A prática de exercícios físicos (EF), principalmente o treinamento de força (TF), traz benefícios à saúde da população saudável; entretanto, a literatura é escassa nas recomendações relacionadas à população com deficiência intelectual (DI). Este estudo representa uma primeira análise sobre o tema e tem como objetivo examinar uma estrutura e a eficácia de programas de intervenção experimental de TS em conformidade com DI. Esta revisão sistemática foi realizada entre janeiro e abril de 2021, nas bases de dados PubMed, Web of Science, Scopus e SPORTDiscus, de acordo com as diretrizes do PRISMA.The practice of physical exercise (PE), especially strength training (ST), has health benefits in the healthy population; however, the literature is scarce in the recommendations related to the population with intellectual disability (ID). This study represents the first analysis on the topic and aims to examine the structure and efficacy of ST experimental intervention programs in individuals with ID. This systematic review was carried out between January and April 2021, using the PubMed, Web of Science, Scopus, and SPORTDiscus databases, according to the PRISMA guidelines.
- intellectual disabilities
- neuromuscular training
- physical exercise program
- resistance training
1. Introdução
O TS visa provocar adaptações na musculatura esquelética por meio de sobrecargas, proporcioionando aumento na produção de força muscular e atividade de enzimas glicolíticas, bem como a produção de trifosfato / fosfocreatina de adenosina e adaptações no sistema nervoso, a fim de aumentar o recrutamento de unidades motoras [
ST aims to provoke adaptations in the skeletal musculature through overloads, providing an increase in the production of muscle strength and activity of glycolytic enzymes, as well as the production of adenosine triphosphate/phosphocreatine and adaptations in the nervous system, in order to increase the recruitment of motor units [24,25]. During ST, the lower and upper limbs move against a resistance provided by gravity, body weight, dumbbells, straps, weighted bars, or exercise machines [26–28]. This entire process results in cellular micro-lesions, mainly in the eccentric action phase, activating defense systems such as neutrophils, macrophages, and cytokines, which will generate reactive oxygen and nitrogen species [29]. These micro-sockets are important for the muscle recovery and regeneration process due to the fusion of satellite cells with a main cell, and the induction of protein synthesis metabolism and muscle tissue recovery [30]. Thereafter, ST seems to induce muscle skeletal adaptations as a result of overload, providing an increase in the production of muscular strength and other central nervous system adaptations [24,25].
2. Análise dos resalysis of resultados
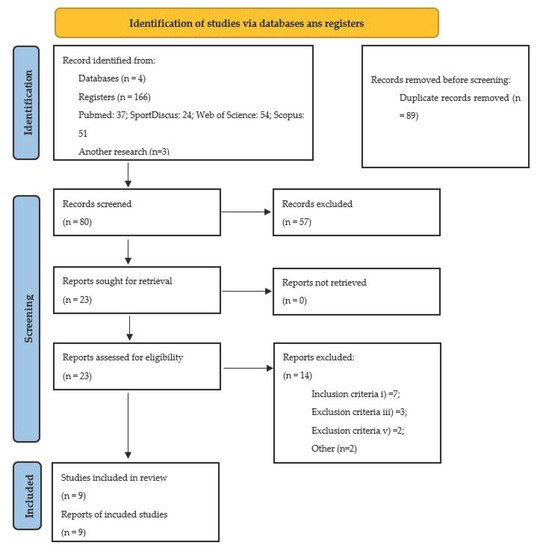
2.1. Seleção de Esctudos
2.2. Characterísticas dos Estudos
2.3. Origthem
2.4. Part articipantes
2,5. Protocolos / instrumo scalentos / técnicas de avaliação
2.6. Características dos protocolospants, study de treinamento de força
3. Percepções atuais
3.1. Duração do programa
3.2. Freqcluência
3.3. Duração da Sessão
3.4. Jogos
3,5
2. Repetições
3,6. Intensidade
2.). A intensidade expressa através da porcentagem da carga de trabalho expressa pelo número de RM variou de 40 a 65% de 8 RM [ 39 , 44 ], de 40 a 50% de 8 RM [ 45 ], e de 60 a 90% de 1 RM [ 47 ]. Diferentes finPalidades, diferentes recursos materiais disponíveis e / ou características individuais podem ser alguns dos motivorticipants para justificar tal gama de intensidades de treinamento usado nos diferentes estudos
2, não atendendo às recomendações usuais sugeridas pelo ACSM [ 48] —75–80% 1 RM. Apesar do uso relatado de intensidades diferentes, em geral, as diretrizes do ACSM [ 48 ] foram aplicadas e todos os estudos relatados um efeito positiEvo (consulte a seção de resultados de ST).
3,7. Exercícios
manual dynamometer [43,45], and different isokinetic strength tests measured by isokinetic dynamometer [45]. It should be noted that Ghaeeni’s [40] and Neto’s [42] studies did not assess neuromuscular capacity, despite applying ST programs. Table 4 shows the duration/frequency, type of exercises, intensity, and results of the nine selected studies.
3,8. Resultados de protrainingramas de ST
showing a weekly frequency of three sessions [39–42,44,45]. The training sessions duration varied between 45 and 60 min. The protocols adopted varied from study to study. Six studies applied circuits in ST machines [39,42,44–47], one study included exercise performed in two surfaces conditions (firm and foam) [41], one study applied exercises with free weights [45], and one study applied an abdominal workout [40]. All studies showed a positive effect from the different ST protocols, which can be seen in Table 4.
3. Os melhores níveDis de força muscular pode permitir que essa população realize um maior cussionúmero de atividades e continuar a se exercitar, assim como o risco de consequências secundárias para sua saúde [ 55 , 56 ]. Além disso, melhorias na resposta à inflamação sistêmica, no sistema de defesa antioxidante e uma redução no dano oxidativo também foram relatadas [
3. Vários estudos diferenças diferenças nos parâmetros de composição corporal após o programa de treinamento de força, a saber: redução do IMC ( p <0,0001) e da dobra cutânea da panturrilha ( p = 0,008) [ 43 ]; diminuição da circunferência da cintura ( p = 0,0416) e aumento da massa magra ( p = 0,011) [ 44 ]; e aumento da massa magra ( p= 0,008) e redução do percentual de gordura ( p = 0,036) [ 43 ] Como o sobrepeso e a obesidade estão associados a problemas de saúde e qualidade de vida, esses resultados mostrados que o treinamento de força é uma boa intervenção para reduzir esses valores2.
3.3. Os diferentes resultados obtidos na Tabela 4 e dos estudos controlados não randomizados [ 57 , 58 , 59 ] são demonstrados devido aos diferentes objetivos e métodos de avaliação utilizados em cada estudo, sendo uma mais-valia a aplicação do TS, uma vez que pode ter este amplo leque de benefícios.Todos essses resultados são importantes para a promoção da qualidade de vida dos relacionados com DI, relacionados ao modelo conceitual de Schalock et al. [ 60 ], um construto don Duratividido em três dimensões: (i) independência; (ii) participação social; (iii) bem-estar
3.
3, instruções simples, supervisão constante e reforço verbal e visual são [ 48 , 53 ] para maior sucesso no processo didático-pedagógico.
that the improvement of task performance is of great interest to this population. Having improved levels of muscle strength may allow this population to perform a greater number of activities and continue to exercise, thus reducing the risk of secondary consequences for their health [55,56]. Additionally, improvements in the response to systemic inflammation, in the antioxidant defense system, and a reduction in oxidative damage were also reported [39,44,45].
process.