Extracorporeal membrane oxygenation (ECMO) is increasingly used for acute respiratory failure with few absolute but many relative contraindications. The contraindications to the initiation of ECMO therapy are not uniformly agreed upon, and each center, as well as each provider involved in the indication for the initiation of ECMO, weights them differently. Whereas absolute contraindications immediately discourage ECMO therapy, relative contraindications should trigger a very thorough consideration of this option. Although relative contraindications should not per se exclude patients from a life-saving procedure such as ECMO, their concurrence may lead to the decision to forgo this procedure. When relative contraindications add up, they might accumulate to a point where they (should) be considered absolute contraindications.
- ARDS
- acute respiratory distress syndrome
- ECMO
- extracorporeal membrane oxygenation
- contraindication
- indication
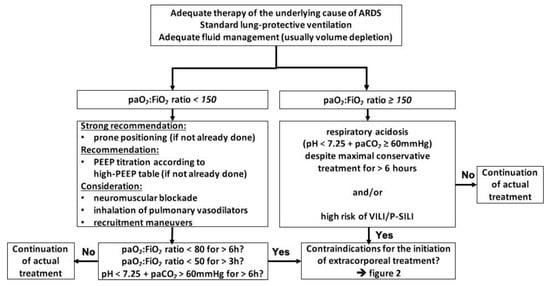
1. Indications for the Initiation of ECMO
2. Absolute Contraindications to the Initiation of ECMO
2.1. Refusal of the Use of Extracorporeal Techniques by the Patient
2.2. Advanced Stage of Cancer
2.3. Fatal Intracerebral Hemorrhage/Cerebral Herniation/Intractable Intracranial Hypertension
| Study | Pathological Condition | Mortality | Worse Outcome | (GOS ≤ 3 or Equal) | |
| Gurer et al. 2017 [24] | Gurer et al. 2017 [11] | SDH/EDH | 49.1% (ICU) | 66.7% (6 months) | |
| Gower et al. 1988 [27] | Gower et al. 1988 [14] | swelling after TBI | 23% (ICU) | 60% (≥ 2 years) | |
| Gaab et al. 1990 [28] | Gaab et al. 1990 [15] | swelling after TBI | 14% (ICU) | 22% (n/a) | |
| Polin et al. 1997 [29] | Polin et al. 1997 [16] | swelling after TBI | 23% (hospital) | 63% (discharge) | |
| De Luca et al. 2000 [30] | De Luca et al. 2000 [17] | swelling after TBI | 18% (n/a) | 59% (n/a) | |
| Taylor et al. 2001 [31] | Taylor et al. 2001 [18] | swelling after TBI (children) | DC: 33% (1 week) medical: 42% (1 week) | 46% (6 months) | |
| Whitfield et al. 2001 [32] | Whitfield et al. 2001 [19] | swelling after TBI | 23% (10 months) | 31% (10 months) | |
| Schneider et al. 2002 [33] | Schneider et al. 2002 [20] | swelling after TBI | 22.5% (6 months) | 71% (6 months) | |
| Albanèse et al. 2003 [34] | Albanèse et al. 2003 [21] | swelling after TBI | early DC: 52% (1 year) late DC: 23% | 62% (1 year) | |
| Aarabi et al. 2006 [35] | Aarabi et al. 2006 [22] | swelling after TBI | 32.4% (30 days) | 48.7% (30 days) | |
| Wettervik et al. 2018 [36] | Wettervik et al. 2018 [23] | swelling after TBI | DC: 17% (6 months) Thiopental: 4% no specific treatment: 11% |
DC: 60% (6 months) Thiopental: 48% no specific treatment: 27% |
|
| Sakai et al. 1998 [37] | Sakai et al. 1998 [24] | cerebral infraction/malignant swelling | 33% (2 months) | 67% (2 months) | |
| Qureshi et al. 2000 [38] | Qureshi et al. 2000 [25] | medical reversal of supratentorial masses | 54% (hospital) | 46% (Barthel & Rankin) (≥6 months) |
|
| Koenig et al. 2008 [39] | Koenig et al. 2008 [26] | medical reversal of transtentorial herniation | 67.6% (hospital) | 77% (GOS 4 & 5) | |
| Skoglund et al. 2005 [40] | Skoglund et al. 2005 [27] | transtentorial herniation after TBI | 26% (≥6 months) | 41% (≥6 months) | |
| Kim et al. 2009 [41] | Kim et al. 2009 [28] | DC for TBI/ICH/infarction | TBI: 21.4% (6 months) ICH: 25% (6 months) Infarction: 60.9% (6 months) |
TBI: 42.9% (6 months) ICH: 50% (6 months) Infarction: 69.6% (6 months) |
|
| Lan et al. 2020 [42] | Lan et al. 2020 [29] | DC for herniation after TBI | 30.4% (6 months) | 66% (6 months) | |
| Delcourt et al. 2017 [43] | Delcourt et al. 2017 [30] | ICH | 12% (90 days) | 45.4% (90 days) | |
| Chen et al. 2019 [44] | Chen et al. 2019 [31] | infratentorial ICH | 8% (90 days) | 28% (90 days) | |
| Poon et al. 2014 [45] (metaanalysis) | Poon et al. 2014 [32] (metaanalysis) | ICH | 46% (1 year) | up to 24% (1 year) | |
| Pinho et al. 2019 [46] (metaanalysis) | Pinho et al. 2019 [33] (metaanalysis) | ICH | 36.3% (1 year) | n/a |
2.4. Irreversible Destruction of the Lung Parenchyma without the Option of Transplantation
2.5. Contraindications to Transplantation without the Option of Sufficient Lung Healing
| Study | Age Defining “Elderly” |
No. of Patients Included Total |
Hospital Mortality in the “Elderly” | ||
|---|---|---|---|---|---|
| History of malignancy (<2–5 years disease free plus high risk of recurrence) | Age >65 years plus low physiological reserve | ||||
| Mendiratta et al. 2014 [58] | Mendiratta et al. 2014 [45] | >65 | 368 | 59% | |
| 54] | Mixed | 66% | n/a | n/a | |
| Huprikar et al. 2019 [67] | Huprikar et al. 2019 [55] | Acute leukemia | n/a | 50% | n/a |
3.3. Time on Injurious Ventilator Settings >7 Days
| Study | Outcomes | |||||
|---|---|---|---|---|---|---|
| Pranikoff et al. 1997 [69] | Pranikoff et al. 1997 [58] | 50% mortality after 5 days on ventilator (90% after 12 days) |
||||
| Significant dysfunction of another major organ system (heart, liver, kidney, brain) | Mechanical ventilation/extracorporeal life support | |||||
| Karagiannidis et al. 2016 [8] | Karagiannidis et al. 2016 [48] | >80 | ||||
| Mols et al. 2000 [ | 1944 | 70 | 76% | ] | Uncorrected coronary artery disease | |
| Deatrick et al. 2020 [61] | Deatrick et al. 2020 [49Controlled coronary artery disease | |||||
| Mols et al. 2000 [59] | No differences between groups | ] | >65 | |||
| Hemmila et al. 2004 [71] | Hemmila et al. 2004 [60] >55 |
182 | 83% | OR 1.20 (1.09, 1.31) (3.2 vs. 4.5 days) (OR 5.53 if > 8 days) 43% |
Unstable medical condition | Significant osteoporosis |
| Giani et al. 2021 [62] | Giani et al. 2021 [50] | >65 | ||||
| Beiderlinden et al. 2006 [72] | Beiderlinden et al. 2006 [61] | OR 1.064 (1.008, 1.123) (5.3 vs. 8.7 days)144 | Uncorrectable bleeding | |||
| Patroniti et al. 2011 [ | Extensive prior chest surgery | |||||
| 56% | 73] | Patroniti et al. 2011 [62] | OR 1.291 |
Poorly controlled infection/resistant microbes | Colonization with resistant microbes | |
| (29% increase each day) | ||||||
| Schmidt et al. 2013 [74] | Schmidt et al. 2013 [63] | p | = 0.0008 between groups (3 vs. 7 days), OR 1.07 | Inadequate social support | Infectious liver cirrhosis | |
| Enger et al. 2014 [75] | Enger et al. 2014 [64] | Severe thorax deformity | HIV infection (unless treated adequately) | |||
| BMI ≥35 kg/m | 2 | BMI 30–35 kg/m | 2 | |||
| Nonadherence to medical therapy (recent & history) | Significant malnutrition | |||||
| Inability to comply with therapy | Specific infections [55] | Specific infections [42] | ||||
| Active tuberculosis/contraindications to immunosuppression | Poorly controlled diabetes, hypertension, epilepsy, peptic ulcer disease, gastroesophageal reflux, or central venous obstruction | |||||
| History of illicit substance abuse | ||||||
| Inability to participate in rehabilitation |
3. Relative Contraindications to the Initiation of ECMO
3.1. Advanced Age >70 Years
5.2. Immunocompromized Patients/Pharmacological Immunosuppression
| Study | Disease State | ICU Mortality | Hospital Mortality | Odds Ratio | |
|---|---|---|---|---|---|
| Cawcutt et al. 2014 [65] | Cawcutt et al. 2014 [53] | HIV/AIDS | 40% | 60% | n/a |
| Schmidt et al. 2018 [66] | Schmidt et al. 2018 [ | ||||
| ] | |||||
| p | |||||
| = 0.140 between groups (1.08 vs. 1.67 days) | |||||
| Kon et al. 2017 [ | |||||
| 87 | |||||
| ] | |||||
| Kon et al. 2017 | |||||
| [ | |||||
| 76 | |||||
| ] | |||||
| OR 0.998 (0.997–0.999), | |||||
| p | |||||
| = 0.001 | |||||
| Wu et al. 2017 [88] | Wu et al. 2017 [77] | p | < 0.001 between groups (1 vs. 6 days) | ||
| Schmidt et al. 2018 [66] | Schmidt et al. 2018 [54] | p | = 0.004 between groups (2 vs. 3 days) | ||
| Posluszny et al. 2020 [89] | Posluszny et al. 2020 [78] | p | = 0.028 between groups (2.33 vs. 3.25 days) | ||
| Giraud et al. 2021 [90] | Giraud et al. 2021 [79] | p | = 0.01 between groups (3.79 vs. 8.67 days) | ||
| Supady et al. 2021 [91] | Supady et al. 2021 [80] | p | = 0.006 between groups (3 vs. 6 days) |
3.4. Right-Heart Failure
3.5. Hematologic Malignancies, Especially Bone Marrow Transplantation and Graft-Versus-Host Disease
| Study | ICU Mortality | Hospital Mortality | Bone Marrow Transplant/HSCT Mortality (Hospital) | |||||
|---|---|---|---|---|---|---|---|---|
| Gow et al. 2010 [117] | Gow et al. 2010 [106] | 61% | 68% | 50% | ||||
| Wohlfarth et al. 2014 [76] | Wohlfarth et al. 2014 [65] | 50% | 50% | 100% | ||||
| Kang et al. 2015 [118] | Kang et al. 2015 [107] | 100% | 100% | 100% | ||||
| Choi et al. 2016 [80] | Choi et al. 2016 [69] | n/a | 80.9% | |||||
| p | ||||||||
| = 0.013 between groups (2 vs. 5 days) | ||||||||
| n/a | ||||||||
| Wohlfarth et al. 2017 [119] | Wohlfarth et al. 2017 [108] | n/a | 81% | 100% (GvHD) | ||||
| Stecher et al. 2018 [124] | Stecher et al. 2018 [113] | n/a | 80% | 100% | ||||
| Cho et al. 2019 [121] | Cho et al. 2019 [110] | 66% | 88% | 66.7% | Mendiratta et al. 2014 [58] | Mendiratta et al. 2014 [45] | p | = 0.049 between groups (1.19 vs. 1.73 days) |
| Park et al. 2021 [122] | Park et al. 2021 [111] | n/a | 86% (OR 42.25 (9.53, 187.22)) | 85.7% (OR 64) | Wohlfarth et al. 2014 [76] | Wohlfarth et al. 2014 [65] | p | = 0.17 between groups (1 vs. 3 days) |
| Schmidt et al. 2015 [77] | Schmidt et al. 2015 [66] | OR 1.15 (1.06, 1.26) (2 vs. 4 days) | ||||||
| Klinzing et al. 2015 [78] | Klinzing et al. 2015 [67] | p | = 0.14 between groups (1 vs. 4 days) | |||||
| Cheng et al. 2016 [79] | Cheng et al. 2016 [68] | p | < 0.001 between groups (1 vs. 6 days), OR 4.71 (1.98, 11.23) | |||||
| Choi et al. 2016 [80] | Choi et al. 2016 [69] | p | = 0.11 between groups (4.5 vs. 4.77 days) | |||||
| Huang et al. 2016 [81] | Huang et al. 2016 [70] | p | = 0.093 between groups (0.5 vs. 1.8 days) | |||||
| Hsin et al. 2016 [82] | Hsin et al. 2016 [71] | p | < 0.001 between groups (1 vs. 6 days) | |||||
| Lee et al. 2016 [83] | Lee et al. 2016 [72] | p | = 0.114 between groups (2.3 vs. 4.2 days) | |||||
| Serpa Neto et al. 2016 [84] | Serpa Neto et al. 2016 [73] | p | = 0.061 between groups (2 vs. 3 days) | |||||
| Wu et al. 2016 [85] | Wu et al. 2016 [74] | p | = 0.005 between groups (2.75 vs. 6.92 days) | |||||
| Hilder et al. 2017 [86] | Hilder et al. 2017 [75 |
3.6. SAPS II Score ≥ 60 Points
3.7. SOFA Score >12 Points (mSOFA Score >8 Points)
3.8. PRESERVE Score ≥ 5 Points
3.9. RESP Score Worse Than −2 Points
3.10. PRESET Score ≥ 6 Points
References
- Patel, B.; Chatterjee, S.; Davignon, S.; Herlihy, J.P. Extracorporeal membrane oxygenation as rescue therapy for severe hypoxemic respiratory failure. J. Thorac. Dis. 2019, 11, S1688–S1697.
- Brower, R.G.; Lanken, P.N.; MacIntyre, N.; Matthay, M.A.; Morris, A.; Ancukiewicz, M.; Schoenfeld, D.; Thompson, B.T.; National Heart, L.; Blood Institute, A.C.T.N. Higher versus lower positive end-expiratory pressures in patients with the acute respiratory distress syndrome. N. Engl. J. Med. 2004, 351, 327–336.
- Moerer, O.; Tonetti, T.; Quintel, M. Rescue therapies for acute respiratory distress syndrome: What to try first? Curr. Opin. Crit. Care 2017, 23, 52–59.
- Harnisch, L.O.; Moerer, O. ECMO therapy for ARDS: When, how, and how is the outcome? In DIVI Jahrbuch 2020/2021; Kluge, S., Heringlake, M., Janssens, U., Rieckels, E., Eds.; Medizinisch Wissenschaftliche Verlagsgesellschaft: Berlin, Germany, 2020; pp. 367–372.
- Fichtner, F.; Moerer, O.; Laudi, S.; Weber-Carstens, S.; Nothacker, M.; Kaisers, U.; the Guideline Group on Mechanical Ventilation; Extracorporeal Membrane Oxygenation in Acute Respiratory Insufficiency. Mechanical Ventilation and Extracorporeal Membrane Oxygena tion in Acute Respiratory Insufficiency. Dtsch. Arztebl. Int. 2018, 115, 840–847.
- Combes, A.; Hajage, D.; Capellier, G.; Demoule, A.; Lavoue, S.; Guervilly, C.; Da Silva, D.; Zafrani, L.; Tirot, P.; Veber, B.; et al. Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2018, 378, 1965–1975.
- Patroniti, N.; Bonatti, G.; Senussi, T.; Robba, C. Mechanical ventilation and respiratory monitoring during extracorporeal membrane oxygenation for respiratory support. Ann. Transl. Med. 2018, 6, 386.
- Neitzke, G.; Burchardi, H.; Duttge, G.; Hartog, C.; Erchinger, R.; Gretenkort, P.; Michalsen, A.; Mohr, M.; Nauck, F.; Salomon, F.; et al. Limits to the appropriateness of intensive care. Med. Klin. Intensivmed. Notfmed. 2019, 114, 46–52.
- Felli, A.; Skhirtladze-Dworschak, K.; Opfermann, P.; Dworschak, M. Limitations of Cerebral Oximetry in a Patient With an Intracerebral Hemorrhage and Brain Edema on Extracorporeal Membrane Oxygenation: A Case Report. AA Pract. 2019, 12, 390–392.
- Nokes, B.T.; Vaszar, L.; Jahanyar, J.; Swanson, K.L. VV-ECMO-Assisted High-Risk Endobronchial Stenting as Rescue for Asphyxiating Mediastinal Mass. J. Bronchol. Interv. Pulmonol. 2018, 25, 144–147.
- Gurer, B.; Kertmen, H.; Yilmaz, E.R.; Dolgun, H.; Hasturk, A.E.; Sekerci, Z. The Surgical Outcome of Traumatic Extraaxial Hematomas Causing Brain Herniation. Turk. Neurosurg. 2017, 27, 37–52.
- Chakalov, I.; Harnisch, L.O.; Meyer, A.C.; Moerer, O. Preemptive veno-venous ECMO support in a patient with anticipated difficult airway: A case report. Respir. Med. Case Rep. 2020, 30, 101130.
- Kalita, J.; Misra, U.K.; Vajpeyee, A.; Phadke, R.V.; Handique, A.; Salwani, V. Brain herniations in patients with intracerebral hemorrhage. Acta Neurol. Scand. 2009, 119, 254–260.
- Gower, D.J.; Lee, K.S.; McWhorter, J.M. Role of subtemporal decompression in severe closed head injury. Neurosurgery 1988, 23, 417–422.
- Gaab, M.R.; Rittierodt, M.; Lorenz, M.; Heissler, H.E. Traumatic brain swelling and operative decompression: A prospective investigation. Acta Neurochir. Suppl. 1990, 51, 326–328.
- Polin, R.S.; Shaffrey, M.E.; Bogaev, C.A.; Tisdale, N.; Germanson, T.; Bocchicchio, B.; Jane, J.A. Decompressive bifrontal craniectomy in the treatment of severe refractory posttraumatic cerebral edema. Neurosurgery 1997, 41, 84–92.
- De Luca, G.P.; Volpin, L.; Fornezza, U.; Cervellini, P.; Zanusso, M.; Casentini, L.; Curri, D.; Piacentino, M.; Bozzato, G.; Colombo, F. The role of decompressive craniectomy in the treatment of uncontrollable post-traumatic intracranial hypertension. Acta Neurochir. Suppl. 2000, 76, 401–404.
- Taylor, A.; Butt, W.; Rosenfeld, J.; Shann, F.; Ditchfield, M.; Lewis, E.; Klug, G.; Wallace, D.; Henning, R.; Tibballs, J. A randomized trial of very early decompressive craniectomy in children with traumatic brain injury and sustained intracranial hypertension. Child’s Nerv. Syst. ChNS Off. J. Int. Soc. Pediatric Neurosurg. 2001, 17, 154–162.
- Whitfield, P.C.; Patel, H.; Hutchinson, P.J.; Czosnyka, M.; Parry, D.; Menon, D.; Pickard, J.D.; Kirkpatrick, P.J. Bifrontal decompressive craniectomy in the management of posttraumatic intracranial hypertension. Br. J. Neurosurg. 2001, 15, 500–507.
- Schneider, G.H.; Bardt, T.; Lanksch, W.R.; Unterberg, A. Decompressive craniectomy following traumatic brain injury: ICP, CPP and neurological outcome. Acta Neurochir. Suppl. 2002, 81, 77–79.
- Albanese, J.; Leone, M.; Alliez, J.R.; Kaya, J.M.; Antonini, F.; Alliez, B.; Martin, C. Decompressive craniectomy for severe traumatic brain injury: Evaluation of the effects at one year. Crit. Care Med. 2003, 31, 2535–2538.
- Aarabi, B.; Hesdorffer, D.C.; Ahn, E.S.; Aresco, C.; Scalea, T.M.; Eisenberg, H.M. Outcome following decompressive craniectomy for malignant swelling due to severe head injury. J. Neurosurg. 2006, 104, 469–479.
- Wettervik, T.S.; Lenell, S.; Nyholm, L.; Howells, T.; Lewen, A.; Enblad, P. Decompressive craniectomy in traumatic brain injury: Usage and clinical outcome in a single centre. Acta Neurochir. 2018, 160, 229–237.
- Sakai, K.; Iwahashi, K.; Terada, K.; Gohda, Y.; Sakurai, M.; Matsumoto, Y. Outcome after external decompression for massive cerebral infarction. Neurol. Med. Chir. 1998, 38, 131–135.
- Qureshi, A.I.; Geocadin, R.G.; Suarez, J.I.; Ulatowski, J.A. Long-term outcome after medical reversal of transtentorial herniation in patients with supratentorial mass lesions. Crit. Care Med. 2000, 28, 1556–1564.
- Koenig, M.A.; Bryan, M.; Lewin, J.L., 3rd; Mirski, M.A.; Geocadin, R.G.; Stevens, R.D. Reversal of transtentorial herniation with hypertonic saline. Neurology 2008, 70, 1023–1029.
- Skoglund, T.; Nellgard, B. Long-time outcome after transient transtentorial herniation in patients with traumatic brain injury. Acta Anaesthesiol. Scand. 2005, 49, 337–340.
- Kim, K.T.; Park, J.K.; Kang, S.G.; Cho, K.S.; Yoo, D.S.; Jang, D.K.; Huh, P.W.; Kim, D.S. Comparison of the effect of decompressive craniectomy on different neurosurgical diseases. Acta Neurochir 2009, 151, 21–30.
- Lan, Z.; Richard, S.A.; Li, Q.; Wu, C.; Zhang, Q.; Chen, R.; Yang, C. Outcomes of patients undergoing craniotomy and decompressive craniectomy for severe traumatic brain injury with brain herniation: A retrospective study. Medicine 2020, 99, e22742.
- Delcourt, C.; Zheng, D.; Chen, X.; Hackett, M.; Arima, H.; Hata, J.; Heeley, E.; Al-Shahi Salman, R.; Woodward, M.; Huang, Y.; et al. Associations with health-related quality of life after intracerebral haemorrhage: Pooled analysis of INTERACT studies. J. Neurol. Neurosurg. Psychiatry 2017, 88, 70–75.
- Chen, R.; Wang, X.; Anderson, C.S.; Robinson, T.; Lavados, P.M.; Lindley, R.I.; Chalmers, J.; Delcourt, C. Infratentorial Intracerebral Hemorrhage. Stroke 2019, 50, 1257–1259.
- Poon, M.T.; Fonville, A.F.; Al-Shahi Salman, R. Long-term prognosis after intracerebral haemorrhage: Systematic review and meta-analysis. J. Neurol. Neurosurg. Psychiatry 2014, 85, 660–667.
- Pinho, J.; Costa, A.S.; Araujo, J.M.; Amorim, J.M.; Ferreira, C. Intracerebral hemorrhage outcome: A comprehensive update. J. Neurol. Sci. 2019, 398, 54–66.
- Giangreco, A.; Arwert, E.N.; Rosewell, I.R.; Snyder, J.; Watt, F.M.; Stripp, B.R. Stem cells are dispensable for lung homeostasis but restore airways after injury. Proc. Natl. Acad. Sci. USA 2009, 106, 9286–9291.
- Oliveira, M.V.; Abreu, S.C.; Padilha, G.A.; Rocha, N.N.; Maia, L.A.; Takiya, C.M.; Xisto, D.G.; Suki, B.; Silva, P.L.; Rocco, P.R. Characterization of a Mouse Model of Emphysema Induced by Multiple Instillations of Low-Dose Elastase. Front. Physiol 2016, 7, 457.
- Meltzer, E.B.; Noble, P.W. Idiopathic pulmonary fibrosis. Orphanet J. Rare Dis. 2008, 3, 8.
- Harnisch, L.O.; Moerer, O. Sequential use of extracorporeal devices to avoid mechanical ventilation in a patient with complicated pulmonary fibrosis. J. Artif. Organs Off. J. Jpn. Soc. Artif. Organs 2017, 20, 365–370.
- Umei, N.; Ichiba, S.; Sakamoto, A. Idiopathic pulmonary fibrosis patient supported with extracorporeal membrane oxygenation for 403 days while waiting for a lung transplant: A case report. Respir. Med. Case Rep. 2018, 24, 86–88.
- Wakwaya, Y.; Brown, K.K. Idiopathic Pulmonary Fibrosis: Epidemiology, Diagnosis andOutcomes. Am. J. Med. Sci. 2019, 357, 359–369.
- Khush, K.K.; Cherikh, W.S.; Chambers, D.C.; Harhay, M.O.; Hayes, D., Jr.; Hsich, E.; Meiser, B.; Potena, L.; Robinson, A.; Rossano, J.W.; et al. The International Thoracic Organ Transplant Registry of the International Society for Heart and Lung Transplantation: Thirty-sixth adult heart transplantation report-2019; focus theme: Donor and recipient size match. J. Heart Lung Transplant. Off. Publ. Int. Soc. Heart Transplant. 2019, 38, 1056–1066.
- Bos, S.; Vos, R.; Van Raemdonck, D.E.; Verleden, G.M. Survival in adult lung transplantation: Where are we in 2020? Curr. Opin. Organ. Transpl. 2020, 25, 268–273.
- Weill, D. Lung transplantation: Indications and contraindications. J. Thorac. Dis. 2018, 10, 4574–4587.
- de Rooij, S.E.; Govers, A.; Korevaar, J.C.; Abu-Hanna, A.; Levi, M.; de Jonge, E. Short-term and long-term mortality in very elderly patients admitted to an intensive care unit. Intensive Care Med. 2006, 32, 1039–1044.
- Sim, Y.S.; Jung, H.; Shin, T.R.; Kim, D.G.; Park, S.M. Mortality and outcomes in very elderly patients 90 years of age or older admitted to the ICU. Respir. Care 2015, 60, 347–355.
- Mendiratta, P.; Tang, X.; Collins, R.T., 2nd; Rycus, P.; Brogan, T.V.; Prodhan, P. Extracorporeal membrane oxygenation for respiratory failure in the elderly: A review of the Extracorporeal Life Support Organization registry. ASAIO J. Am. Soc. Artif. Intern. Organs 1992. 2014, 60, 385–390.
- Volpi, S.; Sertic, F.; Valchanov, K.; De Silva, R. Use veno-venous extra corporeal membrane oxygenation in elderly patients with post-cardiotomy hypoxia: The changing paradigm of respiratory support in adult respiratory distress syndrome. J. Cardiothorac. Surg. 2019, 14, 10.
- Hayanga, J.A.; Murphy, E.; Girgis, R.E.; Jansma, S.; Khaghani, A. Extracorporeal Membrane Oxygenation as a Bridge to Lung Transplantation in Patients Over Age 70 Years: A Case Report. Transpl. Proc. 2017, 49, 218–220.
- Karagiannidis, C.; Brodie, D.; Strassmann, S.; Stoelben, E.; Philipp, A.; Bein, T.; Muller, T.; Windisch, W. Extracorporeal membrane oxygenation: Evolving epidemiology and mortality. Intensive Care Med. 2016, 42, 889–896.
- Deatrick, K.B.; Mazzeffi, M.A.; Galvagno, S.M., Jr.; Tesoriero, R.B.; Kaczoroswki, D.J.; Herr, D.L.; Dolly, K.; Rabinowitz, R.P.; Scalea, T.M.; Menaker, J. Outcomes of Venovenous Extracorporeal Membrane Oxygenation When Stratified by Age: How Old Is Too Old? ASAIO J. Am. Soc. Artif. Intern. Organs 1992. 2020, 66, 946–951.
- Giani, M.; Forlini, C.; Fumagalli, B.; Rona, R.; Pesenti, A.; Foti, G. Indication for Venovenous Extracorporeal Membrane Oxygenation: Is 65 Years Old, Too Old? ASAIO J. Am. Soc. Artif. Intern. Organs 1992. 2021, 67, e55.
- Azoulay, E.; Russell, L.; Van de Louw, A.; Metaxa, V.; Bauer, P.; Povoa, P.; Montero, J.G.; Loeches, I.M.; Mehta, S.; Puxty, K.; et al. Diagnosis of severe respiratory infections in immunocompromised patients. Intensive Care Med. 2020, 46, 298–314.
- Azoulay, E.; Mokart, D.; Pene, F.; Lambert, J.; Kouatchet, A.; Mayaux, J.; Vincent, F.; Nyunga, M.; Bruneel, F.; Laisne, L.M.; et al. Outcomes of critically ill patients with hematologic malignancies: Prospective multicenter data from France and Belgium--a groupe de recherche respiratoire en reanimation onco-hematologique study. J. Clin. Oncol 2013, 31, 2810–2818.
- Cawcutt, K.; Gallo De Moraes, A.; Lee, S.J.; Park, J.G.; Schears, G.J.; Nemergut, M.E. The use of ECMO in HIV/AIDS with Pneumocystis jirovecii Pneumonia: A case report and review of the literature. ASAIO J. Am. Soc. Artif. Intern. Organs 1992. 2014, 60, 606–608.
- Schmidt, M.; Schellongowski, P.; Patroniti, N.; Taccone, F.S.; Reis Miranda, D.; Reuter, J.; Prodanovic, H.; Pierrot, M.; Dorget, A.; Park, S.; et al. Six-Month Outcome of Immunocompromised Patients with Severe Acute Respiratory Distress Syndrome Rescued by Extracorporeal Membrane Oxygenation. An International Multicenter Retrospective Study. Am. J. Respir. Crit. Care Med. 2018, 197, 1297–1307.
- Huprikar, N.A.; Peterson, M.R.; DellaVolpe, J.D.; Sams, V.G.; Lantry, J.H.; Walter, R.J.; Osswald, M.B.; Chung, K.K.; Mason, P.E. Salvage extracorporeal membrane oxygenation in induction-associated acute respiratory distress syndrome in acute leukemia patients: A case series. Int. J. Artif. Organs 2019, 42, 49–54.
- Fichtner, F.; Moerer, O.; Weber-Carstens, S.; Nothacker, M.; Kaisers, U.; Laudi, S.; Guideline, G. Clinical Guideline for Treating Acute Respiratory Insufficiency with Invasive Ventilation and Extracorporeal Membrane Oxygenation: Evidence-Based Recommendations for Choosing Modes and Setting Parameters of Mechanical Ventilation. Respiration 2019, 98, 357–372.
- Extracorporeal Life Support Organization. ELSO Guidelines for Adult Respiratory Failure. 2017. Available online: https://www.elso.org/Portals/0/ELSO%20Guidelines%20For%20Adult%20Respiratory%20Failure%201_4.pdf (accessed on 1 July 2021).
- Pranikoff, T.; Hirschl, R.B.; Steimle, C.N.; Anderson, H.L., 3rd; Bartlett, R.H. Mortality is directly related to the duration of mechanical ventilation before the initiation of extracorporeal life support for severe respiratory failure. Crit. Care Med. 1997, 25, 28–32.
- Mols, G.; Loop, T.; Geiger, K.; Farthmann, E.; Benzing, A. Extracorporeal membrane oxygenation: A ten-year experience. Am. J. Surg. 2000, 180, 144–154.
- Hemmila, M.R.; Rowe, S.A.; Boules, T.N.; Miskulin, J.; McGillicuddy, J.W.; Schuerer, D.J.; Haft, J.W.; Swaniker, F.; Arbabi, S.; Hirschl, R.B.; et al. Extracorporeal life support for severe acute respiratory distress syndrome in adults. Ann. Surg. 2004, 240, 595–605.
- Beiderlinden, M.; Eikermann, M.; Boes, T.; Breitfeld, C.; Peters, J. Treatment of severe acute respiratory distress syndrome: Role of extracorporeal gas exchange. Intensive Care Med. 2006, 32, 1627–1631.
- Patroniti, N.; Zangrillo, A.; Pappalardo, F.; Peris, A.; Cianchi, G.; Braschi, A.; Iotti, G.A.; Arcadipane, A.; Panarello, G.; Ranieri, V.M.; et al. The Italian ECMO network experience during the 2009 influenza A(H1N1) pandemic: Preparation for severe respiratory emergency outbreaks. Intensive Care Med. 2011, 37, 1447–1457.
- Schmidt, M.; Tachon, G.; Devilliers, C.; Muller, G.; Hekimian, G.; Brechot, N.; Merceron, S.; Luyt, C.E.; Trouillet, J.L.; Chastre, J.; et al. Blood oxygenation and decarboxylation determinants during venovenous ECMO for respiratory failure in adults. Intensive Care Med. 2013, 39, 838–846.
- Enger, T.; Philipp, A.; Videm, V.; Lubnow, M.; Wahba, A.; Fischer, M.; Schmid, C.; Bein, T.; Muller, T. Prediction of mortality in adult patients with severe acute lung failure receiving veno-venous extracorporeal membrane oxygenation: A prospective observational study. Crit. Care 2014, 18, R67.
- Wohlfarth, P.; Ullrich, R.; Staudinger, T.; Bojic, A.; Robak, O.; Hermann, A.; Lubsczyk, B.; Worel, N.; Fuhrmann, V.; Schoder, M.; et al. Extracorporeal membrane oxygenation in adult patients with hematologic malignancies and severe acute respiratory failure. Crit. Care 2014, 18, R20.
- Schmidt, M.; Stewart, C.; Bailey, M.; Nieszkowska, A.; Kelly, J.; Murphy, L.; Pilcher, D.; Cooper, D.J.; Scheinkestel, C.; Pellegrino, V.; et al. Mechanical ventilation management during extracorporeal membrane oxygenation for acute respiratory distress syndrome: A retrospective international multicenter study. Crit. Care Med. 2015, 43, 654–664.
- Klinzing, S.; Wenger, U.; Steiger, P.; Starck, C.T.; Wilhelm, M.; Schuepbach, R.A.; Maggiorini, M. External validation of scores proposed for estimation of survival probability of patients with severe adult respiratory distress syndrome undergoing extracorporeal membrane oxygenation therapy: A retrospective study. Crit. Care 2015, 19, 142.
- Cheng, Y.T.; Wu, M.Y.; Chang, Y.S.; Huang, C.C.; Lin, P.J. Developing a simple preinterventional score to predict hospital mortality in adult venovenous extracorporeal membrane oxygenation: A pilot study. Medicine 2016, 95, e4380.
- Choi, K.B.; Kim, H.W.; Jo, K.H.; Kim do, Y.; Choi, H.J.; Hong, S.B. Extracorporeal Life Support in Patients with Hematologic Malignancies: A Single Center Experience. Korean J. Thorac. Cardiovasc. Surg. 2016, 49, 280–286.
- Huang, L.; Li, T.; Xu, L.; Hu, X.M.; Duan, D.W.; Li, Z.B.; Gao, X.J.; Li, J.; Wu, P.; Liu, Y.W.; et al. Performance of Multiple Risk Assessment Tools to Predict Mortality for Adult Respiratory Distress Syndrome with Extracorporeal Membrane Oxygenation Therapy: An External Validation Study Based on Chinese Single-center Data. Chin. Med. J. 2016, 129, 1688–1695.
- Hsin, C.H.; Wu, M.Y.; Huang, C.C.; Kao, K.C.; Lin, P.J. Venovenous extracorporeal membrane oxygenation in adult respiratory failure: Scores for mortality prediction. Medicine 2016, 95, e3989.
- Lee, S.; Yeo, H.J.; Yoon, S.H.; Lee, S.E.; Cho, W.H.; Jeon, D.S.; Kim, Y.S.; Son, B.S.; Kim do, H. Validity of Outcome Prediction Scoring Systems in Korean Patients with Severe Adult Respiratory Distress Syndrome Receiving Extracorporeal Membrane Oxygenation Therapy. J. Korean Med. Sci. 2016, 31, 932–938.
- Serpa Neto, A.; Schmidt, M.; Azevedo, L.C.; Bein, T.; Brochard, L.; Beutel, G.; Combes, A.; Costa, E.L.; Hodgson, C.; Lindskov, C.; et al. Associations between ventilator settings during extracorporeal membrane oxygenation for refractory hypoxemia and outcome in patients with acute respiratory distress syndrome: A pooled individual patient data analysis: Mechanical ventilation during ECMO. Intensive Care Med. 2016, 42, 1672–1684.
- Wu, M.Y.; Huang, C.C.; Wu, T.I.; Wang, C.L.; Lin, P.J. Venovenous Extracorporeal Membrane Oxygenation for Acute Respiratory Distress Syndrome in Adults: Prognostic Factors for Outcomes. Medicine 2016, 95, e2870.
- Hilder, M.; Herbstreit, F.; Adamzik, M.; Beiderlinden, M.; Burschen, M.; Peters, J.; Frey, U.H. Comparison of mortality prediction models in acute respiratory distress syndrome undergoing extracorporeal membrane oxygenation and development of a novel prediction score: The PREdiction of Survival on ECMO Therapy-Score (PRESET-Score). Crit. Care 2017, 21, 301.
- Kon, Z.N.; Bittle, G.J.; Pasrija, C.; Pham, S.M.; Mazzeffi, M.A.; Herr, D.L.; Sanchez, P.G.; Griffith, B.P. Venovenous Versus Venoarterial Extracorporeal Membrane Oxygenation for Adult Patients With Acute Respiratory Distress Syndrome Requiring Precannulation Hemodynamic Support: A Review of the ELSO Registry. Ann. Thorac. Surg. 2017, 104, 645–649.
- Wu, M.Y.; Chang, Y.S.; Huang, C.C.; Wu, T.I.; Lin, P.J. The impacts of baseline ventilator parameters on hospital mortality in acute respiratory distress syndrome treated with venovenous extracorporeal membrane oxygenation: A retrospective cohort study. BMC Pulm. Med. 2017, 17, 181.
- Posluszny, J.; Engoren, M.; Napolitano, L.M.; Rycus, P.T.; Bartlett, R.H.; centers, E.m. Predicting Survival of Adult Respiratory Failure Patients Receiving Prolonged (>/=14 Days) Extracorporeal Membrane Oxygenation. ASAIO J. Am. Soc. Artif. Intern. Organs 1992. 2020, 66, 825–833.
- Giraud, R.; Legouis, D.; Assouline, B.; De Charriere, A.; Decosterd, D.; Brunner, M.E.; Moret-Bochatay, M.; Fumeaux, T.; Bendjelid, K. Timing of VV-ECMO therapy implementation influences prognosis of COVID-19 patients. Physiol. Rep. 2021, 9, e14715.
- Supady, A.; DellaVolpe, J.; Taccone, F.S.; Scharpf, D.; Ulmer, M.; Lepper, P.M.; Halbe, M.; Ziegeler, S.; Vogt, A.; Ramanan, R.; et al. Outcome Prediction in Patients with Severe COVID-19 Requiring Extracorporeal Membrane Oxygenation-A Retrospective International Multicenter Study. Membranes 2021, 11, 170.
- Mekontso Dessap, A.; Boissier, F.; Charron, C.; Begot, E.; Repesse, X.; Legras, A.; Brun-Buisson, C.; Vignon, P.; Vieillard-Baron, A. Acute cor pulmonale during protective ventilation for acute respiratory distress syndrome: Prevalence, predictors, and clinical impact. Intensive Care Med. 2016, 42, 862–870.
- Vogel, D.J.; Fabbri, A.; Falvo, A.; Powell-Tuck, J.; Desai, N.; Vasques, F.; Meadows, C.; Ioannou, N.; Glover, G.; Brame, A.; et al. Assessment of Right Ventricular Function With CT and Echocardiography in Patients With Severe Acute Respiratory Distress Syndrome on Extracorporeal Membrane Oxygenation. Crit. Care Explor. 2021, 3, e0345.
- Lazzeri, C.; Cianchi, G.; Bonizzoli, M.; Batacchi, S.; Terenzi, P.; Bernardo, P.; Valente, S.; Gensini, G.F.; Peris, A. Right ventricle dilation as a prognostic factor in refractory acute respiratory distress syndrome requiring veno-venous extracorporeal membrane oxygenation. Minerva Anestesiol. 2016, 82, 1043–1049.
- Price, L.C.; McAuley, D.F.; Marino, P.S.; Finney, S.J.; Griffiths, M.J.; Wort, S.J. Pathophysiology of pulmonary hypertension in acute lung injury. Am. J. Physiol Lung Cell Mol. Physiol. 2012, 302, L803–L815.
- Nilsson, M.C.; Freden, F.; Larsson, A.; Wiklund, P.; Bergquist, M.; Hambraeus-Jonzon, K. Hypercapnic acidosis transiently weakens hypoxic pulmonary vasoconstriction without affecting endogenous pulmonary nitric oxide production. Intensive Care Med. 2012, 38, 509–517.
- Mekontso Dessap, A.; Charron, C.; Devaquet, J.; Aboab, J.; Jardin, F.; Brochard, L.; Vieillard-Baron, A. Impact of acute hypercapnia and augmented positive end-expiratory pressure on right ventricle function in severe acute respiratory distress syndrome. Intensive Care Med. 2009, 35, 1850–1858.
- Balanos, G.M.; Talbot, N.P.; Dorrington, K.L.; Robbins, P.A. Human pulmonary vascular response to 4h of hypercapnia and hypocapnia measured using Doppler echocardiography. J. Appl. Physiol. 2002, 94, 1543–1551.
- Vieillard-Baron, A.; Schmitt, J.M.; Augarde, R.; Fellahi, J.L.; Prin, S.; Page, B.; Beauchet, A.; Jardin, F. Acute cor pulmonale in acute respiratory distress syndrome submitted to protective ventilation: Incidence, clinical implications, and prognosis. Crit. Care Med. 2001, 29, 1551–1555.
- Vieillard-Baron, A.; Loubieres, Y.; Schmitt, J.M.; Page, B.; Dubourg, O.; Jardin, F. Cyclic changes in right ventricular output impedance during mechanical ventilation. J. Appl. Physiol. 1999, 87, 1644–1650.
- Lansdorp, B.; Hofhuizen, C.; van Lavieren, M.; van Swieten, H.; Lemson, J.; van Putten, M.J.; van der Hoeven, J.G.; Pickkers, P. Mechanical ventilation-induced intrathoracic pressure distribution and heart-lung interactions*. Crit. Care Med. 2014, 42, 1983–1990.
- Shah, T.G.; Wadia, S.K.; Kovach, J.; Fogg, L.; Tandon, R. Echocardiographic parameters of right ventricular function predict mortality in acute respiratory distress syndrome: A pilot study. Pulm. Circ. 2016, 6, 155–160.
- Boissier, F.; Katsahian, S.; Razazi, K.; Thille, A.W.; Roche-Campo, F.; Leon, R.; Vivier, E.; Brochard, L.; Vieillard-Baron, A.; Brun-Buisson, C.; et al. Prevalence and prognosis of cor pulmonale during protective ventilation for acute respiratory distress syndrome. Intensive Care Med. 2013, 39, 1725–1733.
- Osman, D.; Monnet, X.; Castelain, V.; Anguel, N.; Warszawski, J.; Teboul, J.L.; Richard, C.; the French Pulmonary Artery Catheter Study Group. Incidence and prognostic value of right ventricular failure in acute respiratory distress syndrome. Intensive Care Med. 2009, 35, 69–76.
- Giraud, R.; Banfi, C.; Siegenthaler, N.; Bendjelid, K. Massive pulmonary embolism leading to cardiac arrest: One pathology, two different ECMO modes to assist patients. J. Clin. Monit. Comput. 2016, 30, 933–937.
- Reis Miranda, D.; van Thiel, R.; Brodie, D.; Bakker, J. Right ventricular unloading after initiation of venovenous extracorporeal membrane oxygenation. Am. J. Respir. Crit. Care Med. 2015, 191, 346–348.
- Roumy, A.; Liaudet, L.; Rusca, M.; Marcucci, C.; Kirsch, M. Pulmonary complications associated with veno-arterial extra-corporeal membrane oxygenation: A comprehensive review. Crit. Care 2020, 24, 212.
- Zangrillo, A.; Landoni, G.; Biondi-Zoccai, G.; Greco, M.; Greco, T.; Frati, G.; Patroniti, N.; Antonelli, M.; Pesenti, A.; Pappalardo, F. A meta-analysis of complications and mortality of extracorporeal membrane oxygenation. Crit. Care Resusc. 2013, 15, 172–178.
- Bunge, J.J.H.; Caliskan, K.; Gommers, D.; Reis Miranda, D. Right ventricular dysfunction during acute respiratory distress syndrome and veno-venous extracorporeal membrane oxygenation. J. Thorac. Dis. 2018, 10, S674–S682.
- Lecuyer, L.; Chevret, S.; Guidet, B.; Aegerter, P.; Martel, P.; Schlemmer, B.; Azoulay, E. Case volume and mortality in haematological patients with acute respiratory failure. Eur. Respir. J. 2008, 32, 748–754.
- Benoit, D.D.; Vandewoude, K.H.; Decruyenaere, J.M.; Hoste, E.A.; Colardyn, F.A. Outcome and early prognostic indicators in patients with a hematologic malignancy admitted to the intensive care unit for a life-threatening complication. Crit. Care Med. 2003, 31, 104–112.
- Azoulay, E.; Thiery, G.; Chevret, S.; Moreau, D.; Darmon, M.; Bergeron, A.; Yang, K.; Meignin, V.; Ciroldi, M.; Le Gall, J.R.; et al. The prognosis of acute respiratory failure in critically ill cancer patients. Medicine 2004, 83, 360–370.
- Azoulay, E.; Lemiale, V.; Mokart, D.; Pene, F.; Kouatchet, A.; Perez, P.; Vincent, F.; Mayaux, J.; Benoit, D.; Bruneel, F.; et al. Acute respiratory distress syndrome in patients with malignancies. Intensive Care Med. 2014, 40, 1106–1114.
- Azoulay, E.; Mokart, D.; Kouatchet, A.; Demoule, A.; Lemiale, V. Acute respiratory failure in immunocompromised adults. Lancet Respir Med. 2019, 7, 173–186.
- Lemiale, V.; Resche-Rigon, M.; Mokart, D.; Pene, F.; Rabbat, A.; Kouatchet, A.; Vincent, F.; Bruneel, F.; Nyunga, M.; Lebert, C.; et al. Acute respiratory failure in patients with hematological malignancies: Outcomes according to initial ventilation strategy. A groupe de recherche respiratoire en reanimation onco-hematologique (Grrr-OH) study. Ann. Intensive Care 2015, 5, 28.
- Molina, R.; Bernal, T.; Borges, M.; Zaragoza, R.; Bonastre, J.; Granada, R.M.; Rodriguez-Borregan, J.C.; Nunez, K.; Seijas, I.; Ayestaran, I.; et al. Ventilatory support in critically ill hematology patients with respiratory failure. Crit. Care 2012, 16, R133.
- Gow, K.W.; Lao, O.B.; Leong, T.; Fortenberry, J.D. Extracorporeal life support for adults with malignancy and respiratory or cardiac failure: The Extracorporeal Life Support experience. Am. J. Surg. 2010, 199, 669–675.
- Kang, H.S.; Rhee, C.K.; Lee, H.Y.; Kim, Y.K.; Kwon, S.S.; Kim, S.C.; Lee, J.W. Clinical outcomes of extracorporeal membrane oxygenation support in patients with hematologic malignancies. Korean J. Intern. Med. 2015, 30, 478–488.
- Wohlfarth, P.; Beutel, G.; Lebiedz, P.; Stemmler, H.J.; Staudinger, T.; Schmidt, M.; Kochanek, M.; Liebregts, T.; Taccone, F.S.; Azoulay, E.; et al. Characteristics and Outcome of Patients After Allogeneic Hematopoietic Stem Cell Transplantation Treated With Extracorporeal Membrane Oxygenation for Acute Respiratory Distress Syndrome. Crit. Care Med. 2017, 45, e500–e507.
- Gupta, M.; Shanley, T.P.; Moler, F.W. Extracorporeal life support for severe respiratory failure in children with immune compromised conditions. Pediatric Crit. Care Med. A J. Soc. Crit. Care Med. World Fed. Pediatric Intensive Crit. Care Soc. 2008, 9, 380–385.
- Cho, S.; Cho, W.C.; Lim, J.Y.; Kang, P.J. Extracorporeal Life Support in Adult Patients with Hematologic Malignancies and Acute Circulatory and/or Respiratory Failure. Korean J. Thorac. Cardiovasc. Surg. 2019, 52, 25–31.
- Park, C.; Ko, U.W.; Ko, R.E.; Na, S.J.; Yang, J.H.; Jeon, K.; Suh, G.Y.; Sung, K.; Cho, Y.H. Outcomes of extracorporeal membrane oxygenation in adults with active hematologic and nonhematologic malignancy. Artif. Organs 2021.
- Seggewiss, R.; Einsele, H. Immune reconstitution after allogeneic transplantation and expanding options for immunomodulation: An update. Blood 2010, 115, 3861–3868.
- Stecher, S.S.; Beyer, G.; Goni, E.; Tischer, J.; Herold, T.; Schulz, C.; Op den Winkel, M.; Stemmler, H.J.; Lippl, S. Extracorporeal Membrane Oxygenation in Predominantly Leuco- and Thrombocytopenic Haematologic/Oncologic Patients with Acute Respiratory Distress Syndrome-a Single-Centre Experience. Oncol. Res. Treat. 2018, 41, 539–543.
- Le Gall, J.R.; Lemeshow, S.; Saulnier, F. A New Simplified Acute Physiology Score (SAPSII) Based on a European/ North American Multicenter Study. JAMA J. Am. Med. Assoc. 1993, 270.
- Choi, M.J.; Ha, S.O.; Kim, H.S.; Park, S.; Han, S.J.; Lee, S.H. The Simplified Acute Physiology Score II as a Predictor of Mortality in Patients Who Underwent Extracorporeal Membrane Oxygenation for Septic Shock. Ann. Thorac. Surg. 2017, 103, 1246–1253.
- Kim, K.I.; Lee, H.S.; Kim, H.S.; Ha, S.O.; Lee, W.Y.; Park, S.J.; Lee, S.H.; Lee, T.H.; Seo, J.Y.; Choi, H.H.; et al. The pre-ECMO simplified acute physiology score II as a predictor for mortality in patients with initiation ECMO support at the emergency department for acute circulatory and/or respiratory failure: A retrospective study. Scand. J. Trauma Resusc. Emerg. Med. 2015, 23, 59.
- Fisser, C.; Rincon-Gutierrez, L.A.; Enger, T.B.; Taccone, F.S.; Broman, L.M.; Belliato, M.; Nobile, L.; Pappalardo, F.; Malfertheiner, M.V. Validation of Prognostic Scores in Extracorporeal Life Support: A Multi-Centric Retrospective Study. Membranes 2021, 11, 84.
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonca, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996, 22, 707–710.
- Ferreira, F.L.; Bota, D.P.; Bross, A.; Melot, C.; Vincent, J.L. Serial evaluation of the SOFA score to predict outcome in critically ill patients. JAMA J. Am. Med. Assoc. 2001, 286, 1754–1758.
- de Grooth, H.J.; Geenen, I.L.; Girbes, A.R.; Vincent, J.L.; Parienti, J.J.; Oudemans-van Straaten, H.M. SOFA and mortality endpoints in randomized controlled trials: A systematic review and meta-regression analysis. Crit. Care 2017, 21, 38.
- Raith, E.P.; Udy, A.A.; Bailey, M.; McGloughlin, S.; MacIsaac, C.; Bellomo, R.; Pilcher, D.V.; the Australian and New Zealand Intensive Care Society Centre for Outcomes and Resource Evaluation (CORE). Prognostic Accuracy of the SOFA Score, SIRS Criteria, and qSOFA Score for In-Hospital Mortality Among Adults With Suspected Infection Admitted to the Intensive Care Unit. JAMA J. Am. Med. Assoc. 2017, 317, 290–300.
- Minne, L.; Abu-Hanna, A.; de Jonge, E. Evaluation of SOFA-based models for predicting mortality in the ICU: A systematic review. Crit. Care 2008, 12, R161.
- Safari, S.; Shojaee, M.; Rahmati, F.; Barartloo, A.; Hahshemi, B.; Forouzanfar, M.M.; Mohammadi, E. Accuracy of SOFA score in prediction of 30-day outcome of critically ill patients. Turk. J. Emerg. Med. 2016, 16, 146–150.
- Sarkar, R.; Martin, C.; Mattie, H.; Gichoya, J.W.; Stone, D.J.; Celi, L.A. Performance of intensive care unit severity scoring systems across different ethnicities in the USA: A retrospective observational study. Lancet Digit. Health 2021, 3, e241–e249.
- Grissom, C.K.; Brown, S.M.; Kuttler, K.G.; Boltax, J.P.; Jones, J.; Jephson, A.R.; Orme, J.F., Jr. A modified sequential organ failure assessment score for critical care triage. Disaster Med. Public Health Prep. 2010, 4, 277–284.
- Schmidt, M.; Zogheib, E.; Roze, H.; Repesse, X.; Lebreton, G.; Luyt, C.E.; Trouillet, J.L.; Brechot, N.; Nieszkowska, A.; Dupont, H.; et al. The PRESERVE mortality risk score and analysis of long-term outcomes after extracorporeal membrane oxygenation for severe acute respiratory distress syndrome. Intensive Care Med. 2013, 39, 1704–1713.
- Kang, H.R.; Kim, D.J.; Lee, J.; Cho, Y.J.; Kim, J.S.; Lee, S.M.; Lee, J.H.; Jheon, S.; Lee, C.T.; Lee, Y.J. A Comparative Analysis of Survival Prediction Using PRESERVE and RESP Scores. Ann. Thorac. Surg. 2017, 104, 797–803.
- Schmidt, M.; Bailey, M.; Sheldrake, J.; Hodgson, C.; Aubron, C.; Rycus, P.T.; Scheinkestel, C.; Cooper, D.J.; Brodie, D.; Pellegrino, V.; et al. Predicting survival after extracorporeal membrane oxygenation for severe acute respiratory failure. The Respiratory Extracorporeal Membrane Oxygenation Survival Prediction (RESP) score. Am. J. Respir. Crit. Care Med. 2014, 189, 1374–1382.
- Tabatabai, A.; Ghneim, M.H.; Kaczorowski, D.J.; Shah, A.; Dave, S.; Haase, D.J.; Vesselinov, R.; Deatrick, K.B.; Rabin, J.; Rabinowitz, R.P.; et al. Mortality Risk Assessment in COVID-19 Veno-Venous Extracorporeal Membrane Oxygenation. Ann. Thorac. Surg. 2021.
- Montero, S.; Slutsky, A.S.; Schmidt, M. The PRESET-Score: The extrapulmonary predictive survival model for extracorporeal membrane oxygenation in severe acute respiratory distress syndrome. J. Thorac. Dis. 2018, 10, S2040–S2044.