1. Introduction
The musculoskeletal system is a major body system comprising bones, cartilages, muscles, tendons, ligaments, and other connective tissues. It protects internal organs from external danger, supports locomotion including stability and mobility, and provides other homeostatic functions such as storage of minerals and hematopoiesis
[1]. Unfortunately, musculoskeletal disorders are the leading cause of disability worldwide, and over 1.7 billion people suffer from functional impairment of the system
[2]. Despite its regenerative capacity against small damage, the locomotor system is incapable of fully regenerating its functions for large-volume loss and demands interventional support
[3]. Conventionally, autografts, allografts, and xenografts have been implanted into defective sites; however, there are several drawbacks, including a shortage of donor organs and immune rejection
[4]. Therefore, to overcome these limitations, innovative tissue engineering approaches have been proposed based on an understanding of the complexity of human musculoskeletal tissues.
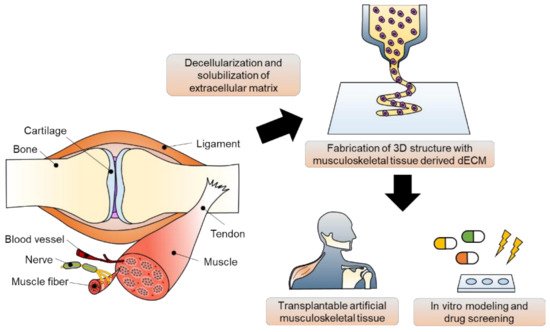
Tissue engineering strategies have been applied for the in vivo regeneration and in vitro modeling of musculoskeletal tissue (
Figure 1). These strategies can be classified as scaffold-based and scaffold-free approaches. The scaffold is defined as a guiding frame-work for cell functions, including adhesion, proliferation, and differentiation
[5]. Using various technologies, such as molding, electrospinning, soft lithography, and micropatterning, scaffolds made of polydimethylsiloxane, poly(2-hydroxyethyl methacrylate), elastin, collagen, and fibrin have been fabricated for musculoskeletal tissue engineering
[6][7][8][9][10][11][6,7,8,9,10,11]. Unlike the classical tissue engineering strategy, scaffold-free tissue equivalents provide a biomimetic microenvironment supporting cellular communication. Based on cell-sheet engineering and pellet/aggregate/spheroid culture platforms, the physiological and functional features of musculoskeletal tissue have been recapitulated in vitro
[12][13][12,13]. Studies on vascularization and innervation in musculoskeletal tissue have also been reported using scaffold-free implants
[14]. By stimulating the innate regenerative capacity of native tissue, tissue-engineered constructs have shown substitutional potential. However, recapitulating the three-dimensional organ structure and complex heterogeneity of the tissue microenvironment using conventional tissue engineering approaches is difficult because of the intrinsic inability to precisely define the spatial distribution of cells
[15].
Figure 1. Musculoskeletal tissue derived decellularized extracellular matrix (dECM) bioink preparation and its applications in 3D bioprinting-based musculoskeletal tissue engineering.
Amongst many tremendous advances, 3D bioprinting technology has been regarded as one of the most promising technologies that can overcome the weaknesses of traditional tissue engineering approaches, leading to technological revolution in the tissue engineering field. By depositing biochemical components to the desired site, the structural and physiological heterogeneity of the organ microenvironment can be recapitulated
[16][17][16,17]. By reproducing the physiological complexities of human tissue, including the diversity of cells, the surrounding structural proteins, and soluble cytokines, in three-dimensional structures, a highly developed approach for tissue regeneration has become possible
[18][19][18,19]. In addition to the regenerative approach, in vitro modeling for physiological and pathological studies of musculoskeletal tissue has also come into greater prominence recently. The 3D-bioprinted in vitro platforms, such as spheroids, organoids, and organ-on-chips containing multiple components, would benefit tissue modeling through drug discovery and the development of precise medicine and patient-specific regenerative therapies
[20][21][20,21].
Bioink, a mixture of biocompatible hydrogels and functional cells, is a key element in 3D bioprinting
[22]. Numerous bioinks, including synthetic polymers and natural hydrogels, have been investigated to replicate the native tissue microenvironment to develop an effective tissue engineering strategy
[23]. Among them, decellularized extracellular matrix (dECM) has been spotlighted as one of the best therapeutic materials available because it inherits tissue- and organ-specific biochemical and physiological characteristics. In addition to basement membrane structural macromolecules, various functional components, such as growth factors and cytokines, can also be provided
[22]. Many studies have shown that dECM bioinks applied to multiple areas, including the brain, heart, liver, pancreas, cornea, and skin, exert synergistic effects on cell survival, growth, migration, and differentiation
[24][25][26][27][28][29][30][24,25,26,27,28,29,30]. Recently, the importance of musculoskeletal tissue engineering has been magnified, which has triggered the active development of musculoskeletal tissue-derived dECM bioinks
[31][32][31,32].
This review aims to introduce the recent advances and accomplishments in musculoskeletal tissue engineering. Together with a description of the features of 3D bioprinting technology and bioprintable materials, effective production strategies for dECM biomaterials and key considerations for grafting them as 3D bioprintable bioinks are explained. The applications of 3D-bioprinted musculoskeletal equivalents using tissue-specific bioinks for both tissue repair and in vitro modeling will be the focus of this review. Lastly, recent advances, limitations, and future perspectives are discussed.
5. Conclusions and Perspectives
Musculoskeletal tissue-derived dECM has shown outstanding potential for tissue engineering applications, resulting in enormous progress. Based on the compositional similarity of the biocompatible material with native tissue, specialized functions along with tissue-specific lineages can be reproduced. Furthermore, the dECM possesses versatility that can be amalgamated with 3D bioprinting technology, which allows spatial patterning to attain structural integrity of the tissue constructs. Therefore, enhanced regenerative capabilities both in vivo and in vitro have been accomplished in many studies.
Despite the biochemical resemblance and complexity of musculoskeletal-tissue–derived dECM bioinks, there are limitations that must be overcome
[152]. Usually, the innate and adaptive immune responses of the donor tissue to dECM are overlooked. To minimize adverse immune reactions against the inevitable disruption of ECM ultrastructure and conformation of secondary analogs, critical analysis and optimization methods of various decellularization protocols are required. In addition to eliminating well-known antigens in dECM, such as dsDNA and GAL epitopes, understanding the interactions between ECM and immune cells, including macrophages and T-cells, is required for material approval for clinical application.
The demands on sophisticated nanostructure hierarchy of each component that make up musculoskeletal tissue have been recognized; the spatial distribution of the molecules of different sizes, shapes, folding, and assembly determine the physiological and mechanical characteristics of the tissue constructs
[153]. For instance, bone displays unique physical performance. The functionality results from the hierarchical structure of hydroxyapatite crystals that exist in various lengths, from nanometers to centimeters scale, comprising up to about 60% of bone. Organizing the fundamental building blocks from the nanoscale to a large scale with precise structural alignment and sustaining the nanostructure of the components is still restricted due to technological limitations
[154]. Therefore, in terms of material engineering, merging the development of nanotechnology and supramolecular chemistry is essential.
The poor mechanical strength of dECM bioinks compared with native tissues is another restriction. The decellularization process to obtain the tissue-specific functional material and the solubilization process to secure printability of a bioink inevitably leads to the loss of various components and destruction of structural stability that affect the specific physical properties such as load-bearing capabilities
[102][155][102,155]. Moreover, the behavior of cells is influenced by the mechanical properties of the incorporated substrates. Not surprisingly, if physical cues, including stiffness, topography, and ligand presentation, are changed, diseases develop. While the processes for preserving biochemical components and solubilizing the dECM are focused on during decellularization, transient elastography and topography have been regarded as unavoidable processes
[156]. To strengthen the weak physical properties of dECM bioinks, multiple approaches such as integrating with polymer scaffolds and incorporating into injectable dECM bioinks other synthetic and cross-linkable molecules such as polyethylene glycol diacrylate (PEGDA), vitamin B2, methacrylate, and Ru/SPS have been tried
[81][85][157][81,85,157]. Furthermore, because the bioink has high mixability and modifiability through covalent bonds, hydrophobic and hydrophilic interactions, and electrostatic forces, cells, drugs, and growth factors can be introduced into dECM bioinks, which is also effective in recapitulating the heterogeneous microenvironment.
The musculoskeletal tissue contains soft-to-hard interface, such as ligament-to-bone, tendon-to-bone, and cartilage-to-bone. Engineering such interface tissues is more complicated than constructing a single specific tissue. It requires a combination of specialized biomaterials with spatially orchestrated compositions, structures, cell types, and biomolecules. Therefore, the conventional monophasic or composite bioinks do not reproduce the biological and physical organization of the interfaces between different tissues
[158]. Hence, advanced biomaterial designs and fabrication strategies are necessary to develop biological constructs with biomimetic gradient features that can encourage the differentiation of multiple cell phenotypes and subsequent interface tissue development.
Finally, the insufficient resolution of 3D printing for reproducing spatiotemporal complexity should also be improved. The resolution depends on the technical specifications of the bioprinter type and physicochemical features of the bioink
[159]. Therefore, optimization of the governing parameters, such as nozzle shape and size, printing head velocity, and bioink viscosity, can improve the resolution. Even pore size, pore interconnection, and proper surface chemistry can be controlled.
In conclusion, the explosive growth of musculoskeletal tissue engineering using 3D bioprinting technology and dECM bioink demands further studies to understand the biochemical and physical features of the musculoskeletal system, optimization of the decellularization protocol, and refinement of 3D bioprinting technology to provide proper in vivo and in vitro platforms. Through this systemic progression, these platforms can be used to identify novel therapeutic medications for disease manifestations. A multidisciplinary optimal design based on cell biology, material science, physics, and mechanical engineering is essential to overcome the recent challenges and accomplish commercialization for clinical applications.