Ceramic composites based on alumina and zirconia have found a wide field of application in the present century in orthopedic joint replacements, and their use in dentistry is spreading. The development of this class of bioceramic composites was started in the 1980s, but the first clinical applications of the total hip replacement joint were introduced in the market only in the early 2000s. Since then, several composite systems were introduced in joint replacements. These materials are classified as Zirconia-Toughened Alumina if alumina is the main component or as Alumina-Toughened Zirconia when zirconia is the main component. In addition, some of them may contain a third phase based on strontium exa-aluminate. The flexibility in device design due to the excellent mechanical behavior of this class of bioceramics results in a number of innovative devices for joint replacements in the hip, the knee, and the shoulder, as well in dental implants.
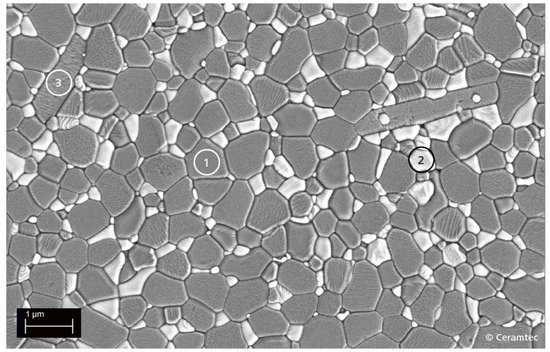
- alumina
- zirconia
- Alumina-Toughened Zirconia
- Zirconia-Toughened Alumina
- hip arthroplasty
- dental implants
1. Introduction
| Property | Units | First-Generation Alumina (1970s) |
Second-Generation (BIOLOX®, Since 1974) |
Third-Generation (BIOLOX®Forte Since 1995) |
|---|---|---|---|---|
| Al2O3 content | vol.% | 99.1–99.6 | 99.7 | >99.8 |
| Density | g cm−3 | 3.90–3.95 | 3.95 | 3.97 |
| Av. grain size | μm | ≤4.5 | 4 | 1.75 |
| Flexural strength | MPa | >300 | 400 | 630 |
| Young’s modulus | GPa | 380 | 410 | 407 |
| Hardness | HV | 1800 | 1900 | 2000 |
| Property | Units | Alumina (1970s) |
Y-TZP |
|---|---|---|---|
| Al2O3 Content | vol % | 99.1–99.6 | -- |
| ZrO2 Content | vol % | -- | >99 |
| Av. Grain Size Al2O3 | µm | ≤4.5 | 0.3 |
| Density | g/cm3 | 3.90–3.95 | 6.02 |
| Thermal Conductivity | W/mK | 30 | 2.5 |
| Hardness | HV | 2000 | 1200 |
| Flexural Strength | MPa | >300 | 1000 |
| Fracture Toughness | MPa m½ | 3.5 | 4.5 |
| Young Modulus | GPa | 380 | 210 |
23. Alumina Zirconia Composites: Early Studies
The abandon of zirconia in 2001 opened a technological gap, leaving unmet the urgent need of ceramic components for arthroplasty with effective design and increased reliability and longevity. Then, materials scientists turned their attention toward different zirconia-toughened ceramics (ZTCs), and promising results were obtained in the development of ceramic composites to be used as biomaterials in orthopedics. The work was focused on composites having alumina (in Zirconia-Toughened Alumina—ZTA) as the main component or zirconia (Alumina-Toughened Zirconia—ATZ). Special attention was devoted to ZTAs. The basic concept of a ZTA material is to substantially increase the material fracture toughness and strength with respect to alumina, while maintaining relevant properties of alumina such as hardness, stiffness, and thermal conductivity, which are key factors for its successful clinical use in joint replacements. This is achieved by exploiting the tetragonal-to-monoclinic phase transformation of zirconia, which is introduced in ZTA as a reinforcing element. The key point for the excellent mechanical properties of ZTA ceramics is the transformability of the tetragonal zirconia. As a consequence, essential aspects are to retain a significant amount of the zirconia tetragonal phase at body temperature and its degree of stabilization in order to reach the desired toughening mechanism. The proper selection of the stabilizing oxide, the homogeneous and finely distribution of Y-TZP in the alumina matrix, and the control of the microstructure and grain size are key parameters to “tune” the stability of the tetragonal phase. In addition, the compressive residual stresses that develop on cooling, due to the mismatch in thermal expansion coefficients between the alumina matrix and the dispersed zirconia phase, increase the energy threshold for the T-M phase transformation, contributing to the strength of the composite [15]. This aspect is critical in the design of a ZTA composite: higher tetragonal zirconia stabilization as a consequence, for example, of a too high yttria concentration would lead to suppression of the zirconia phase transformation, then losing almost all the improvements of ZTA. On the other hand, poor zirconia stabilization—i.e., due to zirconia uncontrolled grain growth because of inappropriate sintering processes—would enhance the LTD of the material. Nevertheless, in the latter case, the mechanical properties might be outstanding, but the material could have unreliable performance, thus leading to catastrophic consequences due to the LTD of the zirconia phase. Furthermore, it is perceived that the toughening mechanisms in monolithic Y-TZP and ZTA are significantly different. In monolithic zirconia, the stress induced by the single transformed ceramic grain makes the neighbor tetragonal zirconia transform as well, consequently spreading the transformation effect throughout the material. Such a transformation results in LTD and deterioration under long-term usage. In the case of alumina–zirconia composites, the zirconia phase is constrained in the stable alumina matrix, thereby preventing the transformation of the adjacent grains. Hence, the ZTA has a better retention of the tetragonal phase compared to the monolithic zirconia, when exposed to hydrothermal conditions in vitro [16]. The first studies on alumina–zirconia composites as biomaterials started during the mid-1980s by French researchers (INSA-Lyon, Ecole Centrale de Lyon) looking for a material strong and tough as zirconia but characterized by better resistance to LTD [17]. Among the tested material, a hot-pressed ZTA (Alumina-20 vol % Y-TZP) showed bending strength (four-point bending) higher than 1100 MPa and fracture toughness of about 10 MPa√m. Aging tests carried out using small bars implanted under the skin of Wistar rats—then in unloaded conditions –showed a limited decrease of the strength due to LTD. Laboratory wear tests (pin-on-disk, cylinder-on-flat) carried out against UHMWPE demonstrated an improved friction and wear behavior of hot-pressed ZTA in comparison with Y-TZP [18]. A further research project was carried out in the framework of the EUREKA programme (project EU 294) under the scientific coordination of the Italian Ceramic Centre (Bologna, Italy). The main goals attained were the production by slip casting of ZTA ball heads with several Z/A ratios [19][20] and the assessment in a hip simulator of the wear behavior of ZTA-UHMWPE bearings. Wear tests were carried out in a hip simulator using Alumina-UHMWPE bearings as the reference. The results did not show significant differences between the experimental and reference material [21]. Cytotoxicity assays confirmed the absence of harmful effects elicited by the composite materials [22].3. Alumina–Zirconia Composites in Orthopedics
Zirconia-Toughened Alumina

References
- Piconi, C.; Maccauro, G.; Muratori, E.; del Brach Prever, E. Alumina and zirconia ceramics in joint replacements: A review. J. Appl. Biomat. Biomech. 2003, 1, 19–32.
- Sandhaus, S. Noveaux Aspects de l’Implantologie. L’Implant CBS; Gessler SA: Sion, Switzerland, 1969.
- Smith, L. Ceramic-Plastic Material as a Bone Substitute. Arch. Surg. 1963, 87, 653–661.
- Boutin, P. Arthroplastie totale de la hanche par prosthéses en alumine fritté. Rev. Chir. Orthop. 1972, 58, 230–246.
- Piconi, C. Alumina. In Comprehensive Biomaterials II; Ducheyne, P., Grainger, D.W., Healy, K.E., Hutmacher, D.W., Kirkpatrick, C.J., Eds.; Elsevier: Oxford, UK, 2017; Volume 1, pp. 92–121.
- Piconi, C.; Labanti, M.; Magnani, G.; Caporale, M.; Maccauro, G.; Magliocchetti, G. Analysis of a failed alumina THR ball head. Biomaterials 1999, 20, 1637–1646.
- Traina, F.; De Fine, M.; Di Martino, A.; Faldini, C. Fracture of Ceramic Bearing Surfaces following Total Hip Replacement: A Systematic Review. BioMed Res. Int. 2013, 2013, 1–8.
- Garvie, R.C.; Nicholson, P.S. Structure and thermodynamical properties of Partially Stabilized Zirconia in the CaO-ZrO2 System. J. Am. Ceram. Soc. 1972, 55, 152–157.
- Garvie, R.C.; Hannink, R.H.J.; Pascoe, R.T. Ceramic Steel? Nature 1975, 258, 703–704.
- Gupta, T.K.; Bechtold, J.H.; Kuznicki, R.C.; Cadoff, L.H.; Rossing, B.R. Stabilization of tetragonal phase in polycrystalline zirconia. J. Mater. Sci. 1977, 12, 2421–2426.
- Piconi, C.; Maccauro, G. Zirconia as a ceramic biomaterial. Biomaterials 1999, 20, 1–25.
- Lughi, V.; Sergo, V. Low temperature degradation -aging- of zirconia: A critical review of the relevant aspects in dentistry. Dent. Mater. 2010, 26, 807–820.
- Piconi, C.; Maccauro, G.; Angeloni, M.; Rossi, B.; Learmonh, I.D. Zirconia heads in perspective: A survey of zirconia outcomes in total hip replacements. Hip. Intl. 2007, 17, 119–130.
- Piconi, C.; Maccauro, G.; Pilloni, L.; Burger, W.; Muratori, F.; Richter, H.G. On the fracture of a zirconia ball head. J. Mater. Sci. Mater. Med. 2006, 17, 289–300.
- Piconi, C.; Porporati, A. Bioinert ceramics: Zirconia and alumina. In Handbook of Bioceramics and Biocomposites; Antoniac, I., Ed.; Springer: Berlin, Germany, 2016; Volume 1, pp. 59–90.
- Fabbri, P.; Piconi, C.; Burresi, E.; Magnani, G.; Mazzanti, F.; Mingazzini, C. Lifetime estimation of a zirconia-alumina composite for biomedical applications. Dent. Mater. 2014, 30, 138–142.
- Mandrino, A.; Moyen, B.; Ben Abdallah, A.; Treheux, D.; Orange, D. Aluminas with dispersoids. Tribol. Prop. In Vivo Aging. Biomater. 1990, 11, 88–91.
- Ben Abdallah, A.; Treheux, D. Frictional and wear of ultrahigh molecular weight polyethylene against various new ceramics. Wear 1991, 142, 43–56.
- Agathopoulos, S.; Nikolopoulos, P.; Salomoni, A.; Tucci, A.; Stamenkovich, I. Preparation and properties of binary oxide bioceramics. J. Mater. Sci. Mater. Med. 1996, 7, 629–636.
- Salomoni, A.; Tucci, A.; Esposito, L.; Stamenkovich, I. Forming and sintering of multiphase bioceramics. J. Mater. Sci. Mater. Med. 1994, 5, 651–653.
- Affatato, S.; Testoni, M.; Cacciari, G.L.; Toni, A. Mixed-oxide prosthetic ceramic ball heads. Part 1: Effect of the ZrO2 fraction on the wear of ceramic on polyethylene joints. Biomaterials 1999, 20, 971–975.
- Ciapetti, G.; Verri, E.; Savioli, F.; Pizzoferrato, A. Vitro Cytotoxicity Testing of Bioceramics for Hip Prosthesis. Proc. 9th SIMCER; Palmonari, C., Stamenkovic, I., Eds.; Centro Ceramico: Bologna, Italy, 2000; pp. 39–42.
- Burger, W.; Richter, H.G. High strength and toughness alumina matrix composites by transformation toughening and “in situ” platelet reinforcement (ZPTA). Key Eng. Mater. 2001, 192–195, 545–548.
- Heimke, G.; Leyen, S.; Willmann, G. Knee arthoplasty: Recently developed ceramics offer new solutions. Biomaterials 2002, 23, 1539–1551.
- Burger, W. Oxidkeramik wieder im Trend-neue Werkstoffe für die Medizintechnik und industrielle Anwendungen. Keram. Z. 2012, 2, 134–137.
- Pecharromán, C.; Bartolome, J.F.; Requena, J.; Moya, J.; Deville, S.; Chevalier, J.; Fantozzi, G.; Torrecillas, R. Percolative Mechanism of Aging in Zirconia-Containing Ceramics for Medical Applications. Adv. Mater. 2003, 15, 507–511.
- Cutler, R.A.; Lindemann, J.M.; Ulvensøen, J.H.; Lange, H.I. Damage-resistant SrO doped Ce-TZP/Al2O3 composites. Mater. Des. 1994, 15, 123–133.
- Piconi, C. Ceramics for joint replacement: Design and application of commercial bearings. In Advances in Ceramic Biomaterials; Palmero, P., Cambier, F., De Barra, E., Eds.; Woodhead: Duxford, UK, 2017; pp. 129–179.
- Ikeda, J.; Mabuchi, M.; Nakanishi, T.; Miyaji, F.; Ueno, M.; Pezzotti, G. Phase Stability and Fracture Toughness of Zirconia Toughened Alumina for Joint Replacement. Damage Assess. Struct. VII 2007, 361, 767–770.
- Ikeda, J.; Murakami, T.; Shimozono, T.; Watanabe, R.; Iwamoto, M.; Nakanishi, T. Characteristics of Low Temperature Degradation Free ZTA for Artificial Joint. Key Eng. Mater. 2014, 631, 18–22.
- Available online: https://global.kyocera.com/prdct/medical/technology/bioceram/material.html (accessed on 30 June 2021).
- Ikeda, J.; Murakami, T.; Sasaki, T.; Shimozono, T.; Shouyama, Y.; Iwamoto, M. Wear amd corrosion resistance of low temperature degradation free ZTA for artificial joints. Key Eng. Mater. 2017, 720, 296–300.
- Al-Hajjar, M.; Jennings, L.M.; Begand, S.; Oberbach, T.; Delfosse, D.; Fisher, J. Wear of novel ceramic-on-ceramic bearings under adverse and clinically relevant hip simulator conditions. J. Biomed. Mater. Res. Part B Appl. Biomater. 2013, 101, 1456–1462.