Endoscopic ultrasonography (EUS) has greater spatial resolution than other diagnostic imaging modalities. In addition, if gallbladder lesions are found and gallbladder cancer is suspected, EUS is an indispensable modality, enabling detailed tests for invasion depth evaluation using the Doppler mode and ultrasound agents. Furthermore, for gallbladder lesions, EUS fine-needle aspiration (EUS-FNA) can be used to differentiate benign and malignant forms of conditions, such as xanthogranulomatous cholecystitis, and collect evidence before chemotherapy.
- Endoscopic ultrasonography (EUS)
- EUS fine-needle aspiration (EUS-FNA)
- gallbladder carcinoma
- xanthogranulomatous
- cholecystitis gallbladder lesions
1. Introduction
Endoscopic ultrasonography (EUS) plays a major role in the diagnosis of gallbladder lesions. The digitization of diagnostic ultrasound imaging devices and advancements in ultrasound contrast media help obtain the blood flow information with the Doppler-mode and contrast-enhanced EUS, and more detailed EUS investigations can be performed to determine the presence of gallbladder lesions and invasion depth for suspected gallbladder cancer. In some cases, EUS combined with fine-needle aspiration (EUS-FNA) is also useful for distinguishing between benign and malignant gallbladder lesions. This review outlines the use of EUS in the diagnosis of gallbladder lesions.
2. EUS for Gallbladder Lesions
Table 1 presents the classification of gallbladder lesions. Gallbladder lesions are classified as neoplastic or non-neoplastic based on their microscopic structure and invasive characteristics ( Table 1 ). In cases of suspected gallbladder cancer, clinical practice guidelines for the management of biliary tract cancers [1] recommend diagnostic imaging, including EUS, as the third diagnostic step for all gallbladder cancers.
Table 1. Classification of gallbladder lesion.
| High-to-Intermediate Frequency | Low Frequency | ||
|---|---|---|---|
| Neoplastic | Adenocarcinoma Adenosquamous carcinoma |
Adenoma Carcinosarcoma Metastatic tumor Neuroendocrine tumor Malignant lymphoma |
|
| Non-Neoplastic | Elevated lesion | Cholesterol polyp | Hyperplastic polyp Metaplastic polyp Inflammatory polyp Fibrous polyp |
| Flat or thickened wall lesion | Cholecystitis Adenomyomatosis Hyperplastic change (associated with the pancreas bile duct maljunction) |
||
EUS is performed using an endoscope equipped with an ultrasound probe. High ultrasound frequencies (5 mHz to 20 mHz) are used for EUS, and it has a high spatial resolution, thereby facilitating a detailed examination of the gallbladder because it can approach and examine the organ at a closer range than the conventional US [2,3,4]. This helps in the qualitative diagnosis of lesions and evaluation of tumor invasion depth [5]. However, because the position of the gallbladder can differ between individuals, visualizing the entire gallbladder is occasionally difficult, particularly the gallbladder fundus. For this reason, different imaging modalities, such as abdominal ultrasonography (US), computed tomography (CT), or magnetic resonance cholangiopancreatography (MRCP), must be used before EUS is performed.
There are two types of EUS scopes for radial scanning and convex array. The devices used for these provide different types of images and are therefore used in various visualization methods. Kaneko et al. [6] reported that there was no significant difference in visualization between these two types of devices in the examination of the pancreaticobiliary region.
3. Diagnosis of Gallbladder Tumor
Diseases that require a differential diagnosis from pedunculated-type gallbladder cancer include cholesterol polyps, gallbladder adenomas, inflammatory polyps, and fibrous polyps ( Table 1 ). Cholesterol polyps account for approximately 95% of raised gallbladder lesions and occur when histiocytes (foamy cells) ingest cholesterol esters, accumulate under the mucosal epithelium, and expand to form polyp-shaped growths. These polyps can break off, leading to complications similar to those caused by small gallstones [14]. During EUS, cholesterol polyps typically appear as multiple lesions and are homogeneous, pedunculated, and smaller than ≤4 mm; polyps are also generally more hyperechoic than the liver parenchyma or gallbladder wall [12,14,15]. However, as the cholesterol polyp grows, the echo intensity inside the polyp may decrease; when this occurs, the cholesterol polyp cannot be easily differentiated from adenoma or cancer. Another study on gallbladder polyps ≥10 mm used contrast-enhanced EUS to diagnose benign or malignant polyps based on the presence of an irregular contrast pattern and reported a 90.3% sensitivity and 96.6% specificity for this method [16].
Gallbladder adenoma, which can exhibit premalignant behavior ( Figure 21 ), is a rare condition that accounts for 10% of ultrasonographically diagnosed gallbladder polyps [14]. It is usually solitary, 5–20 mm in size, and can be sessile or pedunculated [14,17,18]. Gallbladder adenomas have four histological types: pyloric, intestinal, foveolar, and biliary. Histologically, 70% of gallbladder adenomas are tubular adenomas of the pyloric gland. Pyloric gland tubular adenoma of the gallbladder is characterized by multiple microcysts inside a polyp; however, it is difficult to distinguish between cancer and this type of adenoma.
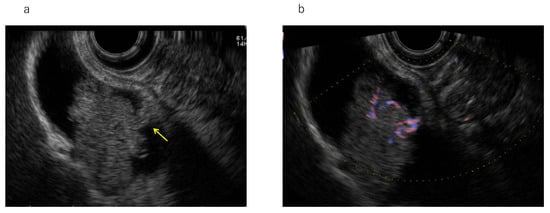
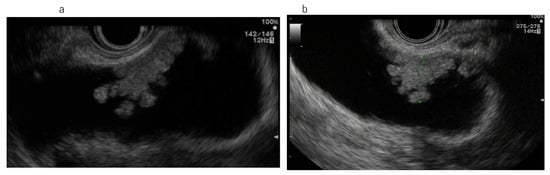
Gallbladder adenomas are generally homogeneous polyps, often isoechoic, contain liver parenchyma, and are sessile or pedunculated. An intralesional vascular spot may be observed on color Doppler investigation [14]. Using contrast-enhanced EUS, pyloric gland tubular adenoma of the gallbladder tends to exhibit more uniform contrast enhancement than gallbladder cancer or cholesterol polyps [19]. Gallbladder adenomas are prone to cancer development by the adenoma–carcinoma sequence; however, the frequency of adenomas progressing to adenocarcinomas remains unclear [12,14,15,18,20]. Intracystic papillary neoplasm (ICPN) is a gallbladder lesion concept proposed by the 2010 WHO classification ( Figure 32 ), although some aspects of how an ICPN differs from adenoma are unclear, and a unified pathological opinion on the topic is anticipated.
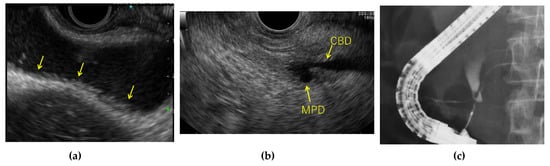
Pancreaticobiliary maljunction (PBM) is a risk factor for biliary tract and gallbladder cancers as it causes mixing of the pancreatic fluid and bile. In particular, gallbladder cancer complicates 40% of PBM cases not associated with dilatation of the extrahepatic biliary tract (undilated PBM). Hyperplastic changes in the gallbladder epithelium are found in 38–63% of PBM cases [21], and biliary tract dilatation is not observed in a high percentage of PMB cases (91–100%) [22]. During the EUS procedure, PBM must always be ruled out when diffuse thickening of the gallbladder wall due to hyperplastic changes is observed by EUS ( Figure 43 ).
4. EUS-FNA of the Gallbladder
Obtaining tissue samples from gallbladder lesions before surgery is difficult, and diagnostic imaging is the main method for differentiating between benign and malignant gallbladder lesions. Although the diagnostic systems for gallbladder lesions are improving owing to advancements in diagnostic imaging technology, differentiating between benign or malignant lesions remains difficult in a significant number of cases, and tissue diagnosis is necessary to rule out other treatable conditions, including not only benign disease but also lymphoma and tuberculosis.
Bile cytodiagnosis using transpapillary endoscopic gallbladder drainage (ENGBD) is reportedly a useful endoscopic method for the cytological diagnosis of gallbladder lesions. However, there are some issues regarding ENGBD cytodiagnosis. This technique poses the risk of perforating the gallbladder duct with the guidewire. In contrast, if a gallbladder lesion can be visualized as a tumor by EUS, a pathological diagnosis can be established using EUS-FNA [28].
Furthermore, in Japan, unlike the diagnosis for pancreatic cancer, preoperative diagnosis by EUS-FNA is not routinely recommended for resectable gallbladder cancer, because there is no evidence of neoadjuvant chemotherapy. Nevertheless, EUS-FNA should be considered in some cases of resectable gallbladder cancer, for example, when it is difficult to categorize a lesion as benign or malignant, or when the surgery is extremely invasive [23]. It can be especially difficult to differentiate XGC from gallbladder cancer, and resection with extensive hepatectomy is sometimes performed for such cases. Preoperative pathological evidence is more important for determining treatment strategies in older patients and those who pose a high risk for surgery. Nevertheless, the absence of malignant cells on EUS-FNA cannot completely rule out coexisting gallbladder cancer, and interpretation of negative EUS-FNA results for malignancy must be performed carefully. XGC coexists in 2–15% of gallbladder cancer cases [43,44]. Cases of coexisting XGC and gallbladder cancer can also involve gallbladder neck cancer with XGC in the body and fundus of the gallbladder due to elevated intra-gallbladder pressure and RAS rupture. For this reason, the gallbladder neck and cystic duct must be examined carefully in addition to the lesion area. EUS allows for the detailed examination of both the gallbladder neck and duct and reduces the risk of overlooked coexisting gallbladder cancer in cases of XGC. Surrounding lymph nodes are also enlarged in 80% of cases of advanced gallbladder cancer [34]. Thus, if enlarged lymph nodes are found when attempting to differentiate between XGC and gallbladder cancer, false positives can be reduced by performing EUS-FNA on the lymph nodes.
EUS-FNA is actively performed in cases of unresectable gallbladder cancer [34]. It is necessary to perform EUS-FNA to help select a treatment strategy in cases of unresectable gallbladder cancer, because small-cell carcinoma of the gallbladder (neuroendocrine type) comprises 2.5% of gallbladder cancer cases [34], and although rare, some reports have described metastatic sarcoma and malignant lymphoma of the gallbladder. Tissue diagnosis is necessary for potentially untreatable gallbladder cancer and to rule out other treatable conditions such as lymphoma, tuberculosis, and XGC [29].