Since multiple reports established an association between diabetes mellitus and various cancers, emerging studies have surfaced to understand the effects of metformin as an anti-cancer agent. Although there was previous, but conflicting evidence, of a relationship between diabetes and ovarian cancer (OvCa), recent studies have supported this association. The mechanism of cancer development in patients with diabetes is likely to involve hyperglycemia, hyperinsulinemia, chronic inflammation, reactive oxygen species, regulation of cellular homeostasis, and activation of various pathways that lead to tumor cell proliferation. Preclinical evidence indicating that metformin, a medication commonly used to treat type 2 diabetes mellitus, may protect against OvCa. Metformin exerts anti-cancer properties by activating the MAPK pathway, inhibiting the PI3K/AKT/mTOR pathway, increasing tumor suppressor genes, inducing G2/M cycle arrest, and various other processes. Several studies have shown the efficacy of metformin as an adjunct with standard chemotherapeutic agents due to its synergistic effects on OvCa cells.
1. Introduction
In the United States, ovarian cancer (OvCa) is currently ranked as the fifth leading cause of death among malignancies, with estimated new cases of 21,410 and estimated deaths of 13,770 in 2021 [
1]. The most common subtype of OvCa is derived from epithelial cells, and these mainly occur in post-menopausal women. In contrast, other types of OvCas, such as germ cells, occur more commonly in premenopausal women; stromal cell tumors can occur at any age [
2]. Among all, high-grade serous ovarian cancer (HGSOC) is dominant and originates from surface epithelium, accounting for 70–80% of OvCa deaths [
3]. Symptoms include abdominal swelling, bloating, pelvic pain, indigestion, altered bowel habits, and getting full easily [
4]. Due to the ambiguity of its symptoms, most OvCas are diagnosed at advanced stages.
Several studies provide links between insulin resistance, hyperglycemia, diabetes mellitus (DM), and cancer [
5,
6]; however, the mechanism by which insulin resistance results in cancer is not fully understood. DM is a metabolic disease that results in hyperglycemia via insulin resistance or lack of insulin production. Various theories of the mechanism of carcinogenesis exist, and are further explored in this article.
Since OvCa and DM share common risk factors, including age, race, obesity, and diet, establishing a direct relationship between DM and OvCa can be difficult. However, several studies have suggested that DM increases the risk of cancer [
5]. A systematic review and meta-analysis of 15 cohorts established a positive correlation between OvCa and DM [
7].
Since an association between DM and OvCa has been established, some studies have explored how metformin, the most common drug used for treating type 2 diabetes (T2DM), is involved in pathways that promote carcinogenicity and induce apoptosis [
8,
9,
10]. A retrospective study of patients with OvCa and concurrent T2DM treated with metformin showed that T2DM patients with OvCa receiving metformin had a longer progression-free survival and overall survival than T2DM patients with OvCa who did not take metformin [
11]. When added to standard first-line chemotherapy, metformin also shows a change in outcome for non-diabetic patients with non-small cell lung cancer [
12]. The present review summarizes evidence showing an association between DM and OvCa, molecular pathways that trigger ovarian carcinogenesis in DM, the effect of metformin as a chemotherapeutic agent, and the synergistic effects of metformin and standard chemotherapeutic regimens in the treatment of OvCa. We have gathered evidence to support the anti-cancer effect of metformin for OvCa. We trust that more research will be accomplished and that clinical trials will be performed to evaluate its efficacy in conjunction with other chemotherapeutic agents.
2. Theories Regarding the Biological Link between DM and OvCa
Most previous epidemiological studies [
39,
40,
41] report no increased risk of OvCa among patients with DM; but some show a borderline significance of associated risk [
42]. For this reason, the relationship between DM and OvCa was unclear until recent systematic reviews and meta-analyses of observational and cohort studies showed a clear association between DM and OvCa [
7,
43,
44]. Although molecular mechanisms for the link between DM and OvCa are yet to be uncovered, there are theories to explain this relationship, including the IGF-I/PI3K/AKT/mTOR pathway used to explain pathogenic connections between DM and other cancers. The KCl co-transport (KCC) protein is essential for developing gynecological cancers; it is involved in the downstream pathways towards cell proliferation and depends on activation of the IGF-1 pathway [
45]. The KCC protein, which exists in three isoforms KCC1, KCC3, and KCC4, regulates cell volume and the influx and efflux ions necessary to maintain the structural integrity [
45]. Because cancer cells usually have a higher growth rate and migration than normal cells, they possess mechanisms to accommodate their volume expansion. Therefore, overexpression of these KCC transporters on cancer cells maintains homeostasis of the cell’s volume. KCC activity is enhanced after activating the IGF-receptor via downstream activation of MAPK/Erk1/2 and PI3K signaling pathways [
46]. Once these pathways are activated, mRNA levels of KCC1, KCC3, and KCC4 increase. When an inhibitor blocks KCC activity, cellular invasion and proliferation are reduced.
In addition to regulating cell volume, KCC activity is also associated with cancer invasion and metastasis by activating matrix metalloproteinases (MMPs) [
47], enzymes involved in collagen degradation in basement membranes [
48]. The KCC4 isoform, isolated from metastatic OvCa cells, interacts with ezrin, a protein involved in epithelial cell migration and adhesion [
49].
3. Antineoplastic Mechanisms of Metformin on OvCa Cells
Recent evidence supports an antineoplastic effect of metformin on cancer cells. There have been several reports on the effectiveness of metformin on OvCa. Although several studies have investigated mechanistic pathways of metformin as an anti-cancer agent, few have revealed targets of the drug in OvCa cells. The molecular mechanisms for the association between DM and the development of OvCa are still being uncovered.
Metformin, a biguanide derivative, is considered a first-line anti-diabetic drug for managing T2DM. It is reported to be associated with a reduced risk of cancer for patients with T2DM [
50]. Although various mechanisms have been considered in understanding its impact on DM and cancer, the most common theory regarding the action of metformin in reducing hyperglycemia and its anti-cancer effects is via activation of the kinase B1 (LKB1)-AMPK pathway in the liver [
51].
AMPK, a heterotrimeric protein kinase that regulates energy metabolism, is activated by oxidative stress, ischemia, hypoxia, and low glucose. Metformin leads to AMPK activation by inhibiting complex 1 of the respiratory chain in the mitochondria, leading to a high AMP/ATP ratio due to a low ATP concentration and elevated conversion of ADP to AMP. Once activated, AMPK leads to various downstream effects, such as activation of tumor suppressor genes P52 and FOXO3a and to inhibition of mTOR, which regulates cell growth and proliferation [
52]. Activation of AMPK also inhibits the PI3K/AKT pathway.
The PI3K/AKT/mTOR pathway, once activated by IGF-I and other growth factors, leads to a series of signaling cascades that promote cell proliferation, growth, invasion, and metastases of various cancers, including OvCa [
53]. This pathway is activated in approximately 70% of OvCa cases [
54]. Metformin inhibits this pathway via interaction with cysteine-rich 61 (Cyr61), a member of the CCN family of growth factors (Cyr61/CTGF/Nov) that is overexpressed in cancers, including OvCas [
55]. In OVCAR-3 OvCa cells, overexpression of Cyr61 enhances cell proliferation by inhibiting carboplatin-induced apoptosis, decreasing expression of the pro-apoptotic marker Bax, and increasing expression of anti-apoptotic markers Bcl-xl, Mcl-1, and Blc-2 [
56]. It also downregulates the tumor suppressor P53 and upregulates NF-KB. Metformin downregulates the protein expression of Cyr61, leading to downregulation of pAKT and mTOR, a process that favors apoptosis [
55].
In a concentration-dependent manner, metformin induces G2/M cell cycle arrest, thus increasing the numbers of cancer cells in the G2 phase [
57]. In addition, it causes DNA damage in OvCa cells, likely due to increased accumulation of intracellular ROS [
57].
Chronic inflammation contributes to pathways that enhance cell proliferation and tumorigenesis. A recent study shows that the OvCa tumor stroma of metformin-treated patients exhibits lower IL6 expression via inhibition of NF-KB [
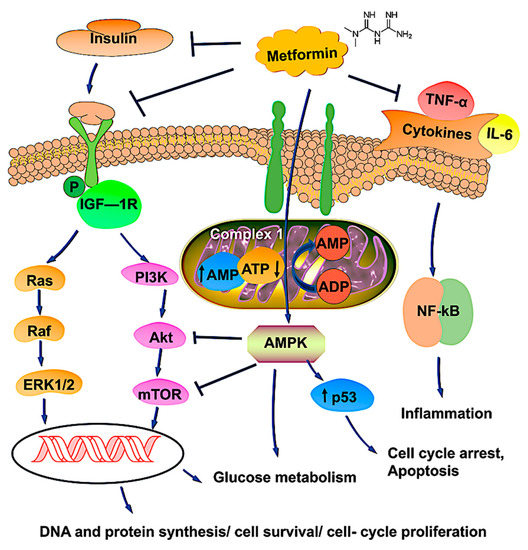
58]. This is a relevant association because IL6 is an inflammatory marker involved in pathogenic pathways in the carcinogenesis of OvCa and inflammation-mediated chemo-resistance. A schematic representation of metformin and its possible mechanisms is shown in
Figure 1.
Figure 1. Schematic representation of metformin’s possible mechanism of action in OvCa therapy. Metformin, a first-line anti-diabetic drug, is likely to be associated with a reduced risk of cancer for those with T2DM. The most common pathway involves the activation of AMPK, which regulates energy metabolism by modulating complex 1 of the respiratory chain in mitochondria by changes in the AMP/ATP ratio. Activated AMPK upregulates the tumor suppressor gene p53, which induces apoptosis and cell cycle arrest. Metformin binds with insulin, IGF, and cytokine receptors and modulates pathways involved in tumor progression. Upon binding, metformin inhibits the PI3K/AKT/mTOR and Ras/Raf/ERK pathways, leading to reductions of DNA synthesis and cell proliferation, thereby causing tumor cell death. Metformin, through AMPK activation and mTOR inhibition, could increase glucose uptake and glycolysis. Overall, metformin promotes phosphorylation, blocking nuclear translocation and impairing gene transcription, processes involved in cell survival, gluconeogenesis, and protein synthesis. The arrows ↑ and ↓ indicates upregulation and downregulation, respectively.
4. The Future of Metformin as an Adjunct for OvCa Therapy
Metformin has been evaluated for its potential synergistic effects with traditional chemotherapeutic agents for the treatment of OvCa. The standard chemotherapy regime involves a combination of a platinum-based agent such as cisplatin or carboplatin and a taxane such as docetaxel or paclitaxel. Metformin enhances the inhibitory effects of cisplatin on epithelial OvCa in vitro and in vivo [
59]. The mechanism proposed here is that metformin inhibits the TGFB-1 pathway, thus decreasing the TGFB-1-induced epithelial-mesenchymal transition, N-cadherin, and MMP, all involved in cancer metastasis. Metformin also has synergistic effects with paclitaxel, as it increases the activity of this chemotherapeutic agent. The combination of metformin and paclitaxel produced a 60% reduction in tumor weight compared to 40% and 42% reductions seen for paclitaxel alone and metformin alone, respectively [
60]. Other studies with OvCa cells have also shown synergistic effects of metformin with chemotherapeutic agents such as dichloroacetate [
60] and trametinib [
61].
A next step to introducing metformin as a nonadjunct therapy to standard chemotherapy agents would be its success in a prospective clinical trial. To the best of our knowledge, only Shahid Faghihi Hospital in Iran has completed a randomized control trial to demonstrate the efficacy of metformin in conjunction with the standard carboplatin-paclitaxel regime after cytoreduction surgery for epithelial OvCa (clinical trials code IRCT2016022726788N1). Patients who underwent total abdominal hysterectomy and bilateral salpingo-oophorectomy diagnosed with epithelial OvCa were considered for this study. A total of 41 patients from each control and intervention group was used to participate. The study results showed a 13.3% 4-year recurrence rate for the study group versus a 67.5% recurrence rate for the control group. The mean survival of patients in the study group was also higher than in the control group [
62]. Although this randomized control study supports the hypothesis that metformin increases the cytotoxic effects of standard chemotherapy agents on OvCa, a limitation is its small sample size (41 patients from each group). According to the NIH
https://clinicaltrials.gov (accessed on 23 July 2021), there are six ongoing clinical trials (
Table 1) to evaluate the effects of metformin in patients receiving chemotherapy for OvCa. These studies, however, are either still recruiting or are in phase 1 or 2; therefore, no results or conclusions have been reported. However, side effects such as gastrointestinal disorders [
63], diarrhea, dyspepsia, and flatulence [
64] are the major limitations reported in the clinical trials.
Table 1. Updates on clinical trials of metformin and OvCa.
| Disease Condition |
Treatment |
Summary |
Trial Phase Status |
Clinical Trial Number |
| Advanced stage OvCa |
Metformin with carboplatin/paclitaxel |
mTOR pathway inhibition, p53-induced apoptosis. |
Phase1 |
NCT02312661 |
| Advanced stage OvCa |
Paclitaxel, carboplatin, and oral metformin |
Increased synergy without compromising patient tolerability. |
Phase 2 |
NCT02437812 |
| Advanced epithelial OvCa in Stages IIIa–-IV |
Metformin,
acetylsalicylic acid,
olaparib, and
letrozole |
Women with advanced (stage IIIa-IV) OvCa of the histologic subtype high-grade serous carcinoma (HGSOC) are going through a diagnostic laparoscopy. They will receive treatment with a study agent for 10–14 days before surgery. The study is randomized and unblinded. |
Early Phase 1 |
NCT03378297 |
Complex endometrial hyperplasia with atypia
grade 1 endometrial endometrioid adenocarcinoma |
Levonorgestrel and metformin |
Metformin is an effective treatment for early-stage endometrial cancer and endometrial hyperplasia with atypia. |
Phase 2 |
NCT01686126 |
| Ovarian, fallopian tube, and primary peritoneal cancer |
Metformin |
To determine if metformin administered in combination with chemotherapy to women with advanced ovarian, primary peritoneal, or fallopian tube cancer will improve recurrence-free survival at 18 months compared to controls. |
Phase 2 |
NCT01579812 |
| Cancer |
Metformin,
atorvastatin,
doxycycline, and
mebendazole |
To determine the effectiveness of a regimen of selected metabolic treatments for patients with cancer in a real-world setting and to conduct exploratory analysis on the relationship between the degree of response and changes in biochemical markers (such as glucose and lipid levels). |
Phase 3 |
NCT02201381 |
Further, metformin has been shown a potential role in immunotherapy, particularly in checkpoint mechanisms, represented by the programmed cell death protein 1 (PD-1)/programmed cell death-ligand 1 (PD-L1) interaction. A study confirms that a patient who received metformin plus anti-PD1 alters immunotherapy resistance by preventing PD-1+/CD8+ T-cell infiltrates [
65]. In a separate survey, metformin enhances the efficacy of PD-1 blockade by reducing the tumor hypoxia in a mouse model [
66]. Since T cells activity in the tumor microenvironment has remained the main goal for US Food and Drug Administration (FDA) approval on the drugs; Liu et al. [
67] displayed several approaches where metformin can enhance T-cell immunity by (1) countering the suppressed state of CD8TILs via AMPK-mTOR signaling, (2) alleviating the intra-tumoral hypoxic state of the tumor microenvironment, and (3) regulating the state of the tumor immune microenvironment (TIME) by downregulating the expression of macrophages, CD39 + CD73 + MSDC, tumor-infiltrating CD4 + CD25 + Treg cells, and upregulation of CD+ T cells, and metabolic reprogramming of Treg cells. A recent report established metformin can holds anti-tumor activity in endometrial cancer by inhibiting the expression of PD-L1 in an AMPK-dependent manner [
68]. Some clinical trial observations indicate metformin with checkpoint inhibitors (nivolumab, pembrolizumab, and durvalumab) is effective in treating tumors [
67]. Indeed, we may overlook various facets where metformin modulates complex immune mechanisms. Therefore, more research is needed to understand the tool before recommending routine therapy in cancer, including OvCa.