Poor oral hygiene is the primary cause of common oral diseases. and has been found to be associated with low-gradeAccumulation of dental plaque allows bacterial growth that may lead to inflamed periodontal tissues and eventually create bacteremia and systemic inflammation, suggesting its potential link to metabolic syndrome (MetS). Invading bacteria from severe caries or endodontic infections is also thought to provoke similar mechanisms.
- oral hygiene
- dental plaque
- oral bacteria
- tooth brushing
- interdental cleaning
- dental visit
- metabolic syndrome
1. Introduction
Metabolic syndrome (MetS), a clustering of abdominal obesity, hyperglycemia, hypertension, and dyslipidemia, represents a growing public health concern globally [1]. Although the prevalence of MetS differs depending on diagnostic criteria, age group, and ethnicity [1][2], it is estimated to affect around 25% of the world population [2][3]. MetS raises the risk of type 2 diabetes mellitus (T2DM) and cardiovascular diseases [1] and is associated with a 20% increase in healthcare costs [4].
Several risk factors for MetS have been identified. Besides socioeconomic status (SES) [25], smoking [36], diet [47], and physical activity [58], oral diseases, such as periodontal diseases and dental caries, are associated with MetS [69][710][811]. PThe link between oral and systemic diseases is suggested due to coor oral hygiene is tmmon risk factors, subgingival biofilm harboring Gram-negative bacteria, and periodontium serving as a cytokine reservoir [12].
Tooth brushing and interde primary cause of commonntal cleaning, which are the main forms of oral self-care, together with regular professional care, are important measures for plaque control or removal and maintaining optimal oral health [13][14][15]. Poor oral dhygiseases andene care is associated with low-grade inflammation [916], suggesting its potential link to MetS [1017]. The association of poor oral hygiene care with a higher risk of the components of MetS, such as obesity [18], diabetes [19][20], hypertension [20][21], and dyslipidemia [20][22], as well as with cardiovascular disease [23][16], has been demonstrated.
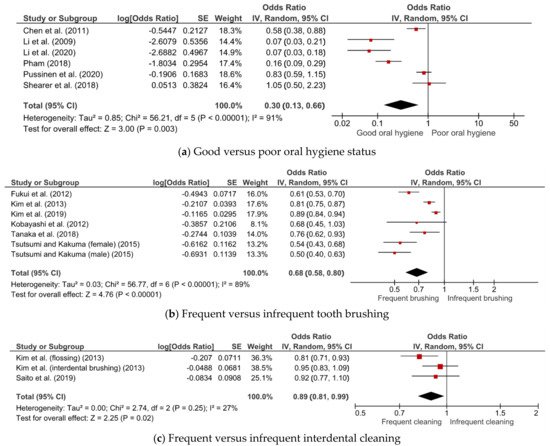
Although several epidemiological studies have reported the association of oral hygiene status [1124] and care [1017][1225] with MetS, some studies found no such association [1326][1427]. To date, there has not been a systematic review conducted on the topic. A summary of evidence can provide a better understanding of the potential relationship and help healthcare practitioners deliver more targeted care. ThisIt systematic review and meta-analysis aimed to evaluate the associations of oral hygiene status and care with MetS.
2. Methods
Briecan provide more substance fly, a systematic seaorch of the PubMed and Web of Science databases from inception to 17 March 2021, and examin the formulation of reference lists was conducted to identify eligible studies. The inclusion criteria include observational studies that examined the association of oral hygiene status (e.g., oral hygiene index, plaque index, plaque score) or care (i.e., tooth brushing, interdental cleaning, and dental visit) with MetS. Two authors independently conducted study selection, data extraction, and quality assessment of the studies. Any ambiguities or disagreements were resolved by consensus. Meta-analysis was conducted separately for different types of exposure (i.e., oral hygiene status, tooth brushing, and interdental cleaning). A random-effects model was applied to pool the effects of oral hygiene status and care on public health programs and policies, especially strategies for the prevention and management of MetS. Potential sources of heterogeneity were assessed using prespecified subgroup analyses by study design and country.
32. ResultAssociation between Oral Hygiene Status, Care, and MetS
Subgroup analysis
3. Subgroup Analyses
4
| Subgroup | Number of Studies | OR (95% CI) | I2 (%) | p |
|---|---|---|---|---|
| Subgroup | Number of Studies | OR (95% CI) | I2 (%) | p | |||||
|---|---|---|---|---|---|---|---|---|---|
| Cross-sectional | 2 | ||||||||
| Study design | 0.72 (0.41–1.26) | 46 | 0.17 | ||||||
| Case–control | 3 | 0.11 (0.06–0.20) | 39 | 0.19 | |||||
| Cross-sectional | 5 | 0.67 (0.55–0.81) | 93 | <0.001 | Cohort | 1 | 0.83 (0.59–1.15) | - | - |
| Cohort | 2 | 0.74 (0.62–0.89) | 0 | 0.64 | |||||
| Country | |||||||||
| Japan | 5 | 0.61 (0.52–0.70) | 55 | 0.06 | |||||
| Korea | 2 | 0.85 (0.78–0.93) | 73 | 0.06 |
3. Conclusion
References
- Cornier, M.A.; Dabelea, D.; Hernandez, T.L.; Lindstrom, R.C.; Steig, A.J.; Stob, N.R.; Van Pelt, R.E.; Wang, H.; Eckel, R.H; The Metabolic Syndrome. Endocrine Reviews 2008, 29, 777-822, 10.1210/er.2008-0024.Cornier, M.A.; Dabelea, D.; Hernandez, T.L.; Lindstrom, R.C.; Steig, A.J.; Stob, N.R.; Van Pelt, R.E.; Wang, H.; Eckel, R.H. The metabolic syndrome. Endocr. Rev. 2008, 29, 777–822.
- Blanquet, M.; Legrand, A.; Pélissier, A.; Mourgues, C.; Socio-economics status and metabolic syndrome: A meta-analysis. Diabetes & Metabolic Syndrome: Clinical Research & Reviews 2019, 13, 1805-1812, 10.1016/j.dsx.2019.04.003.Lear, S.A.; Gasevic, D. Ethnicity and metabolic syndrome: Implications for assessment, management and prevention. Nutrients 2020, 12, 15.
- Sun, K.; Liu, J.; Ning, G.; Active Smoking and Risk of Metabolic Syndrome: A Meta-Analysis of Prospective Studies. PLOS ONE 2012, 7, e47791, 10.1371/journal.pone.0047791.Saklayen, M.G. The Global Epidemic of the Metabolic Syndrome. Curr. Hypertens. Rep. 2018, 20, 1–8.
- Fabiani, R.; Naldini, G.; Chiavarini, M.; Dietary Patterns and Metabolic Syndrome in Adult Subjects: A Systematic Review and Meta-Analysis.. Nutrients 2019, 11, 2056, 10.3390/nu11092056.Curtis, L.H.; Hammill, B.G.; Bethel, M.A.; Anstrom, K.J.; Gottdiener, J.S.; Schulman, K.A. Costs of the metabolic syndrome in elderly individuals: Findings from the Cardiovascular Health Study. Diabetes Care 2007, 30, 2553–2558.
- Joseph, M.S.; Tincopa, M.A.; Walden, P.; Jackson, E.; Conte, M.L.; Rubenfire, M.; The Impact Of Structured Exercise Programs On Metabolic Syndrome And Its Components: A Systematic Review. Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy 2019, ume 12, 2395-2404, 10.2147/DMSO.S211776.Blanquet, M.; Legrand, A.; Pélissier, A.; Mourgues, C. Socio-economics status and metabolic syndrome: A meta-analysis. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 1805–1812.
- Gobin, R.; Tian, D.; Liu, Q.; Wang, J.; Periodontal Diseases and the Risk of Metabolic Syndrome: An Updated Systematic Review and Meta-Analysis. Frontiers in Endocrinology 2020, 11, 336, 10.3389/fendo.2020.00336.Sun, K.; Liu, J.; Ning, G. Active Smoking and Risk of Metabolic Syndrome: A Meta-Analysis of Prospective Studies. PLoS ONE 2012, 7, e47791.
- Cao, X.; Wang, D.; Zhou, J.; Yuan, H.; Chen, Z.; Relationship between dental caries and metabolic syndrome among 13 998 middle-aged urban Chinese. Journal of Diabetes 2016, 9, 378-385, 10.1111/1753-0407.12424.Fabiani, R.; Naldini, G.; Chiavarini, M. Dietary patterns and metabolic syndrome in adult subjects: A systematic review and meta-analysis. Nutrients 2019, 11, 2056.
- Ojima, M.; Amano, A.; Kurata, S.; Relationship Between Decayed Teeth and Metabolic Syndrome: Data From 4716 Middle-Aged Male Japanese Employees. Journal of Epidemiology 2015, 25, 204-211, 10.2188/jea.je20140132.Joseph, M.S.; Tincopa, M.A.; Walden, P.; Jackson, E.; Conte, M.L.; Rubenfire, M. The impact of structured exercise programs on metabolic syndrome and its components: A systematic review. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 2395–2404.
- De Oliveira, C.; Watt, R.; Hamer, M.; Toothbrushing, inflammation, and risk of cardiovascular disease: results from Scottish Health Survey. BMJ 2010, 340, c2451-c2451, 10.1136/bmj.c2451.Gobin, R.; Tian, D.; Liu, Q.; Wang, J. Periodontal Diseases and the Risk of Metabolic Syndrome: An Updated Systematic Review and Meta-Analysis. Front. Endocrinol. 2020, 11, 1035–1057.
- Tanaka, A.; Takeuchi, K.; Furuta, M.; Takeshita, T.; Suma, S.; Shinagawa, T.; Shimazaki, Y.; Yamashita, Y.; Relationship of toothbrushing to metabolic syndrome in middle-aged adults.. Journal of Clinical Periodontology 2018, 45, 538-547, 10.1111/jcpe.12876.Cao, X.; Wang, D.; Zhou, J.; Yuan, H.; Chen, Z. Relationship between dental caries and metabolic syndrome among 13 998 middle-aged urban Chinese. J. Diabetes 2017, 9, 378–385.
- Pham, T.; The association between periodontal disease severity and metabolic syndrome in Vietnamese patients. International Journal of Dental Hygiene 2018, 16, 484-491, 10.1111/idh.12350.Ojima, M.; Amano, A.; Kurata, S. Relationship between decayed teeth and metabolic syndrome: Data from 4716 middle-aged male Japanese employees. J. Epidemiol. 2015, 25, 204–211.
- Kobayashi, Y.; Niu, K.; Guan, L.; Momma, H.; Guo, H.; Cui, Y.; Nagatomi, R.; Oral Health Behavior and Metabolic Syndrome and Its Components in Adults. Journal of Dental Research 2012, 91, 479-484, 10.1177/0022034512440707.Li, X.; Kolltveit, K.M.; Tronstad, L.; Olsen, I. Systemic diseases caused by oral infection. Clin. Microbiol. Rev. 2000, 13, 547–558.
- Shearer, D.M.; Thomson, W.M.; Cameron, C.M.; Ramrakha, S.; Wilson, G.; Wong, T.Y.; Williams, M.J.A.; McLean, R.; Theodore, R.; Poulton, R.; et al. Periodontitis and multiple markers of cardiometabolic risk in the fourth decade: A cohort study. Community Dentistry and Oral Epidemiology 2018, 46, 615-623, 10.1111/cdoe.12414.Claydon, N.C. Current concepts in toothbrushing and interdental cleaning. Periodontol. 2000 2008, 48, 10–22.
- Pussinen, P.J.; Paju, S.; Viikari, J.; Salminen, A.; Taittonen, L.; Laitinen, T.; Burgner, D.; Kahonen, M.; Lehtimaki, T.; Hutri-Kahonen, N.; et al. Childhood Oral Infections Associate with Adulthood Metabolic Syndrome: A Longitudinal Cohort Study. Journal of Dental Research 2020, 99, 1165-1173, 10.1177/0022034520929271.Ainamo, J. Prevention of periodontal disease in the dental office. Int. Dent. J. 1984, 34, 56–61.
- Lim, L.P.; Davies, W.I.R. Comparison of various modalities of “simple” periodontal therapy on oral cleanliness and bleeding. J. Clin. Periodontol. 1996, 23, 595–600.
- De Oliveira, C.; Watt, R.; Hamer, M. Toothbrushing, inflammation, and risk of cardiovascular disease: Results from Scottish Health Survey. BMJ 2010, 340, 1400.
- Tanaka, A.; Takeuchi, K.; Furuta, M.; Takeshita, T.; Suma, S.; Shinagawa, T.; Shimazaki, Y.; Yamashita, Y. Relationship of toothbrushing to metabolic syndrome in middle-aged adults. J. Clin. Periodontol. 2018, 45, 538–547.
- Nijakowski, K.; Lehmann, A.; Rutkowski, R.; Korybalska, K.; Witowski, J.; Surdacka, A. Poor oral hygiene and high levels of inflammatory cytokines in saliva predict the risk of overweight and obesity. Int. J. Environ. Res. Public Health 2020, 17, 6310.
- Chang, Y.; Lee, J.S.; Lee, K.J.; Woo, H.G.; Song, T.J. Improved oral hygiene is associated with decreased risk of new-onset diabetes: A nationwide population-based cohort study. Diabetologia 2020, 63, 924–933.
- Fujita, M.; Ueno, K.; Hata, A. Lower frequency of daily teeth brushing is related to high prevalence of cardiovascular risk factors. Exp. Biol. Med. 2009, 234, 387–394.
- Choi, H.M.; Han, K.; Park, Y.-G.; Park, J.-B. Associations Among Oral Hygiene Behavior and Hypertension Prevalence and Control: The 2008 to 2010 Korea National Health and Nutrition Examination Survey. J. Periodontol. 2015, 86, 866–873.
- Song, T.J.; Kim, J.W.; Kim, J. Oral health and changes in lipid profile: A nationwide cohort study. J. Clin. Periodontol. 2020, 47, 1437–1445.
- Chang, Y.; Woo, H.G.; Park, J.; Lee, J.S.; Song, T.J. Improved oral hygiene care is associated with decreased risk of occurrence for atrial fibrillation and heart failure: A nationwide population-based cohort study. Eur. J. Prev. Cardiol. 2020, 27, 1835–1845.
- Pham, T. The association between periodontal disease severity and metabolic syndrome in Vietnamese patients. Int. J. Dent. Hyg. 2018, 16, 484–491.
- Kobayashi, Y.; Niu, K.; Guan, L.; Momma, H.; Guo, H.; Cui, Y.; Nagatomi, R. Oral health behavior and metabolic syndrome and its components in adults. J. Dent. Res. 2012, 91, 479–484.
- Pussinen, P.J.; Paju, S.; Viikari, J.; Salminen, A.; Taittonen, L.; Laitinen, T.; Burgner, D.; Kahonen, M.; Lehtimaki, T.; Hutri-Kahonen, N.; et al. Childhood Oral Infections Associate with Adulthood Metabolic Syndrome: A Longitudinal Cohort Study. J. Dent. Res. 2020, 99, 1165–1173.
- Shearer, D.M.; Thomson, W.M.; Cameron, C.M.; Ramrakha, S.; Wilson, G.; Wong, T.Y.; Williams, M.J.A.; McLean, R.; Theodore, R.; Poulton, R. Periodontitis and multiple markers of cardiometabolic risk in the fourth decade: A cohort study. Community Dent. Oral Epidemiol. 2018, 46, 615–623.
- Baeza, M.; Morales, A.; Cisterna, C.; Cavalla, F.; Jara, G.; Isamitt, Y.; Pino, P.; Gamonal, J. Effect of periodontal treatment in patients with periodontitis and diabetes: Systematic review and meta-analysis. J. Appl. Oral Sci. 2020, 28.
- Santarelli, A.; Wong, D.T.W.; Lo Muzio, L. Editorial: Saliva and Oral Microbiota: From Physiology to Diagnostic and Therapeutic Implications. Front. Physiol. 2021, 11, 637599.
- Souza, M.L.; Massignan, C.; Peres, K.G.; Peres, M.A. Association between metabolic syndrome and tooth loss: A systematic review and meta-analysis. J. Am. Dent. Assoc. 2019, 150, 1027–1039.e7.