Cripto-1 is an essential protein for human development that plays a key role in the early phase of gastrulation in the differentiation of an embryo as well as assists with wound healing processes. Importantly, Cripto-1 induces epithelial to mesenchymal transition to turn fixed epithelial cells into a more mobile mesenchymal phenotype through the downregulation of epithelial adhesion molecules such as E-cadherin, occludins, and claudins, and the upregulation of mesenchymal, mobile proteins, such as N-cadherin, Snail, and Slug. Consequently, Cripto-1’s role in inducing EMT to promote cell motility is beneficial in embryogenesis, but detrimental in the formation, progression and metastasis of malignant tumors. Indeed, Cripto-1 is found to be upregulated in most cancers, such as breast, lung, gastrointestinal, hepatic, renal, cervical, ovarian, prostate, and skin cancers. Through its role in EMT, Cripto-1 can remodel cancer cells to enable them to travel through the extracellular matrix as well as blood and lymphatic vessels to metastasize to different organs. Additionally, Cripto-1 promotes the survival of cancer stem cells, which can lead to relapse in cancer patients.
1. Cripto-1: Role in Cell Biology
Cripto-1 is a protein encoded by the teratocarcinoma-derived growth factor-1 (TDGF-1) gene
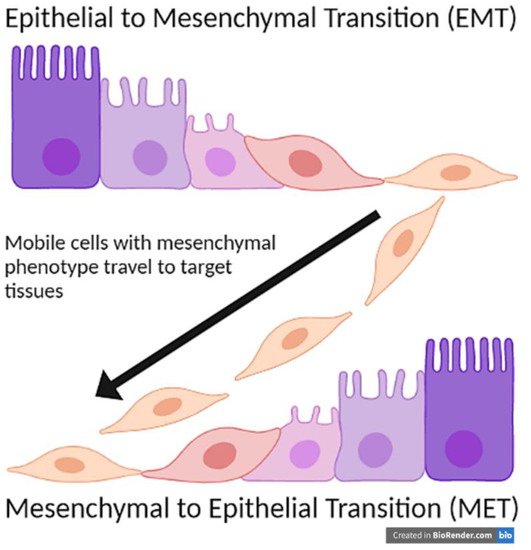
[1]. It is a protein that is found to play a role in embryogenesis, cell migration, and tumor progression through a process called epithelial to mesenchymal transition (EMT) where fixed epithelial cells revert to mobile mesenchymal phenotype and migrate to other areas of the body (
Figure 1). Thus, Cripto-1 is necessary during embryonic development. However, it has a pathological role in promoting tumor progression and metastasis.
Figure 1. Epithelial to Mesenchymal Transition (EMT) and Mesenchymal to Epithelial Transition (MET).
Cripto-1 is also influenced by other signaling molecules, specifically Wnt and β-catenin
[2]. These proteins trigger cardiomyocyte differentiation
[3], as well as mesoderm patterning and cardiac specification
[4]. Mutations in TDGF-1 are associated with the development of ventricular septal defect, the most common congenital heart defect
[1].
Cripto-1 is also the co-receptor for Nodal, a protein in the transforming growth factor-β (TGF-β) family. TGF-β proteins play a role in differentiation and stem cell regulation. Nodal assists with gastrulation, organ positioning, and symmetry
[5]. Both Nodal and Cripto-1 are needed for full functionality
[6]. This article will focus on the role of Cripto-1 in EMT and cancer.
2. Cripto-1: Involvement in Different Types of Cancer
2.1. Breast Cancer
Cripto-1 is overexpressed in a majority of primary human carcinomas including breast cancers. Cripto-1 induces in vitro cell transformation, migration, invasion, epithelial to mesenchymal transition (EMT), and branching morphogenesis in human breast tissues
[7][8][9][10][11][12][13][8,11,44,45,46,47,48]. Moreover, Cripto-1 can be characterized as an oncogene based on studies that demonstrated Cripto-1 transgene’s ability to form mammary hyperplastic lesions and adenocarcinoma of the mammary gland in multiparous transgenic mice that express human Cripto-1 under the murine mammary tumor virus (MMTV) promoter
[10][45]. This transgenic mouse model constantly expresses increased levels of dephosphorylated (active) β-catenin and phosphorylated (inactive) GSK-3β. Importantly, the mammary tumors from the MMTV/Cripto-1 transgenic mice display features of epithelial to mesenchymal transition, including reduced expression of the epithelial marker E-cadherin and increased expression of the mesenchymal markers, Vimentin and N-cadherin, compared to the normal counterpart FVB multiparous mice
[14][7].
Intriguingly, an inverse correlation between the expression of Snail, a known trigger of epithelial to mesenchymal transition, and the prognosis of breast cancers has been documented
[15][49]. Studies revealed that Snail expression correlates directly with the differentiation status and the invasive and metastatic abilities of mouse and human breast cancer cell lines and tissues
[16][50].
Similarly, the developmental transcription factor Msx2 has been shown to induce EMT by up-regulating Cripto-1 expression in the immortalized normal mouse mammary epithelial cells, NMUMG, as evident in the accompanied reduced expression of E-cadherin and increased expression of the mesenchymal phenotype proteins, Vimentin and N-cadherin. Moreover, this mesenchymal phenotype of Msx2-expressing cells can be reversed into a more epithelial-like phenotype by inhibiting Cripto-1 signaling using specific anti-Cripto-1 small-interfering RNA or blocking the c-Src signaling pathway
[7][8]. Altogether, these findings suggest that Msx2 and Cripto-1 collaborate in promoting EMT and contribute to breast tumor progression and invasion processes.
Moreover, Cripto-1 indirectly induces the phosphorylation of Erb-B2 receptor tyrosine kinase 4 (erbB4), which seems to be a necessary step in the Cripto-1-mediated activation of the mitogen-activated protein kinase (MAPK) signaling pathway
[17][51].
Cripto-1 also promotes tumor angiogenesis, an important hallmark of cancer. It has been established that Cripto-1 significantly increases the proliferation and migration of human umbilical vein endothelial cells (HUVECs) and stimulates new blood vessels’ formation in mouse models of breast cancer. Cripto-1 angiogenic effects seem to be independent of those of the vascular endothelial growth factor (VEGF)
[11][46].
Additionally, Cripto-1 promoter is shown to be highly methylated in most breast cancer cell lines studied to date, including T47D and MCF-7 cells. Treatment with histone deacetylase inhibitors (HDAC) and a demethylating agent can reactivate Cripto-1 expression and results in an aggressive phenotype characterized by enhanced migratory and invasive abilities in the human mammary gland adenocarcinoma MCF-7 cell line
[12][47]. While histone deacetylase inhibitors can inadvertently activate other genes responsible for the aggressive phenotype, co-treatment with anti-Cripto-1 small interfering RNA seems to abrogate the HDAC-driven enhanced migratory abilities of MCF7 cells, suggesting a role for Cripto-1 in the migratory and invasive behavior of breast cancers.
Finally, the resistance to anoikis, a form of apoptosis induced when the interaction between epithelial cells and extracellular matrix is disrupted, is enhanced in MCF-7 human breast cancer cells with the overexpression of Cripto-1 due to the activation of Akt
[8][11]. Future studies might shed more light on Cripto-1 involvement in breast cancer progression as the scientific evidence currently remains inconclusive.
2.2. Lung Cancer
In patients with Stage I non-small cell lung cancer (NSCLC), high Cripto-1 expression correlates with metastatic disease and worse prognosis as shown by postoperative survival curves
[18][52]. Although, detection of Cripto-1 using commercially-available antibodies may be subject to reconsideration due to the lack of specificity of some of these antibodies
[19][53]. Importantly, overexpression of Cripto-1 can be detected in about half of the biopsies from lung adenocarcinoma (LAC) patients where it correlates with several clinical and pathological parameters, including tumor size, lymph involvement, advanced TNM clinical stages
[20][54], and loss of E-cadherin expression. Moreover, patients who are intrinsically resistant to epidermal growth factor receptor-tyrosine kinase inhibitors (EGFR-TKI) treatment are more likely to show overexpression of Cripto-1. Patients in clinical stages I, II, and III with high Cripto-1 have a significantly lower 5-year progression-free survival (PFS) rate and median survival time than those with low Cripto-1 expression. When Cripto-1 expression is combined with carcinoembryonic antigen (CEA) levels higher than 5 ng/mL, the cancer is more progressive, and prognosis is typically poor. Altogether, the combination of Cripto-1 expression and CEA levels might be a useful prognostic indicator to predict tumor progression and survival in lung adenocarcinoma patients
[21][10].
2.3. Gastrointestinal Tract Cancers
In a recent study, Cripto-1 and its binding partner, Nodal, were found to be re-expressed in oral squamous cell carcinoma (OSCC) tissue samples. Additionally, their downstream signaling molecules Src, which is associated with the function of Cripto-1, and ERK1/2, which is involved in Nodal signaling, were detected in their phosphorylated active form in the invasive squamous cell carcinoma cell lines SCC15 and SCC25. Additionally, this study attempted to simultaneously block Nodal and Cripto-1 signaling in SCC15 and SCC25 using a blocking antibody, WS65 and a bicyclic peptide, B3, made to prevent Cripto-1 from binding to ALK4 receptor. This blockade of both Nodal and Cripto-1 signaling pathways resulted in significant reduction in the viability of the treated cells, which was accompanied by reduced activation of the signaling molecules, P-Src and P-ERK1/2, associated with Cripto-1 and Nodal, respectively. Moreover, the combined treatment seemed to diminish the aggressiveness of SCC25 cells as measured by a transwell migration and invasion assay
[22][55].
Cripto-1 might also serve as an independent prognostic biomarker in esophageal squamous cell carcinoma (ESCC) since Cripto-1 expression levels positively correlates with the depth of invasion, lymph node involvement, late TNM stages
[20][54], and poor overall survival. Moreover, Cripto-1 could be a marker for ESCC cancer stem-like cells (ECSLC) since ESCC cells with high levels of Cripto-1 possess cancer stem-like (CSL) properties. Indeed, the flow cytometry-sorted Cripto-1
high subpopulations of the EC109 and TE-1 human esophageal squamous cell carcinoma cell lines exhibit higher levels of the stemness-related transcription factors Sox2, Oct4 and Nanog, and display a stronger capacity of sphere and colony formation in vitro as well as higher tumorigenicity and metastatic potential in a xenograft nude mouse model. Additionally, Cripto-1
high cells exhibit EMT-related gene expression pattern including reduced expression of E-cadherin and increased expression of Vimentin, Snail, E47, Foxc2, SIX1, ZEB1, ZEB2 and MMP9. The Cripto-1-induced EMT is associated with enhanced invasive and metastatic abilities of the Cripto-1
high esophageal squamous cell carcinoma cells. Consequently, silencing of Cripto-1 expression by RNA interference reduces the gene expression of factors related to stemness and epithelial to mesenchymal transition
[23][38].
Immunohistochemistry studies have documented an upregulated Cripto-1 expression and downregulated E-cadherin expression in primary gastric carcinoma compared to the counterpart normal gastric mucosa. These studies established a strong correlation between gastric malignancies with Cripto-1 expression with no E-cadherin expression (CR
+/E-cad
−) and several aggressive clinicopathological features, including positive lymph node metastasis, advanced TNM stages
[20][54], and the presence of liver metastases. Thus, a combined Cripto-1 and E-cadherin expression analysis can potentially predict the metastatic behavior and determine the overall prognosis for patients with gastric adenocarcinoma
[24][56].
Patients with colon carcinomas show significantly higher serum Cripto-1 levels than healthy individuals
[25][57]. Immunohistochemical analysis demonstrated that Cripto-1 is abundant in colorectal cancer samples and that its expression is positively correlated with tumor size, depth of invasion, lymph node involvement, liver metastasis, and advanced TNM stages
[20][54]. Moreover, the expression of Cripto-1 correlates with worse overall survival (OS) in all clinical stages and with decreased disease-free survival in patients with stage 0-III colorectal cancer. Cripto-1 is postulated to play a crucial role in the carcinogenesis, progression and metastasis in colorectal cancer since Akt and MAPK signaling pathways are activated by Cripto-1 and the knockdown of Cripto-1 can inhibit proliferation and migration in colorectal cancer cell lines
[26][58].
2.4. Liver Cancer
Patients with hepatocellular carcinoma (HCC) typically have elevated serum Cripto-1 levels, especially those with HBV-related HCC and cirrhosis
[13][48]. A positive correlation between serum Cripto-1 levels and the α-feto-protein (AFP) has been documented in HBV-related HCC patients. Similarly, larger tumors (<5 cm in diameter), lymph node involvement, distant metastases advanced TNM
[20][54] and Barcelona clinic liver cancer (BCLC) stages, as well as tumor recurrences positively correlated with high levels of Cripto-1 in HCC. It was found that overexpression of Cripto-1, high AFP level, high gamma-glutamyl transferase (GGT) level, liver cirrhosis, larger tumors, and vascular invasion lead to poor overall survival (OS) in HCC patients. Similarly, shorter time to recurrence (TTR) significantly correlates with overexpression of Cripto-1, high AFP level, high GGT level, liver cirrhosis, larger tumor size, satellite nodule, and vascular invasion. On the other hand, HCC patients with low Cripto-1 expression have significant OS and TTR advantages. Therefore, Cripto-1 proved to be a reliable predictor for OS and TTR in HCC patients, the 5-year OS and TTR rates in those patients with high Cripto-1 are 37% and 23% compared to OS of 66% and TTR of 62% for patients with low Cripto-1. Similarly, Cripto-1 levels are significantly higher in advanced TNM and BCLC stages. Additionally, patients with overexpression of Cripto-1 are almost three times more likely to relapse. Altogether, this suggests that Cripto-1 can be utilized as an independent prognostic biomarker, or in combination with AFP values, for the different groups of HCC patients. Moreover, there is a close association between capsular infiltration and matrix metallopeptidase 9 (MMP-9) levels in HCC tumors. Interestingly, patients with high MMP-9 levels have high Cripto-1 levels as well
[27][59].
3. Cripto-1 as a Therapeutic Target in Cancer
Given Cripto-1′s role in cancer, especially in cancer stem cells, it is an ideal target for precise therapies, such as blocking monoclonal antibodies, especially since it is detected in higher levels in cancers compared to healthy tissues
[28][68]. In general, anti-Cripto-1 blocking antibodies have shown promising therapeutic effects. For instance, blockade of both Cripto-1 and Nodal signaling is shown to inhibit cell viability and invasiveness in oral squamous cell carcinoma cells
[22][55]. Several anti-Cripto-1 antibodies have been developed, including the antibody-cytotoxic conjugate, BIIB015
[29][69]. Despite the encouraging preclinical data, the phase I-clinical trial (NCT00674947) to evaluate the safety and maximum-tolerated dose (MTD) of BIIB015 ended in 2011 without the publication of its clinical outcome. Other immunotherapeutic agents include a monoclonal antibody that disrupts AKT signaling
[30][70] and a novel humanized Cripto-1 antibody
[31][71]. Moreover, anti-Cripto-1 monoclonal antibodies can target tumor angiogenesis since they are shown to inhibit microvessel formation in vivo
[11][46]. Intriguingly, Cripto-1 has also been utilized as an oncofetal tumor antigen in vaccination immunotherapies resulting in robust cytotoxic T cell-mediated immune responses against cancer stem cells and metastases in melanoma and breast cancer animal models
[32][33][72,73]. Additionally, it has been documented that treatment with antisense oligonucleotides directed against Cripto-1 results in a significant inhibition of the growth of human cancer cells of different histological origins, where Cripto-1 functions as either an autocrine or paracrine growth factor
[8][34][35][36][11,74,75,76]. Altogether, Cripto-1 might serve as a promising target for effective treatments of different types of cancer and to prevent metastatic disease and relapse, especially through specific targeting of small molecules, small interfering RNA, and monoclonal antibodies.