Breast cancer (BC) is one of the most common causes of female mortality around the globe. It is the second most common cancer and the fifth leading cause of death from cancer in the world. It accounts for around 25% of all female cancers. The worldwide incidence of BC in 2012 was 1.67 million, which is alarming. The incidence may increase to 3.2 million by 2050. Males may also develop BC, but this is very rare, accounting for <1% of diagnosed BCs worldwide. BC may be of different types, based on various factors including etiology, location, and clinical and molecular characteristics. Based on location, BC may be of two types; namely, non-invasive and invasive. Non-invasive BC does not extend away from the lobules or duct where it is located. Invasive BC, on the other hand, reaches out from the lobules and ducts to the nearby mammary tissue.
- breast cancer
- phytonutrients
- chemosensitizer
- polyphenols
- nutrigenomic
- gene expression
- natural compounds
1. Overview
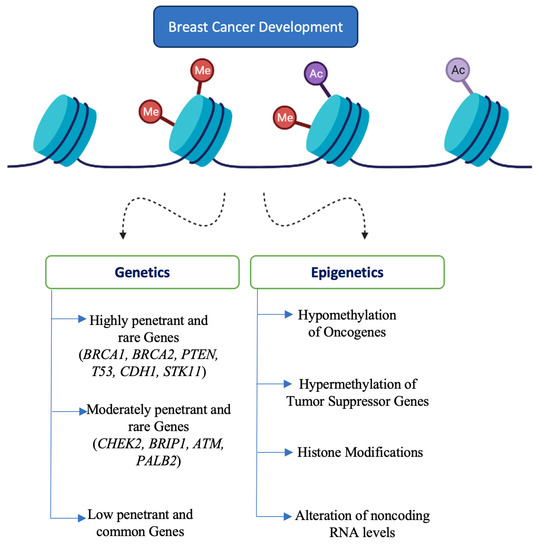
Breast cancer (BC) is one of the most common type of cancer and an important contributor to female mortality. Several genes and epigenetic modifications are involved in the development and progression of BC. Research in phytochemistry, nutrigenomics, and nutrigenetics has provided strong evidence that certain phytonutrients are able to modulate gene expression at transcriptional and post-transcriptional levels. Such phytonutrients may also be beneficial to prevent and treat BC. In this review, we will focus on the nutrigenomic effects of various phytochemicals including polyphenols, phytosterols, terpenoids, alkaloids, and other compounds from different sources. Overall, these phytonutrients are found to inhibit BC cell proliferation, differentiation, invasion, metastasis, angiogenesis, and induce apoptotic cell death by targeting various molecular pathways. They also alter epigenetic mechanisms and enhance the chemosensitivity and radiosensitivity of cancer cells. Such phytochemicals may be used for the effective management of BC patients in the clinical setting in the future. The present article aims to summarize the specific molecular pathways involved in the genetic effects of phytochemicals in BC.
2. Phytochemicals
3. Genetics of Breast Cancer
4. Conclusions
References
- McMillon, E.; McKenna, W.; Milne, C. Guidelines on preparing a medical report for compensation purposes. Br. J. Dermatol. 1982, 106, 489–494.
- Sun, Y.-S.; Zhao, Z.; Yang, Z.-N.; Xu, F.; Lu, H.-J.; Zhu, Z.-Y.; Shi, W.; Jiang, J.; Yao, P.-P.; Zhu, H.-P. Risk factors and preventions of breast cancer. Int. J. Biol. Sci. 2017, 13, 1387–1397.
- Momenimovahed, Z.; Salehiniya, H. Cervical cancer in Iran: Integrative insights of epidemiological analysis. BioMedicine 2018, 8, 18.
- Karthika, C.; Hari, B.; Rahman, H.; Akter, R.; Najda, A.; Albadrani, G.M.; Sayed, A.A.; Akhtar, M.F.; Abdel-Daim, M.M. Multiple strategies with the synergistic approach for addressing colorectal cancer. Biomed. Pharmacother. 2021, 140, 111704.
- Hortobagyi, G.N.; Salazar, J.D.L.G.; Pritchard, K.; Amadori, D.; Haidinger, R.; Hudis, C.A.; Khaled, H.; Liu, M.-C.; Martin, M.; Namer, M.; et al. The global breast cancer burden: Variations in epidemiology and survival. Clin. Breast Cancer 2005, 6, 391–401.
- Yalaza, M.; İnan, A.; Bozer, M.J. Male breast cancer. J. Breast Health 2016, 12, 1.
- Akram, M.; Iqbal, M.; Daniyal, M.; Khan, A.U. Awareness and current knowledge of breast cancer. Biol. Res. 2017, 50, 1–23.
- Manna, S.; Holz, M.K. Tamoxifen action in ER-negative breast cancer. Signal Transduct. Insights 2016, 5, S29901.
- Dembinski, R.; Prasath, V.; Bohnak, C.; Siotos, C.; Sebai, M.E.; Psoter, K.; Gani, F.; Canner, J.; Camp, M.S.; Azizi, A.; et al. Estrogen receptor positive and progesterone receptor negative breast cancer: The role of hormone therapy. Horm. Cancer 2020, 11, 148–154.
- Pernas, S.; Tolaney, S.M. HER2-positive breast cancer: New therapeutic frontiers and overcoming resistance. Ther. Adv. Med. Oncol. 2019, 11, 1758835919833519.
- Drăgănescu, M.; Carmocan, C.J.C. Hormone therapy in breast cancer. Chirurgia 2017, 112, 413–417.
- Mehanna, J.; Haddad, F.G.; Eid, R.; Lambertini, M.; Kourie, H.R. Triple-negative breast cancer: Current perspective on the evolving therapeutic landscape. Int. J. Women Health 2019, 11, 431–437.
- Lester, S.C.; Bose, S.; Chen, Y.-Y.; Connolly, J.L.; de Baca, M.E.; Fitzgibbons, P.L.; Hayes, D.F.; Kleer, C.; O’Malley, F.P.; Page, D.L.; et al. Protocol for the examination of specimens from patients with invasive carcinoma of the breast. Arch. Pathol. Lab. Med. 2009, 133, 1515–1538.
- Bungau, S.G.; Popa, V.-C. Between religion and science some aspects concerning illness and healing in antiquity. Transylv. Rev. 2015, 24, 3–18.
- Bhattacharya, T.; Rather, G.A.; Akter, R.; Kabir, T.; Rauf, A.; Rahman, H. Nutraceuticals and bio-inspired materials from microalgae and their future perspectives. Curr. Top. Med. Chem. 2021, 21, 1.
- Guerriero, G.; Berni, R.; Muñoz-Sánchez, J.A.; Apone, F.; Abdel-Salam, E.M.; Qahtan, A.A.; Alatar, A.A.; Cantini, C.; Cai, G.; Hausman, J.-F.; et al. Production of plant secondary metabolites: Examples, tips and suggestions for biotechnologists. Genes 2018, 9, 309.
- Rui, H.J. Health-promoting components of fruits and vegetables in human health. Nutrients 2013, 4, 384S–392S.
- Behl, T.; Bungau, S.; Kumar, K.; Zengin, G.; Khan, F.; Kumar, A.; Kaur, R.; Venkatachalam, T.; Tit, D.M.; Vesa, C.M.; et al. Pleotropic effects of polyphenols in cardiovascular system. Biomed. Pharmacother. 2020, 130, 110714.
- Behl, T.; Kumar, K.; Brisc, C.; Rus, M.; Nistor-Cseppento, D.C.; Bustea, C.; Aron, R.A.C.; Pantis, C.; Zengin, G.; Sehgal, A.; et al. Exploring the multifocal role of phytochemicals as immunomodulators. Biomed. Pharmacother. 2021, 133, 110959.
- Behl, T.; Sharma, A.; Sharma, L.; Sehgal, A.; Zengin, G.; Brata, R.; Fratila, O.; Bungau, S. Exploring the multifaceted therapeutic potential of withaferin A and its derivatives. Biomedicines 2020, 8, 571.
- Sivasankarapillai, V.S.; Nair, R.M.K.; Rahdar, A.; Bungau, S.; Zaha, D.C.; Aleya, L.; Tit, D.M. Overview of the anticancer activity of withaferin A, an active constituent of the Indian ginseng Withania somnifera. Environ. Sci. Pollut. Res. 2020, 27, 26025–26035.
- Aron, R.C.; Abid, A.; Vesa, C.; Nechifor, A.; Behl, T.; Ghitea, T.; Munteanu, M.; Fratila, O.; Andronie-Cioara, F.; Toma, M.; et al. Recognizing the benefits of pre-/probiotics in metabolic syndrome and type 2 diabetes mellitus considering the influence of Akkermansia muciniphila as a key gut bacterium. Microorganisms 2021, 9, 618.
- Arora, A.; Behl, T.; Sehgal, A.; Singh, S.; Sharma, N.; Bhatia, S.; Sobarzo-Sanchez, E.; Bungau, S. Unravelling the involvement of gut microbiota in type 2 diabetes mellitus. Life Sci. 2021, 273, 119311.
- Abdel-Daim, M.M.; Abushouk, A.I.; Bungau, S.; Bin-Jumah, M.; El-Kott, A.; Shati, A.; Aleya, L.; Alkahtani, S. Protective effects of thymoquinone and diallyl sulphide against malathion-induced toxicity in rats. Environ. Sci. Pollut. Res. 2020, 27, 10228–10235.
- Behl, T.; Kaur, G.; Sehgal, A.; Singh, S.; Bhatia, S.; Al-Harrasi, A.; Zengin, G.; Bungau, S.; Munteanu, M.; Brisc, M.; et al. Elucidating the multi-targeted role of nutraceuticals: A complementary therapy to starve neurodegenerative diseases. Int. J. Mol. Sci. 2021, 22, 4045.
- Makkar, R.; Behl, T.; Bungau, S.; Zengin, G.; Mehta, V.; Kumar, A.; Uddin, S.; Ashraf, G.M.; Abdel-Daim, M.M.; Arora, S.; et al. Nutraceuticals in neurological disorders. Int. J. Mol. Sci. 2020, 21, 4424.
- Tit, D.M.; Bungau, S.; Iovan, C.; Cseppento, D.C.N.; Endres, L.; Sava, C.; Sabau, A.M.; Furau, G.; Furau, C. Effects of the hormone replacement therapy and of soy isoflavones on bone resorption in postmenopause. J. Clin. Med. 2018, 7, 297.
- Țiț, D.M.; Pallag, A.; Iovan, C.V.; Furău, G.; Furău, C.; Bungau, S. Somatic-vegetative symptoms evolution in postmenopausal women treated with phytoestrogens and hormone replacement therapy. Iran. J. Public Health 2017, 46, 1528–1534.
- Bumbu, A.; Bianca, P.; Tit, D.M.; Bungau, S.; Bumbu, G. The effects of soy isoflavones and hormonal replacing therapy on the incidence and evolution of postmenopausal female urinary incontinence. Farmacia 2016, 64, 419–422.
- Bungau, S.; Vesa, C.; Abid, A.; Behl, T.; Tit, D.; Purza, A.; Pasca, B.; Todan, L.; Endres, L. Withaferin A—A promising phytochemical compound with multiple results in dermatological diseases. Molecules 2021, 26, 2407.
- Kapinova, A.; Kubatka, P.; Golubnitschaja, O.; Kello, M.; Zubor, P.; Solar, P.; Pec, M. Dietary phytochemicals in breast cancer research: Anticancer effects and potential utility for effective chemoprevention. Environ. Health Prev. Med. 2018, 23, 36.
- Rahman, M.H.; Akter, R.; Bhattacharya, T.; Abdel-Daim, M.M.; Alkahtani, S.; Arafah, M.W.; Al-Johani, N.S.; Alhoshani, N.M.; Alkeraishan, N.; Alhenaky, A.J. Resveratrol and neuroprotection: Impact and its therapeutic potential in Alzheimer’s disease. Front. Pharmacol. 2020, 11, 2272.
- Shiovitz, S.; Korde, L.A. Genetics of breast cancer: A topic in evolution. Ann. Oncol. 2015, 26, 1291–1299.
- Pasculli, B.; Barbano, R.; Parrella, P. Epigenetics of breast cancer: Biology and clinical implication in the era of precision medicine. Semin. Cancer Biol. 2018, 51, 22–35.
- Karsli-Ceppioglu, S.; Dagdemir, A.; Judes, G.; Ngollo, M.; Penault-Llorca, F.; Pajon, A.; Bignon, Y.-J.; Bernard-Gallon, D. Epigenetic mechanisms of breast cancer: An update of the current knowledge. Epigenomics 2014, 6, 651–664.