The practice of physical exercise (PE), especially strength training (ST), has health benefits in the healthy population; however, the literature is scarce in the recommendations related to the population with intellectual disability (ID). This study represents the first analysis on the topic and aims to examine the structure and efficacy of ST experimental intervention programs in individuals with ID. This systematic review was carried out between January and April 2021, using the PubMed, Web of Science, Scopus, and SPORTDiscus databases, according to the PRISMA guidelines.A prática de exercícios físicos (EF), principalmente o treinamento de força (TF), traz benefícios à saúde da população saudável; entretanto, a literatura é escassa nas recomendações relacionadas à população com deficiência intelectual (DI). Este estudo representa a primeira análise sobre o tema e tem como objetivo examinar a estrutura e a eficácia de programas de intervenção experimental de TS em indivíduos com DI. Esta revisão sistemática foi realizada entre janeiro e abril de 2021, nas bases de dados PubMed, Web of Science, Scopus e SPORTDiscus, de acordo com as diretrizes do PRISMA.
1. Introdução
O TS visa provocar adaptioações na musculatura esquelética por meio de sobrecargas, proporcionando aumento na produção de força muscular e atividade de enzimas glicolíticas, bem como a produção de trifosfato / fosfocreatina de adenosina e adaptações no sistema nervoso, a fim de aumentar o recrutamento de unidades motoras [ 24 , 25 ]. Durante o ST, os membros inferiores e superiores se movem contra uma resistência fornecida pela gravidade, peso corporal, halteres, tiras, barras de peso ou máquinas de exercício [ 26 , 27 , 28] Todo esse processo resulta em microlesões celulares, principalmente na fase de ação excêntrica, ativando sistemas de defesa como neutrófilos, macrófagos e citocinas, que gerarão espécies reativas de oxigênio e nitrogênio [ 29 ]. Esses micro-soquetes são importantes para o processo de recuperação e regeneração muscular devido à fusão das células satélites com uma célula principal, além da indução do metabolismo da síntese de proteínas e recuperação do tecido muscular [ 30 ]. A partir daí, o TF parece induzir adaptações músculo-esqueléticas em decorrência da sobrecarga, proporcionando aumento na produção de força muscular e outras adaptações do sistema nervoso central [ 24 , 25 ].
ST aims to provoke adaptations in the skeletal musculature through overloads, providing an increase in the production of muscle strength and activity of glycolytic enzymes, as well as the production of adenosine triphosphate/phosphocreatine and adaptations in the nervous system, in order to increase the recruitment of motor units [1][2]. During ST, the lower and upper limbs move against a resistance provided by gravity, body weight, dumbbells, straps, weighted bars, or exercise machines [3][4][5]. This entire process results in cellular micro-lesions, mainly in the eccentric action phase, activating defense systems such as neutrophils, macrophages, and cytokines, which will generate reactive oxygen and nitrogen species [6]. These micro-sockets are important for the muscle recovery and regeneration process due to the fusion of satellite cells with a main cell, and the induction of protein synthesis metabolism and muscle tissue recovery [30]. Thereafter, ST seems to induce muscle skeletal adaptations as a result of overload, providing an increase in the production of muscular strength and other central nervous system adaptations [1][2].
2. Análise dos resultados
2. Analysis on Results
2.1. Selection of Studies
2.1. Seleção de Estudos
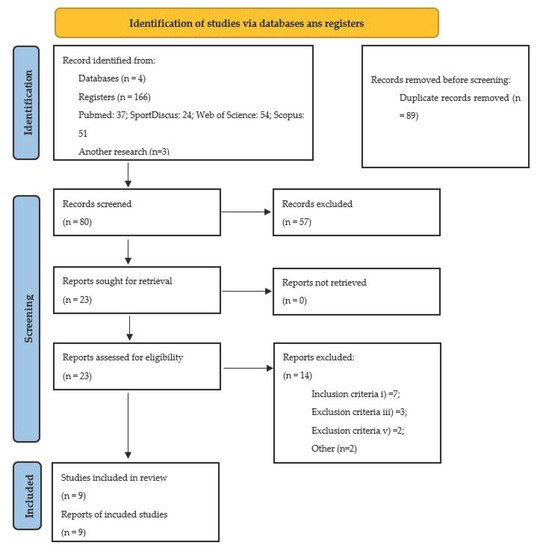
The initial research carried out in the four databases identified 169 studies. In the first phase, and after reading the titles and the abstracts, 23 potentially relevant studies were identified for the next phase. Considering the inclusion and exclusion criteria, previously defined for this systematic review, of the complete reading of the studies, a sample of nine was constituted for their full analysis.A pesquisa inicial realizada nas quatro bases de dados identificou 169 estudos. Na primeira fase, e após a leitura dos títulos e resumos, foram identificados 23 estudos potencialmente relevantes para a fase seguinte. Critérios de inclusão e exclusão, definidos para esta revisão sistemática, da leitura na íntegra dos estudos, constituiu-se uma amostra de nove para sua análise na íntegra.
Figure 1 represents the PRISMA flowchart of this systematic review.A Figura 1 representa o fluxograma PRISMA desta revisão sistemática.
Figure 1. Flow diagram PRISMA.Figura 1. Diagrama de fluxo PRISMA.
2.2. Characteristics of Studies
2.2. Características dos Estudos
Table 1 shows the nine studies included for systematic review, as well as the results of the quality of information assessment. The quality analysis of the studies showed that scores varied between six and eight on the PEDro scale, thus presenting a good quality of the methodological procedures.A Tabela 2 mostra os nove estudos incluídos para revisão sistemática, bem como os resultados da avaliação da qualidade da informação. A análise da qualidade dos estudos mostrou que os escores variaram de seis a oito na escala PEDro, apresentando uma boa qualidade dos procedimentos metodológicos.
Table 1. Assessment of the quality of the articles, using the PEDro scale, as well as their total score.
| Author (Year) |
PEDro Scale |
Total |
A Tabela 3 mostra os objetivos, os participantes, os desenhos dos estudos e a avaliação dos instrumentos / técnicas utilizadas nos estudos incluídos.
Table 2. Characteristics of the strength training programs of the nine studies.
| Author, Year, Country |
Aims |
Participants |
Study Design |
Assessment Tools/Techniques |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
10 |
11 |
|
| Fornieles et al. [7] |
s |
1 |
0 |
1 |
- |
- |
0 |
1 |
1 |
1 |
1 |
6 |
Fornieles et al. [7]
Spain |
Influence of ST on salivary immunoglobulin A levels and hormone profile in sedentary DS adults. |
N = 40 ♂; age: 23.7 ± 3.1;
DS (IQ: 60–69);
randomized groups:
GE: N = 24 | CG: N = 16). |
Prospective cohort. |
8 RM test (exercises: bicep curl; leg extension; seated row; leg curl; triceps extension; leg press);
saliva samples—analysis of immunoglobulin, testosterone, and cortisol (ELISA kits);
box stacking test (ACSM, 2013; Smail and Horvat, 2006). |
Ghaeeni et al. [8] |
s |
1 |
0 |
Ghaeeni et al. [8]
Iran | 1 |
- |
- |
Effect of 8 weeks core stability training on static balance of DS children. |
N = 16; | 0 |
age: 9.7 ± 1.7 y; DS;
| 1 |
randomized groups:
GE: N = 8 | CG: N = 8. | 1 |
1 |
1 |
6 |
[13]
Spain |
Effect of ST on antioxidant defence system in sedentary DS. |
N = 36 ♂;
age: 28.1 ± 3.3;
DS (mild ID–IQ: 60–69);
randomized groups:
GE: N = 18 | CG: N = 18. |
Prospective cohort. |
8 RM test (exercises: arm curl, leg extension, leg curl, low stroke, triceps extension and leg press);
blood samples—puncture of the antecubital vein;
maximum force—manual dynamometer JAMAR (Bolingbrook, IL, USA);
peak torque of flexion and extension of the of the knees—isokinetic dynamometer at 90°/s -Technogym-REV 9000 (Technogym Spa, Gambettola, Italy);
total antioxidant status of plasma—spectrophotometrically, Hitachi 902 Autoanalyzer (Roche, Alameda, CA, USA) by commercial kits (Randox, Crumlin, UK);
reduced glutathione level after reaction with DTNB [(5,5-dithio-bis (2-nitrobenzoic acid)];
superoxide dismutase activity—xanthine oxidase-cytochrome c method;
glutathione reductase activity;
plasma ascorbate and α-tocopherol—reverse phase high-performance liquid chromatography. |
Shields and Taylor [14]
Australia |
Effects of ST on the ability to produce muscle strength and physical fitness. |
N = 23 (♂ = 17; ♀ = 6); age: 15.6 ± 1.6; DS (mild to moderate ID);
random groups:
GE: N = 11 | CG: N = 12. |
Prospective cohort. |
1 RM test (chest and leg press);
timed Up and Go test (Rikli and Jones, 1999);
down stairs test (Zaino et al., 2004);
grocery shelving task (Hill et al., 2004). |
Shields et al. [15]
Australia |
Effects of ST in adolescents and young DS adults. |
N = 68 (♂ = 38; ♀ = 30); age: 17.9 ± 2.6; DS (mild to moderate ID);
random groups:
GE: N = 34 | CG: N = 34. |
Prospective cohort. |
Box stacking test (ACSM, 2013);
weighted pail carry test (ACSM, 2013);
1 RM test (chest and leg press). |
Tabela 3. Características dos programas de treinamento de força dos nove estudos.
2.3. Origem
2.3. Origin
Dos nove estudos selecionados que foram analisados na revisão sistemática, um é da Ásia [ 40 ], outro da África [ 41 ], dois são da Oceania [ 46 , 47 ], dois outros são da América [ 42 , 43 ] e três são da Europa, sendo a Espanha o país com maior número de publicações sobre o tema [ 39 , 44 , 45 ].
From the nine selected studies that were analyzed in the systematic review, one is from Asia [8], another from Africa [9], two are from Oceania [14][15], two others are from America [10][11] and three are from Europe, with Spain being the country with the largest number of publications about this topic [7][12][13].
2.4. Participants
2.4. Participantes
The total number of participants involved in the selected studies are 280, 150 included in the intervention groups and 130 as part of the control groups. The subjects’ mean age from all the studies is 18.23 ± 2.86 years, including children, adolescents, and young adults. All the studies used participants with ID and associated Down syndrome, except for the study of Kachouri et al. [9]. There is a shortage of studies in the literature that implemented ST programs in participants with ID without any other associated condition and using a randomized controlled method.O número total de participantes envolvidos nos estudos selecionados é de 280, 150 incluídos nos grupos de intervenção e 130 como parte dos grupos de controle. A idade média dos sujeitos de todos os estudos é de 18,23 ± 2,86 anos, incluindo crianças, adolescentes e adultos jovens. Todos os estudos utilizaram participantes com DI e síndrome de Down associada, exceto o estudo de Kachouri et al. [ 41 ]. Na literatura existe uma escassez de estudos que implementaram programas de TS em participantes com DI sem nenhuma outra condição associada e utilizando um método controlado randomizado.
2.5. Evaluation Protocols/Instruments/Techniques
2,5. Protocolos / instrumentos / técnicas de avaliação
Most studies used assessment instruments, such as the agility test, the “box stacking” test, the “supermarket” test, the “bucket transportation” test, or the stairs up/down test [7][12][14][15] to evaluate functional capacity. The anthropometric assessment was accomplished using weight, height, waist circumference, and Body Mass Index—BMI [10][11]. Some studies also evaluate fat-free mass and fat mass using the electrical bioimpedance method or subcutaneous adiposity skinfolds [10][11][12]. Although there was a wide dispersion in the evaluation methods used in different studies, the neuromuscular capacity is always assessed either through the exercises prescribed in the training programs or through standard assessments. Maximal and submaximal strength tests were used, such as the one max repetition test—1 RM [14][15], the 8 RM [7][13], the handgrip test measured by manual dynamometer [11][13], and different isokinetic strength tests measured by isokinetic dynamometer [13]. It should be noted that Ghaeeni’s [8] and Neto’s [10] studies did not assess neuromuscular capacity, despite applying ST programs. Table 3 shows the duration/frequency, type of exercises, intensity, and results of the nine selected studies.A maioria dos estudos utilizou instrumentos de avaliação, como o teste de agilidade, o teste de “empilhamento de caixas”, o teste de “supermercado”, o teste de “transporte de baldes” ou o teste de subir / descer escadas [ 39 , 44 , 46 , 47 ] para avaliar capacidade funcional. A avaliação antropométrica foi realizada usando peso, altura, circunferência da cintura e Índice de Massa Corporal - IMC [ 42 , 43 ]. Alguns estudos também avaliam a massa livre de gordura e a massa gorda usando o método de bioimpedância elétrica ou dobras cutâneas de adiposidade subcutânea [ 42 , 43 , 44] Embora tenha havido uma grande dispersão nos métodos de avaliação utilizados nos diferentes estudos, a capacidade neuromuscular é sempre avaliada, seja por meio dos exercícios prescritos nos programas de treinamento, seja por meio de avaliações padronizadas. Testes de força máxima e submáxima foram usados, como o teste de uma repetição máxima — 1 RM [ 46 , 47 ], a 8 RM [ 39 , 45 ], o teste de preensão manual medido por dinamômetro manual [ 43 , 45 ] e diferentes forças isocinéticas testes medidos por dinamômetro isocinético [ 45 ]. Deve-se notar que Ghaeeni's [ 40 ] e Neto's [ 42] estudos não avaliaram a capacidade neuromuscular, apesar de aplicar programas de ST. A Tabela 4 mostra a duração / frequência, tipo de exercícios, intensidade e resultados dos nove estudos selecionados.
Table 3. Characteristics of the strength training protocols from the nine studies.
| Author, Year |
Program Duration, Frequency,
Session Duration |
Exercise Protocol |
Results |
| Fornieles et al. [7] |
12 weeks;
3 × week;
session duration ND. |
Exercises: arm curl; leg extension; seated row; leg curl; triceps extension; leg press;
intensity: 40 a 65% 8 RM;
2 sets; 6 to 10 rep; 90 sec rest. |
Increased concentration of salivary immunoglobulin (p = 0.0120), testosterone levels (p = 0.0088) and job performance (p = 0.0141). |
| Ghaeeni et al. [8] |
8 weeks;
3 × week;
45 a 60 min/session. |
Abdominal workout;
Prospective cohort. |
3 to 4 exercises per session;
3 to 6 sets; 10 to 20 rep.Static balance—stork test (Rahmani and Shahrokhi, 2011). |
Improvement of static balance (p = 0.0001). |
Kachouri. et al. [9] |
s |
1 |
0 |
1 |
- |
- |
Kachouri et al. [9]
Tunisia |
8 weeks; | 0 |
1 |
1 |
1 |
1 |
| Kachouri et al. | 6 |
[9]
Tunisia |
Effect of a combined strength and proprioception training program on muscle strength and postural balance in children with ID. |
3 × week;
45 a 60 min/session.N = 20 ♂;
age: 11.5 ± 1;
ID (IQ: 50–70);
randomized groups:
GE: N = 10 | CG: N = 10. |
All exercises were performed in two surfaces, firm and foam; Prospective cohort. |
exercises included air squat, squat jumps, straight sit ups, power sit up, flutter kicks, two-foot ankle hop, single-foot side-to side ankle hop, tuck jump with knees up, standing long jump, double leg hops, single leg hops, standing on one-foot, lateral jump with both feet, lateral jump with one foot, running up the stairs with one foot and running up the stairs with both feet.
3 to 5 sets; 15 to 20 rep.Maximum voluntary contraction—quadríceps (dynamometer or manual muscle testing—Bohannon, 2005; Brinkmann, Andres, Medoza, and Sanjak, 1997); |
Improves postural balance.
centre of pressure—static stabilometric platform (PostureWin©, Techno Concept®, Cereste, France; 12-bits A/D conversion). |
Neto et al. [10] |
s |
1 |
0 |
1 |
- |
- |
0 |
1 |
1 |
1 |
1 |
| Neto et al. | 6 |
[10]
Brazil |
Effects of ST on body composition. |
| Neto et al. | N = 15 (♂ = 11; ♀ = 4); age: 22.1 ± 7.5; DS;
randomized groups:
GE: ♂ = 6; ♀ = 2
CG: ♂ = 5; ♀ = 2. |
Prospective cohort. |
[10Body mass—electronic scale model Filizola (Indústria Filizola S/A, São Paulo, Brazil);
percentage of fat—seven thoracic, axillary, tricipital, subscapular, abdominal, supra-iliac, and thigh skinfolds (adipometer);
fat mass calculated using the formula: body mass × percentage of fat/100;
lean mass calculated using the formula: body mass − fat mass. |
] |
12 weeks;
3 × week;
60 min/session. |
Exercises: chest press, squat, shoulders, leg curl, one-sided stroke, heel lift, bicipital curl, tricipital French e abdominal crunch;
3 sets; 8 to 12 rep; 30 to 60 sec rest. |
Increased lean mass (p = 0.008) and reduced fat percentage (p = 0.036). |
Ortiz-Ortiz et al. [11] |
s |
Ortiz-Ortiz et al. [11]
Mexico | 1 |
0 |
1 |
- |
Effect of a physical fitness program on body composition and isometric strength | - |
Ortiz-Ortiz et al. [
| 0 |
1 |
11]in DS children. | 1 |
1 |
16 weeks;
5 × week;
55 min/session.N = 22;
age: 11.8 ± 1.9 y; DS;
randomized groups:
GE: N = 13 | CG: N = 9. |
Prospective cohort. |
Body weight—Tanita |
Circuit exercises using weight disks, rubber bands, dumbbells, medical balls and shin guards with weights—biceps curl, triceps extension, chest press, and handgrip with different degrees of tension. |
Reduction in the BMI (p < 0.0001) and the skin fold of the twin (p = 0.008);
® InnerScan (BC-533, Tanita Corporation of America, Inc., Clearbrook, IL, USA);
BMI = weight ÷ (height2); | 1 |
6 |
| increased isometric strength ( | p | < 0.0001). |
| percentage of fat—subcutaneous triceps and calf sites;
isometric strength—manual dynamometer—(dominant hand) MSD, (model SH5001, Düsseldorf, Germany). |
Rosety-Rodriguez. et al. [12] |
s |
| Rosety-Rodriguez et al. [ | 1 |
12 | 0 |
1 |
-- |
1 |
1 |
1 |
1 |
1 |
7 |
Rosety-Rodriguez et al. [12]
Spain |
]Effect of ST on low-grade systemic inflammation in DS adults. |
12 weeks;
3 × week;
N = 40 ♂; age: 23.7 ± 3.1;
DS (IQ: 60–69);
randomized groups:
GE: N = 24 | CG: N = 16. |
Prospective cohort. |
session duration ND. |
Exercises included arm curl, leg extension, seated row, leg curl, triceps extension, and leg press;
40 to 65% of 8 RM;
2 sets; 6 to 10 rep.Blood samples—plasma levels of leptin, adiponectin, interleukin-6 and TNF-α (ELISA kits); |
Plasma levels of leptin (p < 0.05), TNF-α (p < 0.05) and IL-6 (p < 0.05) and waist circumference decreased (p = 0.0416);
increase in fat-free mass (p = 0.011);
improved response to systemic inflammation.
C-reactive protein—nephelometry;
fat-free mass percentage—bio impedance (Tanita TBF521, Tanita Corporation of America, Inc., Clearbrook, IL, USA);
waist circumference—anthropometric tape; |
Rosety-Rodriguez et al. [13] |
s |
1 |
1 |
| Rosety-Rodriguez et al. [13 | 1 |
] |
12 weeks; | - |
3 × week;
| - |
Session duration ND. |
Exercises included arm curl, leg extension, seated row, leg curl, triceps extension, and | 0 |
leg press;
| 1 |
1 |
1 |
1 |
7 |
| time up-and-go test (Rikli and Jones, 1999). |
40 to 50% of 8 RM;
2 sets; 8 to 10 rep; 90s rest. |
Improvement of the antioxidant defense system;
|
Shields and Taylor [14 |
| Rosety-Rodriguez et al. | reduction in markers of oxidative damage. |
] |
s |
1 |
1 |
1 |
- |
- |
1 |
1 |
1 |
1 |
1 |
8 |
| Shields and Taylor [14] |
10 weeks;
2 × week;
session duration ND. |
Exercises: lat pull-down, seated chest press, seated row, seated
leg press, knee extension, calf raise;
3 sets; 12 rep or until fatigue;
2 min rest between exercises. |
Improvement in muscle strength of the lower limbs (mean difference 36 kg, 95% CI 15 to 58). |
Shields et al. [15] |
s |
| Shields et al. | 1 |
[ | 1 |
1 |
15 | - |
- |
] | 1 |
1 |
10 weeks;
2 × week;
60 min/session. |
Exercises: lat pull-down, seated chest press, seated row, seated
leg press, knee extension, seated calf raise;
3 sets; 12 rep; 60 to 80% RM;
| 1 |
1 |
1 |
8 |
Tabela 2. Avaliação da qualidade dos artigos, por meio da escala PEDro, bem como sua pontuação total.
Table 2 shows the aims, the participants, study designs and the assessment of the instruments/techniques used in the studies included.
| 2 min rest between exercises. |
| Improvement in muscle strength of the lower 1imbs (mean difference 25 kg, 95% CI 8 to 42) and upper limbs 1 (mean difference 7 kg, 95% CI 3 to 11). |
Tabela 4. Características dos protocolos de treinamento de força dos nove estudos.2.6. Characteristics of the Strength Training Protocols
2.6. Características dos protocolos de treinamento de força
Table 3 shows the characteristics of the ST protocols. The programs’ duration varied between 8 and 16 weeks, with half the studies prescribing 12 weeks [7][10][12][13]. The weekly frequency varied between two and five times, with a greater number of studies showing a weekly frequency of three sessions [7][8][9][10][12][13]. The training sessions duration varied between 45 and 60 min.A Tabela 4 mostra as características dos protocolos ST. A duração dos programas variou entre 8 e 16 semanas, com metade dos estudos prescrevendo 12 semanas [ 39 , 42 , 44 , 45 ]. A frequência semanal variou de duas a cinco vezes, com maior número de estudos mostrando uma frequência semanal de três sessões [ 39 , 40 , 41 , 42 , 44 , 45 ]. A duração das sessões de treinamento variou entre 45 e 60 min.
The protocols adopted varied from study to study. Six studies applied circuits in ST machines [7][10][12][13][14][15], one study included exercise performed in two surfaces conditions (firm and foam) [9], one study applied exercises with free weights [13], and one study applied an abdominal workout [8].Os protocolos adotados variaram de estudo para estudo. Seis estudos aplicaram circuitos em máquinas ST [ 39 , 42 , 44 , 45 , 46 , 47 ], um estudo incluiu exercícios realizados em duas condições de superfícies (firme e espuma) [ 41 ], um estudo aplicou exercícios com pesos livres [ 45 ], e um estudo aplicou um treino abdominal [ 40 ].
All studies showed a positive effect from the different ST protocols, which can be seen in Table 3.Todos os estudos mostraram efeito positivo dos diferentes protocolos de TS, o que pode ser observado na Tabela 4 .
3. Current Insights3. Percepções atuais
The present systematic review aims to analyze the effects of ST in individuals with ID, based on the characterization of several programs implemented, as well as the identification of mean characteristics for ST prescription programs, namely duration, weekly frequency, appropriate assessment methods, and type of exercises. The following subsections will discuss all main point of the ST programs applied.A presente revisão sistemática tem como objetivo analisar os efeitos do TS em indivíduos com DI, a partir da caracterização de diversos programas implantados, bem como na identificação de características médias para programas de prescrição de TS, a saber, duração, frequência semanal, métodos de avaliação adequados e tipo de exercícios. As subseções a seguir discutirão todos os pontos principais dos programas ST aplicados.
3.1. Program Duration
3.1. Duração do programa
As mentioned in the results section, the programs’ durations varied between 8 and 16 weeks, with half the studies prescribing 12 weeks [7][10][12][13]. Short-term intervention programs may be a limitation presented in some studies [7][14]. Although all studies have shown several positive results (Table 1), further studies with a longer duration are needed to understand the long-term benefits, as well as the type of ST periodization to be applied in the population with ID. We consider that the duration of the training programs is critical to outwit if there are individuals who do not experience significant improvements following an exercise training intervention. Such individuals are commonly termed “non-responders”. However, recently, many researchers have taken a skeptical view as to whether exercise non-response either exists, or is clinically relevant.Conforme mencionado na seção de resultados, a duração dos programas variou entre 8 e 16 semanas, com metade dos estudos prescrevendo 12 semanas [ 39 , 42 , 44 , 45 ]. Programas de intervenção de curto prazo podem ser uma limitação apresentada em alguns estudos [39,46. Embora todos os estudos tenham mostrado vários resultados positivos ( Tabela 2), são necessários mais estudos com maior duração para entender os benefícios em longo prazo, bem como o tipo de periodização de TS a ser aplicada na população com DI. Consideramos que a duração dos programas de treinamento é crítica para enganar se houver indivíduos que não experimentaram melhorias significativas após uma intervenção de treinamento de exercício. Esses indivíduos são comumente chamados de “não respondentes”. No entanto, recentemente, muitos pesquisadores têm assumido uma visão cética quanto à existência ou não de relevância clínica para a não resposta ao exercício.
3.2. Frequency
3.2. Frequência
The weekly frequency followed the recommendations of the American College of Sports Medicine (ACSM) [16]; once weekly frequency occurred between two and five times. This number of weekly TS sessions allows adaptations that lead to catabolism and consequent protein anabolism, allowing the maintenance or increase in lean mass [1]. Moreover, except for Ortiz-Ortiz et al. [11], all the other studies did not report sessions on consecutive days. It is important to reinforce that even the study of Ortiz-Ortiz et al. [11] improved the BMI (p < 0.0001) and skin fold of the calf (p = 0.008), which suggests future studies should confirm such results.A frequência semanal seguiu as recomendações do American College of Sports Medicine (ACSM) [ 48 ]; uma vez por semana, a frequência ocorreu entre duas e cinco vezes. Esse número de sessões semanais de TS permite adaptações que levam ao catabolismo e consequente anabolismo protéico, permitindo a manutenção ou aumento da massa magra [ 24 ]. Além disso, exceto Ortiz-Ortiz et al. [ 43 ], todos os outros estudos não relataram sessões em dias consecutivos. É importante reforçar que mesmo o estudo de Ortiz-Ortiz et al. [ 43 ] melhoraram o IMC ( p <0,0001) e a dobra cutânea da panturrilha ( p = 0,008), o que sugere que estudos futuros devem confirmar tais resultados.
3.3. Session Duration
3.3. Duração da Sessão
The training sessions duration varied between 45 and 60 min and their structure consisted of warm-up, main phase, and a return to calm/cool down, which is in accordance with the ACSM guidelines [16]. However, some studies did not mention the session duration [7][12][13][14], which is a limitation, leaving some doubts about the recovery period that was applied, as well as the replicability of the studies.A duração das sessões de treinamento variou entre 45 e 60 min e sua estrutura consistiu em aquecimento, fase principal e retorno à calma / resfriamento, o que está de acordo com as diretrizes do ACSM [ 48 ]. No entanto, alguns estudos não mencionaram a duração da sessão [ 39 , 44 , 45 , 46 ], o que é uma limitação, deixando algumas dúvidas sobre o período de recuperação aplicado, bem como a replicabilidade dos estudos.
3.4. Sets
3.4. Jogos
The number of sets per exercise varied between two and six, depending on the progress and training periodization. However, the prescription of two or three sets was more frequent [7][10][12][13][14][15], in accordance with ACSM [16]. Some authors state that, in untrained individuals, both single set and multiple sets produce similar increases in muscle strength of upper and lower limbs; that is, in the early stages, the RT, regardless of number of sets, seems to be effective for improving muscle outcomes [17].O número de séries por exercício variou de duas a seis, dependendo do progresso e da periodização do treinamento. Porém, a prescrição de duas ou três séries foi mais frequente [ 39 , 42 , 44 , 45 , 46 , 47 ], de acordo com o ACSM [ 48 ]. Alguns autores afirmam que, em indivíduos não treinados, tanto as séries únicas quanto as múltiplas produzem aumentos semelhantes na força muscular dos membros superiores e inferiores; ou seja, nos estágios iniciais, o TR, independentemente do número de séries, parece ser eficaz para melhorar os resultados musculares [ 49 ].
3.5. Repetitions
3,5. Repetições
The number of repetitions per set varied between 6 and 30; however, most studies prescribed 6 to 12 repetitions [7][10][12][15]. This number is influenced by the prescription of one RM methods or the use of a number of repetitions by exercise (not one RM). The number of sets and repetitions per exercise can vary depending on volume and intensity [18]. This number follows previous recommendations for healthy people [19].O número de repetições por série variou entre 6 e 30; no entanto, a maioria dos estudos prescreveu 6 a 12 repetições [ 39 , 42 , 44 , 47 ]. Este número é influenciado pela prescrição de um método de RM ou pelo uso de várias repetições por exercício (não um RM). O número de séries e repetições por exercício pode variar dependendo do volume e intensidade [ 50 ]. Este número segue recomendações anteriores para pessoas saudáveis [ 51 ].
3.6. Intensity
3,6. Intensidade
ST programs presented different training intensities according to the different objectives established for the development of strength adaptations (endurance, resistance, power, etc.). The intensity expressed through the percentage of the working load expressed by the number of RM varied between 40 to 65% of 8 RM [7][12], from 40 to 50% of 8 RM [13], and from 60 to 90% of 1 RM [15]. Different purposes, different available material resources and/or individual characteristics may be some of the reasons to justify such a range of training intensities used in the different studies, not fulfilling the usual recommendations suggested by the ACSM [16]—75–80% 1 RM. Despite the reported use of different intensities, in general, the ACSM guidelines [16] were applied and all studies reported a positive effect (see ST results section).Os programas de TF apresentaram diferentes intensidades de treinamento de acordo com os diferentes objetivos estabelecidos para o desenvolvimento das adaptações de força (endurance, resistência, potência, etc.). A intensidade expressa através da porcentagem da carga de trabalho expressa pelo número de RM variou de 40 a 65% de 8 RM [ 39 , 44 ], de 40 a 50% de 8 RM [ 45 ], e de 60 a 90% de 1 RM [ 47 ]. Diferentes finalidades, diferentes recursos materiais disponíveis e / ou características individuais podem ser alguns dos motivos para justificar tal gama de intensidades de treinamento utilizadas nos diferentes estudos, não atendendo às recomendações usuais sugeridas pelo ACSM [ 48] —75–80% 1 RM. Apesar do uso relatado de intensidades diferentes, em geral, as diretrizes do ACSM [ 48 ] foram aplicadas e todos os estudos relataram um efeito positivo (consulte a seção de resultados de ST).
The application of the training progression general principle was common to several studies [8][9][11][13][14][15], with an increase in intensity throughout the intervention period, regardless of the type of material/equipment used (whether the programs used weight machines, free weights, rubber bands, or other materials). The progression of the intensity increased gradually, depending on the number of training weeks or individual performance, either by increasing the percentage of the training load (by increasing the weight in the ankle shin guards), or simply by increasing the number of series and/or repetitions to perform during the training session, as recommended by the ACSM [16][18].A aplicação do princípio geral de progressão do treinamento foi comum a diversos estudos [ 40 , 41 , 43 , 45 , 46 , 47 ], com aumento da intensidade ao longo do período de intervenção, independente do tipo de material / equipamento utilizado (sejam os programas máquinas de musculação usadas, pesos livres, elásticos ou outros materiais). A progressão da intensidade aumentou gradativamente, dependendo do número de semanas de treinamento ou desempenho individual, seja pelo aumento da porcentagem da carga de treinamento (pelo aumento do peso nas caneleiras), ou simplesmente pelo aumento do número de séries e / ou repetições a realizar durante a sessão de treinamento, conforme recomendado pelo ACSM [48 , 50 ].
3.7. Exercises
3,7. Exercícios
According to the studies evaluated [8][11][13][14][15], most ST programs included exercises targeting the main muscle groups in each session. Although the studies analyzed use different types of equipment (weight training machines, using resistance elastics, and/or ankle weights), all of them show intentionality to use ST exercises aiming to request the main muscle group [18]. It should be noted that only two studies used a period of adaptation and familiarization to the prescribed exercises [20][21], which is important to eliminate the fear of using new materials, movement perception, and to ensure high quality results. The most common exercises used in the ST programs are the leg flexion and leg extension exercises (hamstrings and quadriceps), the abdominals in their different variants (abdomen muscles), the chest press (pectoral major), the low row or the lat pull down (latissimus dorsi), flexion of the forearm (biceps), an extension of the forearm (triceps), and elevation, abduction, or shoulder press (deltoids). When prescribing six to eight exercises, ST programs were in accordance with the recommendations provided by ACSM [16], however, in some studies, this was not the case [8][10]. In the majority of the studies, selected exercises tended to be simple and easy to be performed, with special attention and reinforcement in the instruction, demonstration, and familiarization [16][20][21]. Some individuals may experience difficulties in controlling movement, particularly in the eccentric phase, and thus it was suggested to use machines that help to better control them (for example, a chest press device rather than the bench press). Additionally, machine exercises are preferable to avoid some type of injury, for presenting a smaller range of motion; however, there were some exceptions such as the biceps curl, seen as working well in participants with ID [18].De acordo com os estudos avaliados [ 40 , 43 , 45 , 46 , 47 ], a maioria dos programas de ST incluiu exercícios direcionados aos principais grupos musculares em cada sessão. Embora os estudos analisados utilizem diferentes tipos de equipamentos (aparelhos de musculação, utilizando elásticos de resistência e / ou pesos de tornozelo), todos eles mostram intencionalidade em utilizar exercícios de TF com o objetivo de solicitar o grupo muscular principal [ 50 ]. Deve-se notar que apenas dois estudos utilizaram um período de adaptação e familiarização aos exercícios prescritos [ 52 , 53], importante para eliminar o medo de usar novos materiais, percepção de movimento e garantir resultados de alta qualidade. Os exercícios mais comuns usados nos programas de ST são os exercícios de flexão e extensão de pernas (isquiotibiais e quadríceps), os abdominais em suas diferentes variantes (músculos abdominais), o supino torácico (peitoral maior), a remada baixa ou o puxão lateral (latissimus dorsi), flexão do antebraço (bíceps), uma extensão do antebraço (tríceps) e elevação, abdução ou pressão do ombro (deltóide). Ao prescrever seis a oito exercícios, os programas de ST estavam de acordo com as recomendações fornecidas pelo ACSM [ 48 ], no entanto, em alguns estudos, esse não foi o caso [ 40 , 42] Na maioria dos estudos, os exercícios selecionados tendiam a ser simples e fáceis de serem realizados, com atenção especial e reforço na instrução, demonstração e familiarização [ 48 , 52 , 53 ]. Alguns indivíduos podem ter dificuldade em controlar o movimento, principalmente na fase excêntrica, e por isso foi sugerido o uso de máquinas que ajudem a controlá-los melhor (por exemplo, um aparelho de supino ao invés do supino). Além disso, exercícios com máquina são preferíveis para evitar algum tipo de lesão, por apresentarem uma menor amplitude de movimento; no entanto, houve algumas exceções, como a rosca direta para bíceps, vista como funcionando bem em participantes com DI [ 50 ].
3.8. ST Programs Outcomes
3,8. Resultados de programas de ST
Some studies have shown significant positive effects on muscle strength in lower limbs [14], in upper and lower limbs [15], and in handgrip strength (p < 0.0001) [11]. These results are very encouraging for further studies with this population and to implement in clinical practice. A greater capacity to generate strength by the muscles (lower and upper limbs) may become an essential tool to insert these patients in professional activities due to the increase in their physical capacities [14].Alguns estudos demonstraram efeitos positivos significativos na força muscular dos membros inferiores [ 46 ], nos membros superiores e inferiores [ 47 ] e na força de preensão manual ( p <0,0001) [ 43 ]. Esses resultados são muito encorajadores para novos estudos com essa população e para implementação na prática clínica. Uma maior capacidade de geração de força pelos músculos (membros inferiores e superiores) pode se tornar uma ferramenta essencial para inserir esses pacientes nas atividades profissionais devido ao aumento de suas capacidades físicas [ 46 ].
Other studies found an increase in fat-free mass and a reduction in fat mass [10][11][12]. Depending on the aims and evaluation methods used, some studies reported a reduction in the waist circumference [12] of the BMI [11] and an improvement in balance [8].Outros estudos encontraram um aumento na massa livre de gordura e uma redução na massa gorda [ 42 , 43 , 44 ]. Dependendo dos objetivos e métodos de avaliação usados, alguns estudos relataram uma redução na circunferência da cintura [ 44 ] do IMC [ 43 ] e uma melhora no equilíbrio [ 40 ].
An increase in the concentration of salivary immunoglobulin, testosterone levels, plasma leptin levels, TNF-α, and IL-6 was also found. Specifically, Fornieles et al. [7] showed thar resistance training program of 12 weeks increased concentration of salivary immunoglobulin (p = 0.0120), testosterone levels (p = 0.0088) and task performance (p = 0.0141). This study highlights the benefits of ST, as this increase in salivary IgA levels can prevent respiratory tract infections in individuals with DS [22]. This study also shows an improvement in the anabolic status of DS patients after the ST program, as cortisol levels remain unchanged and there was an increase in salivary testosterone. It was also found that the improvement of task performance is of great interest to this population. Having improved levels of muscle strength may allow this population to perform a greater number of activities and continue to exercise, thus reducing the risk of secondary consequences for their health [23][24]. Additionally, improvements in the response to systemic inflammation, in the antioxidant defense system, and a reduction in oxidative damage were also reported [7][12][13].Também foi encontrado aumento na concentração de imunoglobulina salivar, níveis de testosterona, níveis plasmáticos de leptina, TNF-α e IL-6. Especificamente, Fornieles et al. [ 39 ] mostraram que o programa de treinamento resistido de 12 semanas aumentou a concentração de imunoglobulina salivar ( p = 0,0120), os níveis de testosterona ( p = 0,0088) e o desempenho na tarefa ( p = 0,0141). Este estudo destaca os benefícios do TS, visto que esse aumento nos níveis de IgA salivar pode prevenir infecções do trato respiratório em indivíduos com SD [ 54] Este estudo também mostra uma melhora no estado anabólico de pacientes com SD após o programa de ST, uma vez que os níveis de cortisol permanecem inalterados e houve aumento da testosterona salivar. Verificou-se também que a melhoria do desempenho das tarefas é de grande interesse para essa população. Ter melhores níveis de força muscular pode permitir que essa população realize um maior número de atividades e continue a se exercitar, reduzindo assim o risco de consequências secundárias para sua saúde [ 55 , 56 ]. Além disso, melhorias na resposta à inflamação sistêmica, no sistema de defesa antioxidante e uma redução no dano oxidativo também foram relatadas [ 39 , 44 , 45 ].
Dynamic balance as a parameter of functional capacity is also limited in individuals with ID. Even so, two studies reported improvements with ST, particularly in exercises focused to improve strength and power of the lower limbs [8][14]. These improvements were also associated with improvements in gait speed and balance [14]. Other non-randomized controlled studies have shown interesting results through the implementation of ST programs in individuals with ID, namely, cognitive effects such as positive changes in working memory, short-term memory, vocabulary knowledge, and reasoning ability [25], and improved flexibility [26] and performance in daily life activities [27]. There is an urgent need for randomized procedures to assess the benefits of these variables and aerobic capacity. Several studies have found significant differences in body composition parameters after the strength training program, namely a reduction in the BMI (p < 0.0001) and the skin fold of the calf (p = 0.008) [11]; a decreased in waist circumference (p = 0.0416) and increase in the fat-free mass (p = 0.011) [12]; and an increased in the lean mass (p = 0.008) and reduction in the fat percentage (p = 0.036) [11]. Since being overweight and obesity are associated with poor health and quality of life, these results show that strength training is a good intervention to reduce these values.O equilíbrio dinâmico como parâmetro da capacidade funcional também é limitado em indivíduos com DI. Mesmo assim, dois estudos relataram melhorias com o TS, principalmente em exercícios voltados para melhorar a força e a potência dos membros inferiores [ 40 , 46 ]. Essas melhorias também foram associadas a melhorias na velocidade da marcha e equilíbrio [ 46 ]. Outros estudos controlados não randomizados mostraram resultados interessantes por meio da implementação de programas de TS em indivíduos com DI, ou seja, efeitos cognitivos, como mudanças positivas na memória de trabalho, memória de curto prazo, conhecimento de vocabulário e capacidade de raciocínio [ 57 ], e melhora flexibilidade [ 58 ] e desempenho nas atividades da vida diária [ 59] Há uma necessidade urgente de procedimentos randomizados para avaliar os benefícios dessas variáveis e da capacidade aeróbia. Vários estudos encontraram diferenças significativas nos parâmetros de composição corporal após o programa de treinamento de força, a saber: redução do IMC ( p <0,0001) e da dobra cutânea da panturrilha ( p = 0,008) [ 43 ]; diminuição da circunferência da cintura ( p = 0,0416) e aumento da massa magra ( p = 0,011) [ 44 ]; e aumento da massa magra ( p = 0,008) e redução do percentual de gordura ( p = 0,036) [ 43] Como o sobrepeso e a obesidade estão associados a problemas de saúde e qualidade de vida, esses resultados mostram que o treinamento de força é uma boa intervenção para reduzir esses valores.
With the implementation of ST programs, despite the different prescriptions, positive results were verified in terms of the aims defined in all studies, which shows how training variables, techniques, and methods (for example, training frequency and exercise selection volume, training load and repetitions, and others), can be manipulated to optimize training response. The different results presented in Table 3 and of the non-randomized controlled studies [25][26][27] are demonstrated due to the different aims and evaluation methods used in each study, being an added value the application of ST, since it can have this wide range of benefits. All these results are important in terms of promoting the quality of life of individuals with ID, related to the conceptual model of Schalock et al. [28], a construct divided into three dimensions: (i) independence; (ii) social participation; (iii) well-being.Com a implantação dos programas de TF, apesar das diferentes prescrições, verificaram-se resultados positivos em relação aos objetivos definidos em todos os estudos, o que mostra como as variáveis, técnicas e métodos de treinamento (por exemplo, frequência de treinamento e volume de seleção de exercícios, carga de treinamento e repetições e outros), podem ser manipulados para otimizar a resposta do treinamento. Os diferentes resultados apresentados na Tabela 4 e dos estudos controlados não randomizados [ 57 , 58 , 59] são demonstrados devido aos diferentes objetivos e métodos de avaliação utilizados em cada estudo, sendo uma mais-valia a aplicação do TS, uma vez que pode ter este amplo leque de benefícios. Todos esses resultados são importantes para a promoção da qualidade de vida dos indivíduos com DI, relacionados ao modelo conceitual de Schalock et al. [ 60 ], um construto dividido em três dimensões: (i) independência; (ii) participação social; (iii) bem-estar.
Some studies included in the systematic review have some limitations, which may limit the magnitude of the results. Future studies should take them into account when implementing ST programs: (i) short-term studies [7][12][15]; (ii) no follow up to determine whether the positive effects were maintained [7][12][13][15]; (iii) small sample size [9]; (iv) sample size only boys [9]; (v) exclusion of children with severe and profound ID [9]; (vi) a small number of professionals to supervise the exercises produced in the experimental protocol [10]; (vii) lack of more accurate measurements to evaluate; and (viii) a small number of outcomes [15].Alguns estudos incluídos na revisão sistemática apresentam algumas limitações, que podem limitar a magnitude dos resultados. Estudos futuros devem levá-los em consideração ao implementar programas de TS: (i) estudos de curto prazo [ 39 , 44 , 47 ]; (ii) nenhum acompanhamento para determinar se os efeitos positivos foram mantidos [ 39 , 44 , 45 , 47 ]; (iii) pequeno tamanho da amostra [ 41 ]; (iv) tamanho da amostra apenas meninos [ 41 ]; (v) exclusão de crianças com DI grave e profundo [ 41 ]; (vi) um pequeno número de profissionais para supervisionar os exercícios produzidos no protocolo experimental [ 42]; (vii) falta de medidas mais precisas para avaliar; e (viii) um pequeno número de resultados [ 47 ].
At the same time, future studies are suggested to apply the assessment of body composition variables by electrical bioimpedance, such as the phase angle, since it has been considered a relevant marker of health status [29]. Moreover, a higher phase angle value is positively associated with a higher quality of cell membranes [30], while a lower value is associated with deterioration, which can compromise all cell functions [30]. Thus, phase angle assessment would be helpful to understand if there are adaptations with ST in this variable that has a strong correlation with cell health and integrity, being an excellent indicator of the capacity of the cell membrane to retain liquids, fluids, and nutrients in the population with ID.Ao mesmo tempo, sugere-se que estudos futuros apliquem a avaliação de variáveis da composição corporal por bioimpedância elétrica, como o ângulo de fase, por ter sido considerado um marcador relevante do estado de saúde [ 61 ]. Além disso, um valor de ângulo de fase mais alto está positivamente associado a uma qualidade superior das membranas celulares [ 62 ], enquanto um valor mais baixo está associado à deterioração, que pode comprometer todas as funções celulares [ 62 ]. Assim, a avaliação do ângulo de fase seria útil para entender se há adaptações com ST nesta variável que tem forte correlação com a saúde e integridade celular, sendo um excelente indicador da capacidade da membrana celular em reter líquidos, fluidos e nutrientes em a população com ID.
The fact that ID is a multisystem and complex disorder characterized by the presence of delays or deficits in the development of adaptive behavior comprising conceptual, social, and motor skills may support a possible explanation why results could differ between studies and studies without the RCT method. The effects of the interventions in the various studies appear similar to those that have been reported following resistance training in the average healthy and intellectually disabled population [31][32][2][33][34]. However, some variability has also been reported in other resistance training studies and those examining other exercise modalities [35][6][14][15][25]. Inherent within any measurement are both technical error and random within-subject variation [36]. Studies included in this systematic review have shown that, although using different training intensities, it was possible to identify improvements in the variables under study; however, it is noted that, before starting the training program, it is necessary to carry out strength assessments, either through RM tests, using devices, or isokinetic, as recommended by ACSM [16], to determine the correct intensity to be used. During this strength assessment process, as during training, RM tests using free weights, push-ups, and pull-ups should be avoided [16] to prevent any type of injury. Moreover, familiarization with the assessment procedures, a practical demonstration of execution, simple instructions, constant supervision, and verbal and visual reinforcement are necessary [16][21] for greater success in the didactic-pedagogical process.O fato de o DI ser um transtorno multissistêmico e complexo caracterizado pela presença de atrasos ou déficits no desenvolvimento do comportamento adaptativo compreendendo habilidades conceituais, sociais e motoras pode apoiar uma possível explicação de porque os resultados podem diferir entre estudos e estudos sem o método RCT. Os efeitos das intervenções nos vários estudos parecem semelhantes aos que foram relatados após o treinamento de resistência na população média saudável e com deficiência mental [ 3 , 22 , 25 , 30 , 33 ]. No entanto, alguma variabilidade também foi relatada em outros estudos de treinamento de resistência e aqueles que examinam outras modalidades de exercício [ 20 , 29 ,46 , 47 , 57 ]. Inerentes a qualquer medição estão tanto o erro técnico quanto a variação aleatória dentro do sujeito [ 63 ]. Os estudos incluídos nesta revisão sistemática mostraram que, embora utilizando diferentes intensidades de treinamento, foi possível identificar melhorias nas variáveis em estudo; entretanto, ressalta-se que, antes de iniciar o programa de treinamento, é necessário realizar avaliações de força, seja por meio de testes de RM, por meio de aparelhos, ou isocinética, conforme preconizado pelo ACSM [ 48 ], para determinar a intensidade correta a ser utilizada. Durante este processo de avaliação de força, como durante o treinamento, os testes de RM usando pesos livres, flexões e flexões devem ser evitados [ 48] para prevenir qualquer tipo de lesão. Além disso, familiarização com os procedimentos de avaliação, demonstração prática de execução, instruções simples, supervisão constante e reforço verbal e visual são necessários [ 48 , 53 ] para maior sucesso no processo didático-pedagógico.
This systematic review analyzed the effects of ST in individuals with intellectual disability, aiming to be a reference guidelines tool for researchers and professionals of PE. The analyzed studies show characteristics and recommendations that professionals can follow when implementing an ST program to promote benefits and positive outcomes, namely, the maintenance of/increase in physical fitness, quality of life, and health, thus decreasing the risk of developing chronic diseases, being the strong aspect of this systematic review. Therefore, it is essential to implement this type of ST program, incorporated into the weekly routine of this population, which, when associated with an appropriate lifestyle, causes a set of adaptations and benefits and, ultimately, can promote a decrease in clinical expenses, an increase in healthy aging, and better health.Esta revisão sistemática analisou os efeitos do TS em indivíduos com deficiência intelectual, com o objetivo de ser uma ferramenta de orientação de referência para pesquisadores e profissionais da EF. Os estudos analisados apresentam características e recomendações que os profissionais podem seguir na implementação de um programa de TS para promover benefícios e resultados positivos, a saber, a manutenção / aumento da aptidão física, qualidade de vida e saúde, diminuindo assim o risco de desenvolver doenças crônicas, sendo o aspecto forte desta revisão sistemática. Portanto, é imprescindível a implantação desse tipo de programa de TS, incorporado à rotina semanal dessa população, que, quando associado a um estilo de vida adequado, provoca um conjunto de adaptações e benefícios e, em última instância, pode promover a diminuição dos gastos clínicos, um aumento no envelhecimento saudável,
It is recommended to increase the implementation of ST programs in the target population, expanding the knowledge in terms of the methods, structure, and duration used, so that professionals can prescribe adapted and effective ST programs. At the same time, it is important that the exercise professionals have an in-depth knowledge of the individual, their comorbidities, limitations, and preferences, before prescribing and starting a PE program [18].Recomenda-se aumentar a implantação de programas de TS na população-alvo, ampliando o conhecimento quanto aos métodos, estrutura e duração utilizados, para que os profissionais possam prescrever programas de TS adaptados e eficazes. Ao mesmo tempo, é importante que os profissionais de exercício tenham um conhecimento profundo do indivíduo, suas comorbidades, limitações e preferências, antes de prescrever e iniciar um programa de EF [ 50 ].
Despite the relevance of the selected clinical trials for the preparation of this systematic review, some limitations can be observed: (1) the diversified intervention methodology, involving different strengths, intensities, volumes, and weekly training exercise programs; (2) unclear descriptions of the process of randomization and allocation of people with ID in the groups; (3) loss of follow-up; (4) different evaluation methodologies, as well as the results, not allowing a further discussion as well as a meta-analysis about the effects produced by the several ST programs applied; (5) the level of ID was not mentioned in all studies included, which limits the generalization of the results and suggests that future studies should mention such specificity.Apesar da inclusão dos ensaios clínicos selecionados para a elaboração desta revisão sistemática, algumas limitações podem ser observadas: (1) a metodologia de intervenção diversificada, envolvendo diferentes, intensidades, volumes e programas semanais de exercícios de treinamento; (2) descrições pouco claras do processo de randomização e alocação de pessoas com DI nos grupos; (3) perda de seguimento; (4) diferentes metodologias de avaliação, bem como dos resultados, não permitindo uma discussão mais aprofundada e também uma meta-análise sobre os resultados obtidos pelos diversos programas de TS;(5) o nível de DI não foi incluído em todos os estudos incluídos, o que limita a generalização dos resultados e necessários que estudos futuros devem mencionar tal especificidade.