LRRK2 is a large (2527 amino acids, 286 kDa), multidomain protein, that bears two enzymatic functions: kinase and GTPase, and several protein-protein interaction domains. Numerous genomic LRRK2 variants have been repeatedly confirmed as pathogenic in Parkinson's Disease (PD). Inhibition of LRRK2 was shown to rescue neurite shortening caused by PD mutations in this protein. This entry discusses possible ways of targetting LRRK2 as potential treatment for PD.
- kinase inhibitors
- neurodegenerative diseases
- Parkinson’s disease
- protein–protein interactions
- small GTPases
- LRRK2
1. Overview
Parkinson’s Disease (PD) affects millions of people worldwide with no cure to halt the progress of the disease. Leucine-rich repeat kinase 2 (LRRK2) is the most common genetic cause of PD and, as such, LRRK2 inhibitors are promising therapeutic agents. In the last decade, great progress in the LRRK2 field has been made. As the majority of developed LRRK2 inhibitors are ATP-competitve and shown some safety concerns, here we present alternative ways of targeting LRRK2 (full text [1]). Currently there are three LRRK2-targeting agents in clinical trials, so more developments are predicted in the upcoming years.
2. Genetic causes of Parkinson's Disease
3. LRRK2 targeting agents in clinical trials
4. Other ways of targeting LRRK2
Since the various PD-mutations have a different effect on the activation mechanism and there are still safety issues raised with the ATP-competitive kinase inhibitors, targeting other domains of LRRK2 than the kinase may prove to be therapeutically effective. Every step in the complex activation mechanism of LRRK2, including, but not limited to, the Roc domain, protein–protein interaction with the N- and C-terminal domains of LRRK2 (e.g., targeting binding of upstream Rab proteins), and/or dimerization, is a potential therapeutic target (Figure 1). The first Roc domain-targeting, GTP-competitive inhibitors have been developed. To identify new targeting surfaces and further develop these sorts of compounds for allosteric targeting of LRRK2 [16], further characterization of the LRRK2 activation mechanism and high-resolution structures will be of great importance. In this respect, the recently identified full-length structure of LRRK2 will be instrumental [17]. In addition to inhibiting LRRK2 activation, approaches that stimulate dephosphorylation of the major LRRK2 substrates, Rabs, could also be considered [18]. Then, finally, there are factors that could regulate the level of the LRRK2 protein itself, either by PROTACs or targeted gene therapy.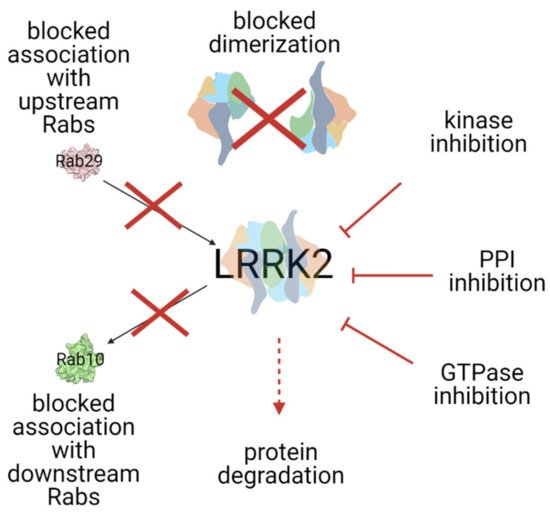
5. Summary and outlook
LRRK2 field has seen great developments over the past decade and went from the lab to the clinic. Numerous kinase-competitive LRRK2 inhibitors have been developed, few of them advancing to clinical trials. A major question that remains to be answered in the upcoming years is whether the LRRK2 specific compounds would also benefit PD patients that do not carry LRRK2 mutations. The next big challenge in the field is the development of reliable biomarkers for accurate detection of LRRK2 activity and monitoring the progression of PD from the early stages. In this respect, antibody or mass spectrometry-based assays that can detect Rab10 phosphorylation in patients’ samples are being studied, as well as urinary proteome profiling, as non-invasive analytical methods [16][17][18].References
- Dominika Wojewska; Arjan Kortholt; LRRK2 Targeting Strategies as Potential Treatment of Parkinson’s Disease. Biomolecules 2021, 11, 1101, 10.3390/biom11081101.
- E. Ray Dorsey; Todd Sherer; Michael S. Okun; Bastiaan R. Bloem; The Emerging Evidence of the Parkinson Pandemic. Journal of Parkinson's Disease 2018, 8, S3-S8, 10.3233/JPD-181474.
- Eldbjørg Hustad; Jan O. Aasly; Clinical and Imaging Markers of Prodromal Parkinson's Disease. Frontiers in Neurology 2020, 11, 395, 10.3389/fneur.2020.00395.
- Sigurlaug Sveinbjornsdottir; The clinical symptoms of Parkinson's disease. Journal of Neurochemistry 2016, 139, 318-324, 10.1111/jnc.13691.
- Roberta Balestrino; Anthony H.V. Schapira; Parkinson disease. European Journal of Neurology 2019, 27, 27-42, 10.1111/ene.14108.
- Ronald B. Postuma; Dag Aarsland; Paolo Barone; David Burn; Christopher H. Hawkes; Wolfgang Oertel; Tjalf Ziemssen; Identifying prodromal Parkinson's disease: Pre-Motor disorders in Parkinson's disease. Movement Disorders 2012, 27, 617-626, 10.1002/mds.24996.
- Dennis W. Dickson; Parkinson's Disease and Parkinsonism: Neuropathology. Cold Spring Harbor Perspectives in Medicine 2012, 2, a009258-a009258, 10.1101/cshperspect.a009258.
- Edoardo Monfrini; Alessio Di Fonzo; Leucine-Rich Repeat Kinase (LRRK2) Genetics and Parkinson’s Disease. Advances in Neurobiology 2017, 14, 3-30, 10.1007/978-3-319-49969-7_1.
- Dunhui Li; Frank L. Mastaglia; Sue Fletcher; Steve D. Wilton; Progress in the molecular pathogenesis and nucleic acid therapeutics for Parkinson's disease in the precision medicine era. Medicinal Research Reviews 2020, 40, 2650-2681, 10.1002/med.21718.
- Udhaya Kumari; E. K. Tan; LRRK2 in Parkinson’s disease: genetic and clinical studies from patients. The FEBS Journal 2009, 276, 6455-6463, 10.1111/j.1742-4658.2009.07344.x.
- Roberto Di Maio; Eric K. Hoffman; Emily Rocha; Matthew T. Keeney; Laurie H. Sanders; Briana R. De Miranda; Alevtina Zharikov; Amber Van Laar; Antonia F. Stepan; Thomas Lanz; et al.Julia K. KoflerEdward A. BurtonDario R. AlessiTeresa G. HastingsJ. Timothy Greenamyre LRRK2 activation in idiopathic Parkinson’s disease. Science Translational Medicine 2018, 10, eaar5429, 10.1126/scitranslmed.aar5429.
- Denali press release 14 January 2020 . Denali Therapeutics. Retrieved 2021-8-6
- Denali press release 6 August 2020 . Denali Therapeutics. Retrieved 2021-8-6
- Denali press release 8 January 2021 . Denali Therapeutics. Retrieved 2021-8-6
- Ahmed Soliman; Fatma Nihan Cankara; Arjan Kortholt; Allosteric inhibition of LRRK2, where are we now. Biochemical Society Transactions 2020, 48, 2185-2194, 10.1042/bst20200424.
- Ying Fan; Francesca Tonelli; Shalini Padmanabhan; Marco A.S. Baptista; Lindsey Riley; Danielle Smith; Connie Marras; Andrew Howden; Dario Alessi; Esther Sammler; et al. Human Peripheral Blood Neutrophil Isolation for Interrogating the Parkinson's Associated LRRK2 Kinase Pathway by Assessing Rab10 Phosphorylation.. Journal of Visualized Experiments 2020, 1, e58956, 10.3791/58956.
- Raja S. Nirujogi; Francesca Tonelli; Matthew Taylor; Pawel Lis; Alexander Zimprich; Esther Sammler; Dario R. Alessi; Development of a multiplexed targeted mass spectrometry assay for LRRK2-phosphorylated Rabs and Ser910/Ser935 biomarker sites. Biochemical Journal 2021, 478, 299-326, 10.1042/bcj20200930.
- Sebastian Virreira Winter; Ozge Karayel; Maximilian Thomas Strauss; Shalini Padmanabhan; Matthew Surface; Kalpana Merchant; Roy N Alcalay; Matthias Mann; Urinary proteome profiling for stratifying patients with familial Parkinson’s disease. EMBO Molecular Medicine 2021, 13, e13257, 10.15252/emmm.202013257.