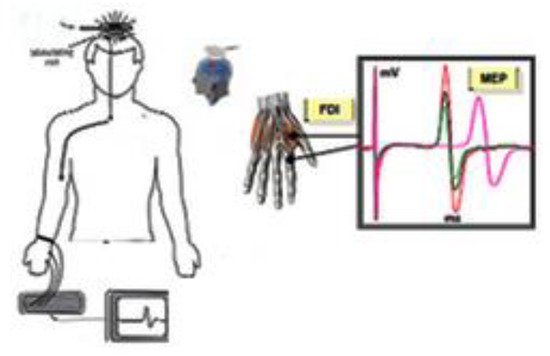
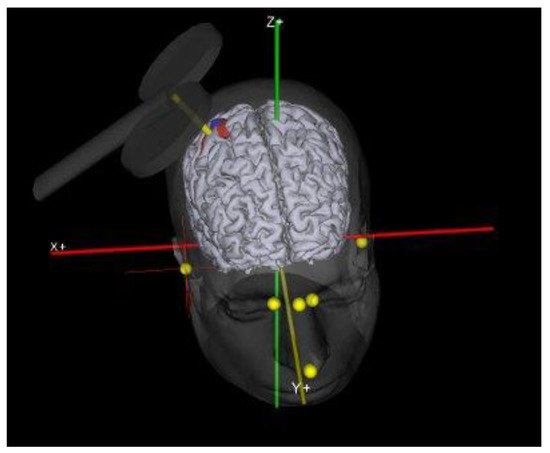
The TMS is a noninvasive method to investigate the CNS in the human. Transcranial magnetic stimulation, since its introduction in 1985, has brought important innovations to the study of cortical excitability as it is a non-invasive method and, therefore, can be used both in healthy and sick subjects. Since the introduction of this cortical stimulation technique, it has been possible to deepen the neurophysiological aspects of motor activation and control. Repetitive physical training is generally considered as a principal strategy for acquiring a motor skill, and this process can elicit cortical motor representational changes referred to as use-dependent plasticity. In training settings, physical practice combined with the observation of target movements can enhance cortical excitability and facilitate the process of learning. The data to date suggest that TMS is a valid technique to investigate the changes in motor cortex excitability in trained and untrained subjects.
- corticalexcitability
- transcranial magnetic stimulation
- motor cortex
- TMS
1. Transcranial Magnetic Stimulation (TMS)
2. Cortical Excitability and Physical Exercise
2.1. Skill Training
2.2. Fatigue
2.3. Aerobic and Anaerobic Exercise
3. The Use of TMS in Sport Science
| Authors | Type of Sport | Type of Exercise | Main Findings |
|---|---|---|---|
| Jensen et al., 2005 [28] | Original research | Strength training | The results of this investigation show that increased corticospinal excitability may develop over several weeks of skill training and indicate that these changes may be of importance for task acquisition. |
| Moscatelli et al., 2016 [41] | Original research | Karate | Karate athletes show higher corticospinal excitability compared to non athletes indicating the presence of an activity-dependent alteration in the balance and interactions between inhibitory and facilitatory circuits determining the final output from the M1 |
| Moscatelli et al., 2016 [42] | Original research | Karate | The practice of competitive sports affects central/peripheral nervous system. Subjects that showed higher cortical excitability showed also higher velocity at which the neural signal is propagated from the motor cortex to the muscle and consequently better reaction time. |
| Moscatelli et al., 2016 [44] | Original research | Taekwondo | The results of this study show that blood lactate seems to have the greater effect in taekwondo athletes compared to untrained subjects. During extremely intensive exercise in taekwondo athletes, lactate may delay the onset of fatigue not only by maintaining the excitability of muscle, but also by increasing the excitability of the primary motor cortex more than in non-athletes. |
| Tergau et al., 2000 [47] | Original research | Lifting | Double-pulse TMS gives access to the motor cortex independently of spinal or peripheral mechanisms, reduced Intra Cortical Facilitation reflects decreased excitability of interneuronal circuits within the motor cortex. |
| Coco et al., 2014 [52] | Original research | Intensive isometric exercises | The relation between blood lactate and the amplitudes of motor-evoked potentials showed a significant direct proportionality. |
| Höllgeet al., 1997 [58] | Original research | Aerobic and anaerobic exercise | This investigation show the possible use of TMS in sports medicine, indicating that only exhaustive or strength exercises result in reduced MEPs. |
| Ljubisavljević et al., 1996 [59] | Original research | submaximal isometric voluntary contraction | The increase in MEP magnitude after the sustained 60% maximal voluntary contraction may indicate residual changes in cortical activity after fatiguing contraction. |
| MaKay et al., 1996 [60] | Original research | Isometric maximal contraction | These results of this investigation suggest that MEP and SP might have common sources of facilitation during maximal voluntary contraction and that inhibitory mechanisms remain focally augmented following a fatiguing maximal voluntary contraction. |
| Fulton et al., 2002 [64] | Original research | Rowers | There were no differences in MEP depression or latency between elite rowers and non-rowers after intense exercise. The authors conclude that the smaller degree of MEP depression in the elite rowers after light exercise reflects less central fatigue within corticospinal control pathways than that seen in the non-rowers. |
| Coco et al., 2010 [70] | Original research | Cycling | In this study was observed that an increase of blood lactate is associated with a decrease of motor threshold, that is, an enhancement of motor cortex excitability. The authors conclude by hypothesizing that in the motor cortex the lactate could have a protective role against fatigue. |
| Moscatelli et al., 2020 [78] | Original resea | Aerobic exercise | This study shows that aerobic activity seems to induce changes in cortical excitability if performed for a period longer than 4 weeks, in addition to typical cardiorespiratory benefits in previously untrained males |
| Percivalle et al., 2010 [68] | Original research | Maximal exhausting exercise | The authors observed a similar enhancement of excitability of primary motor cortex, concomitantly with an increase of blood lactate, in both young male and female athletes. However, the improvement was significantly higher in women than in men, suggesting a greater sensitiveness of female cerebral cortex to blood lactate. |
| Cros et al., 2007 [75] | Original research | Isometric contraction | The timing of central conduction was different depending on functional role of the target muscle, as either agonist or joint fixator. These results indicate that the architecture of motor plans remain grossly undisrupted by cortical stimulation applied during voluntary motor behavior. |
| Brasil-Neto et al., 1994 [76] | Original research | Isometric and isotonic exercise | The results are similar to those found at the neuromuscular junction in myasthenia gravis and are consistent with a reduced safety factor of cortical synaptic transmission in central nervous system fatigue. |
| Verin et al., 1985 [77] | Original research | Incremental treadmill exercise | The results of this study confirm significant depression of both diaphragm and quadriceps MEPs after incremental treadmill exercise. |