Wheat is a valuable source of essential nutrients, providing carbohydrate-based energy and fiber, protein, B vitamins, calcium, magnesium, phosphorus, potassium, zinc, and iron. In low and medium-income countries, grain-based foods still make up the central part of the diet. The wheat seed can be ground into flour or semolina, for example, which form the essential ingredients of bread, pasta, noodles, and other food products, essentially the primary source of nutrients for most of the world population.
- wheat
- nutrients
- celiac disease
- wheat allergy
- non-celiac wheat/gluten sensitivity
1. Introduction
The domestication of wheat revolutionized the human diet as this cereal provided a significant source of energy. Globally, wheat accounts for the largest harvested area of any crop [1] and provides more protein and calories than any other cereal crop [2]. Wheat is nutritious, simple to transport and store, and can be transformed into several types of food. The most valuable modern wheat species are hexaploid bread wheat ( Triticum aestivum L.) and tetraploid durum wheat ( T. turgidum L. var. durum ), which have distinct genomes, grain composition, and end-use quality attributes. Wheat adapts to all climatic conditions common in agricultural fields (except for the hot tropics), so globally, it is harvested all year round [3].
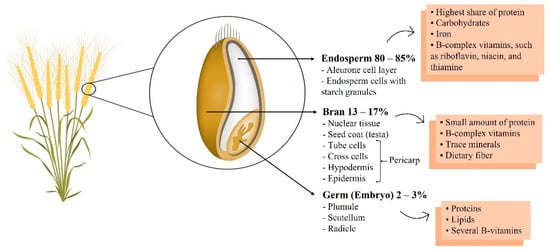
Wheat is a valuable source of essential nutrients, providing carbohydrate-based energy and fiber, protein, B vitamins, calcium, magnesium, phosphorus, potassium, zinc, and iron [4]. In low and medium-income countries, grain-based foods still make up the central part of the diet. The wheat seed can be ground into flour or semolina, for example, which form the essential ingredients of bread, pasta, noodles, and other food products, essentially the primary source of nutrients for most of the world population [5]. Conversely, the lack of grains too often signifies hunger and malnutrition. The characteristic that has given wheat an advantage over other temperate crops is the unique viscoelastic properties of dough formed from wheat flours, which allow it to be processed into such an array of forms [6]. Dough viscoelasticity depends on the structures and interactions that occur between grain storage proteins that form the gluten protein complex [7].
Gluten, which is now an almost ubiquitous ingredient in the food industry, is implicated in several immune-mediated disorders, such as celiac disease (CD). Both CD and other intolerances are of increasing concern [8][9], and the prevalence of CD is predicted to rise [10]. These disorders demand a gluten-free diet (GFD), but a GFD can itself be associated with digestive problems due to insufficient intake of dietary fiber and other nutrients [11].
2. The Health Benefits of Wheat
3. Wheat/Gluten-Related Disorders
Wheat/gluten-related diseases can be classified into three different disorders: autoimmune, allergic, and neither autoimmune nor allergic. Celiac disease is the most prominent autoimmune gluten-related disorder (CD). It is a condition of the small intestine caused by gluten and gluten-related proteins and influenced by environmental and genetic factors [32][33]. An IgE and non-IgE mediated immune response characterize wheat allergy (WA), resulting in an allergic reaction in some individuals upon contact, inhalation, or uptake of foods containing wheat but not necessarily other grains as barley or rye. However, IgE-cross reactivity to other cereals is possible in some people [34][35][36]. Patients with non-celiac wheat/gluten sensitivity (NCWGS) experience identical symptoms to CD, but they do not test positive for CD [37].
The binding of gluten peptides to T cells triggers Celiac Disease (CD) in some individuals expressing human leukocyte antigen (HLA) DQ2 or DQ8 in cells specialized in presenting antigens. Specific CD4+ T cells then recognize the presented peptides releasing inflammatory cytokines, leading to changes in the architecture of intestinal mucosa with atrophy and flattening of villi that can lead to total villous degeneration and enteropathy. Moreover, gliadin peptides are responsible for the activation of innate immunity of the intestinal epithelial cells [38][39].
Gluten ataxia (GA) is a form of cerebellar ataxia, affecting mainly Purkinje cells, and is caused by antibodies released when digesting gluten that mistakenly attacks part of the brain in individuals that are sensitive and genetically susceptible [40]. The clinical symptoms of GA are identical to those of other ataxias. They include gait ataxia (100%), lower limb ataxia (90%), gaze-evoked nystagmus (84%), upper limb ataxia (75%), ocular signs like dysarthria (66%), and other movement disorders including chorea, myoclonus, opsoclonus myoclonus, and palatal tremor [41].
Dermatitis herpetiformis (DH), repeatedly associated with CD, is an autoimmune, chronic, and recurrent cutaneous-intestinal disorder detected in genetically susceptible individuals [11][42][43]. Anti-tTG antibodies that also recognize epidermal transglutaminase (ETG) can be produced after exposure to gluten. ETG is homologous to tTG in terms of structure and is the primary antigen in DH [42]. IgA antibody deposition in dermal papillae causes pruritic, vesiculobullous, and localized lesions in DH patients. DH affects the extensor surfaces such as knees, buttocks, elbows, and scapular areas [42][44][45].
Allergens cause allergic reactions, and wheat is one of the five most frequent foods causing them in children. After milk and eggs, wheat is the most common allergen in Japan, Germany, and Finland [46]. In children and adults, wheat allergy (WA) prevalence is approximately 1% depending on age and region [47][48]. In contrast to CD, distinct wheat components such as water-insoluble proteins (gliadin and glutenin) and water/saline-soluble proteins (albumin and globulin) contribute to the development of WA [11][49][50].
4. Gluten-Related Misconceptions
References
- Food and Agriculture Organization of the United Nations. FAOSTAT Statistics Database Crops. Available online: http://www.fao.org/faostat/en/#data/QC (accessed on 6 October 2020).
- Food and Agriculture Organization of the United Nations. FAOSTAT Statistics Database New Food Balances. Available online: http://www.fao.org/faostat/en/#data/FBS (accessed on 6 October 2020).
- Ribeiro, M.; Nunes, F.M.; Rodriguez-Quijano, M.; Carrillo, J.M.; Branlard, G.; Igrejas, G. Next-generation therapies for celiac disease: The gluten-targeted approaches. Trends Food Sci. Technol. 2018, 75, 56–71.
- Khan, K.; Shrewry, P.R. Wheat: Chemistry and Technology, 4th ed.; AACC International, Inc.: St. Paul, MN, USA, 2009; ISBN 9780128104545.
- Šramková, Z.; Gregová, E.; Šturdík, E. Chemical composition and nutritional quality of wheat grain. Acta Chim. Slovaca 2009, 2, 115–138.
- Peña, R. Wheat for Bread and Other Foods. In Bread Wheat Improvement and Production; Food and Agriculture Organization of the United Nations: Rome, Italy, 2002.
- Shewry, P.R. Wheat. J. Exp. Bot. 2009, 60, 1537–1553.
- Evans, K.E.; Hadjivassiliou, M.; Sanders, D.S. Is it time to screen for adult coeliac disease? Eur. J. Gastroenterol. Hepatol. 2011, 23, 833–838.
- Mustalahti, K.; Catassi, C.; Reunanen, A.; Fabiani, E.; Heier, M.; McMillan, S.; Murray, L.; Metzger, M.H.; Gasparin, M.; Bravi, E.; et al. The prevalence of celiac disease in Europe: Results of a centralized, international mass screening project. Ann. Med. 2010, 42, 587–595.
- Biesiekierski, J.R.; Newnham, E.D.; Irving, P.M.; Barrett, J.S.; Haines, M.; Doecke, J.D.; Shepherd, S.J.; Muir, J.G.; Gibson, P.R. Gluten Causes gastrointestinal symptoms in subjects without celiac disease: A double-blind randomized placebo-controlled trial. Am. J. Gastroenterol. 2011, 106, 508–514.
- Taraghikhah, N.; Ashtari, S.; Asri, N.; Shahbazkhani, B.; Al-Dulaimi, D.; Rostami-Nejad, M.; Rezaei-Tavirani, M.; Razzaghi, M.R.; Zali, M.R. An updated overview of spectrum of gluten-related disorders: Clinical and diagnostic aspects. BMC Gastroenterol. 2020, 20, 258.
- Kumar, P.; Yadava, R.; Gollen, B.; Kumar, S.; Verma, R.; Yadav, S. Nutritional Contents and Medicinal Properties of Wheat: A Review. Life Sci. Med. Res. 2011, 2011, 22.
- Zhang, P.; Ma, G.; Wang, C.; Lu, H.; Li, S.; Xie, Y.; Ma, D.; Zhu, Y.; Guo, T. Effect of irrigation and nitrogen application on grain amino acid composition and protein quality in winter wheat. PLoS ONE 2017, 12, e0178494.
- Poutanen, K. Past and future of cereal grains as food for health. Trends Food Sci. Technol. 2012, 25, 58–62.
- Vogel, K.P.; Johnson, V.A.; Mattern, P.J. Protein and Lysine Contents of Endosperm and Bran of the Parents and Progenies of Crosses of Common Wheat 1. Crop Sci. 1978, 18, 751–754.
- Shewry, P.R.; Hey, S.J. The contribution of wheat to human diet and health. Food Energy Secur. 2015, 4, 178–202.
- Davis, K.; Cain, R.F.; Peters, L.; Tourneau, D.L.; Mcginnis, J. Evaluation of the nutrient composition of wheat. II. Proximate analysis, thiamin, riboflavin, niacin, and pyridoxine. Cereal Chem. 1981, 58, 116–120.
- Osborne, T.B. The Proteins of the Wheat Kernel; Carnegie Inst.: Washington, DC, USA, 1907.
- WHO; FAO. Global trends in production and consumption of carbohydrate foods. In Carbohydrates in Human Nutrition; Food and Agriculture Organization of the United Nations: Rome, Italy, 1998.
- Jones, J.M.; Peña, R.J.; Korczak, R.; Braun, H.J. Carbohydrates, grains, and wheat in nutrition and health: An overview part I. Role of carbohydrates in health. Cereal Foods World 2015, 60, 224–233.
- Raichle, M.E.; Gusnard, D.A. Appraising the brain’s energy budget. Proc. Natl. Acad. Sci. USA 2002, 99, 10237–10239.
- Kahleova, H.; Dort, S.; Holubkov, R.; Barnard, N.D. A plant-based high-carbohydrate, low-fat diet in overweight individuals in a 16-week randomized clinical trial: The role of carbohydrates. Nutrients 2018, 10, 1302.
- WHO; FAO. The role of carbohydrates in maintenance of health. In Carbohydrates in Human Nutrition; Food and Agriculture Organization of the United Nations: Rome, Italy, 1998.
- Uthayakumaran, S.; Wrigley, C. Wheat: Grain-Quality Characteristics and Management of Quality Requirements. In Cereal Grains: Assessing and Managing Quality, 2nd ed.; Elsevier Inc.: Amsterdam, The Netherlands, 2017; pp. 91–134. ISBN 9780081007198.
- Chung, O. Lipid-protein interactions in wheat flour, dough, gluten, and protein fractions. Cereal Foods World 1986, 31, 242–256.
- Neal, A.L.; Geraki, K.; Borg, S.; Quinn, P.; Mosselmans, J.F.; Brinch-Pedersen, H.; Shewry, P.R. Iron and zinc complexation in wild-type and ferritin-expressing wheat grain: Implications for mineral transport into developing grain. J. Biol. Inorg. Chem. 2013, 18, 557–570.
- Batifoulier, F.; Verny, M.A.; Chanliaud, E.; Rémésy, C.; Demigné, C. Variability of B vitamin concentrations in wheat grain, milling fractions and bread products. Eur. J. Agron. 2006, 25, 163–169.
- Piironen, V.; Salmenkallio-Marttila, M. Chapter 7: Micronutrients and Phytochemicals in Wheat Grain. In WHEAT: Chemistry and Technology; AACC International, Inc.: St. Paul, MN, USA, 2009; pp. 179–222.
- Van den Berg, H. Bioavailability of niacin—PubMed. Eur. J. Clin. Nutr. 1997, 51, S64–S65.
- Shewry, P.R.; Van Schaik, F.; Ravel, C.; Charmet, G.; Rakszegi, M.; Bedo, Z.; Ward, J.L. Genotype and environment effects on the contents of vitamins B1, B2, B3, and B6 in wheat grain. J. Agric. Food Chem. 2011, 59, 10564–10571.
- Carter, E.G.A.; Carpenter, K.J. The bioavailability for humans of bound niacin from wheat bran. Am. J. Clin. Nutr. 1982, 36, 855–861.
- Gujral, N.; Freeman, H.J.; Thomson, A.B.R. Celiac disease: Prevalence, diagnosis, pathogenesis and treatment. World J. Gastroenterol. 2012, 18, 6036–6059.
- Cabanillas, B. Gluten-related disorders: Celiac disease, wheat allergy, and nonceliac gluten sensitivity. Crit. Rev. Food Sci. Nutr. 2020, 60, 2606–2621.
- Pourpak, Z.; Mesdaghi, M.; Mansouri, M.; Kazemnejad, A.; Toosi, S.B.; Farhoudi, A. Which cereal is a suitable substitute for wheat in children with wheat allergy? Pediatr. Allergy Immunol. 2005, 16, 262–266.
- Jin, Y.; Acharya, H.G.; Acharya, D.; Jorgensen, R.; Gao, H.; Secord, J.; Ng, P.K.W.; Gangur, V. Advances in molecular mechanisms of wheat allergenicity in animal models: A comprehensive review. Molecules 2019, 24.
- Czaja-Bulsa, G.; Bulsa, M. What do we know now about IgE-mediated wheat allergy in children? Nutrients 2017, 9, 35.
- Pinto-Sanchez, M.I.; Verdu, E.F. Non-celiac gluten or wheat sensitivity: It’s complicated! Neurogastroenterol. Motil. 2018, 30, e13392.
- Maiuri, L.; Ciacci, C.; Ricciardelli, I.; Vacca, L.; Raia, V.; Auricchio, S.; Picard, J.; Osman, M.; Quaratino, S.; Londei, M. Association between innate response to gliadin and activation of pathogenic T cells in coeliac disease. Lancet 2003, 362, 30–37.
- Londei, M.; Ciacci, C.; Ricciardelli, I.; Vacca, L.; Quaratino, S.; Maiuri, L. Gliadin as a stimulator of innate responses in celiac disease. Mol. Immunol. 2005, 42, 913–918.
- Hadjivassiliou, M.; Sanders, D.D.; Aeschlimann, D.P. Gluten-related disorders: Gluten ataxia. Dig. Dis. 2015, 33, 264–268.
- Hadjivassiliou, M.; Grünewald, R.; Sharrack, B.; Sanders, D.; Lobo, A.; Williamson, C.; Woodroofe, N.; Wood, N.; Davies-Jones, A. Gluten ataxia in perspective: Epidemiology, genetic susceptibility and clinical characteristics. Brain 2003, 126, 685–691.
- Clarindo, M.V.; Possebon, A.T.; Soligo, E.M.; Uyeda, H.; Ruaro, R.T.; Empinotti, J.C. Dermatitis herpetiformis: Pathophysiology, clinical presentation, diagnosis and treatment. An. Bras. Dermatol. 2014, 89, 865–877.
- Antiga, E.; Maglie, R.; Quintarelli, L.; Verdelli, A.; Bonciani, D.; Bonciolini, V.; Caproni, M. Dermatitis herpetiformis: Novel perspectives. Front. Immunol. 2019, 10, 1290.
- Hull, C.M.; Liddle, M.; Hansen, N.; Meyer, L.J.; Schmidt, L.; Taylor, T.; Jaskowski, T.D.; Hill, H.R.; Zone, J.J. Elevation of IgA anti-epidermal transglutaminase antibodies in dermatitis herpetiformis. Br. J. Dermatol. 2008, 159, 120–124.
- Mendes, F.B.R.; Hissa-Elian, A.; De Abreu, M.A.M.M.; Gonçalves, V.S. Review: Dermatitis herpetiformis. An. Bras. Dermatol. 2013, 88, 594–599.
- Longo, G.; Berti, I.; Burks, A.W.; Krauss, B.; Barbi, E. IgE-mediated food allergy in children. Lancet 2013, 382, 1656–1664.
- Zuidmeer, L.; Goldhahn, K.; Rona, R.J.; Gislason, D.; Madsen, C.; Summers, C.; Sodergren, E.; Dahlstrom, J.; Lindner, T.; Sigurdardottir, S.T.; et al. The prevalence of plant food allergies: A systematic review. J. Allergy Clin. Immunol. 2008, 121, 1210–1218.
- Nwaru, B.I.; Hickstein, L.; Panesar, S.S.; Roberts, G.; Muraro, A.; Sheikh, A. Prevalence of common food allergies in Europe: A systematic review and meta-analysis. Allergy Eur. J. Allergy Clin. Immunol. 2014, 69, 992–1007.
- Pasha, I.; Saeed, F.; Sultan, M.T.; Batool, R.; Aziz, M.; Ahmed, W. Wheat Allergy and Intolerence; Recent Updates and Perspectives. Crit. Rev. Food Sci. Nutr. 2016, 56, 13–24.
- Marchioni Beery, R.M.; Birk, J.W. Wheat-related disorders reviewed: Making a grain of sense. Expert Rev. Gastroenterol. Hepatol. 2015, 9, 851–864.
- Marcason, W. Is there evidence to support the claim that a gluten-free diet should be used for weight loss? J. Am. Diet. Assoc. 2011, 111, 1786.
- Gaesser, G.A.; Angadi, S.S. Gluten-free diet: Imprudent dietary advice for the general population? J. Acad. Nutr. Diet. 2012, 112, 1330–1333.
- Lebwohl, B.; Cao, Y.; Zong, G.; Hu, F.B.; Green, P.H.R.; Neugut, A.I.; Rimm, E.B.; Sampson, L.; Dougherty, L.W.; Giovannucci, E.; et al. Long term gluten consumption in adults without celiac disease and risk of coronary heart disease: Prospective cohort study. BMJ 2017, 357, j1892.
- Cheng, J.; Brar, P.S.; Lee, A.R.; Green, P.H.R. Body mass index in celiac disease: Beneficial effect of a gluten-free diet. J. Clin. Gastroenterol. 2010, 44, 267–271.
- Dickey, W.; Kearney, N. Overweight in celiac disease: Prevalence, clinical characteristics, and effect of a gluten-free diet. Am. J. Gastroenterol. 2006, 101, 2356–2359.
- Melini, V.; Melini, F. Gluten-free diet: Gaps and needs for a healthier diet. Nutrients 2019, 11, 170.
- Pearlman, M.; Casey, L. Who Should Be Gluten-Free? A Review for the General Practitioner. Med. Clin. N. Am. 2019, 103, 89–99.
- Kasarda, D.D. Can an increase in celiac disease be attributed to an increase in the gluten content of wheat as a consequence of wheat breeding? J. Agric. Food Chem. 2013, 61, 1155–1159.