripts encoding classical CTC markers such as keratins, mucin 1 (MUC1), EpCAM and E-cadherin are under expressed in CTC clusters
[35][75]. Clusters of CTCs are composed not only of tumor cells but also of cancer-associated fibroblasts, white blood cells and platelets
[34][35][24,75]. To ensure the viability of tumor cells in the bloodstream, cooperation is necessary. In fact, neutrophils have been shown to increase the metastatic potential of tumor cells by overexpressing the cell cycle and DNA replication genes
[35][75]. To date, clusters of CTCs have been observed in patients predominantly during advanced disease stages (i.e., with established distant metastases). The last study published by Aceto’s laboratory
[36][76] evidences the presence of CTC clusters in early breast cancer, suggesting their possible involvement in early metastatic spread and disease progression.
Finally, Krol et al. have highlighted two implications of identifying CTC clusters in early breast cancer: (1) CTC clusters are a general event of breast cancer biology regardless of disease stage; and (2) The presence of CTC clusters in early breast cancer could be considered as an additional and substantial risk factor for disease progression. However, further clinical trials are needed to confirm the latter point
[37][77].
CTCs clusters due to their intrinsic heterogeneity provide both spatial and temporal information with a prognostic value, being associated to shorter PFS and OS. Their identification can be solved easily by staining
[37][77] or by separation based on size
[38][78]. Their promising role could be due by their biological activity as a more consistent tool to reproduce primary tumor as compared to tissue biopsy or single CTC providing a possible therapeutic target
[39][79].