Classroom active desks refer to the desks placed in the classroom and can be moved in teaching activities. This entry was to examine the effects of active desks in the school setting on sedentary behavior, physical activity, academic achievements and overall health among children and adolescents aged 5–17 years.
- academic achievements
- active desks
1. Introduction
Concerns and research regarding the effects of sedentary behaviors and physical inactivity on overall health have been growing for the last decades, leading nowadays to a better identification of their independent and joint implications [1][2]. While sedentary behaviors is defined as any waking behavior characterized by an energy expenditure ≤1.5 metabolic equivalents, while in a sitting, reclining or lying posture [3][4], physical inactivity is typically defined as “the non-achievement of physical activity guidelines” [5]. Both sedentary behaviors and physical inactivity have substantially increased in our societies, with physical inactivity being identified as the main cause for about 1.6 million deaths worldwide [6] and leading to a public health cost of $53.8 billion per year [7]. Due to their important implication in the risks of all-cause mortality and cardio-metabolic morbidity as well as in some cancer occurrence [8], both sedentary behaviors [9][10] and physical inactivity [11][12] are of public health concern today.
In children and adolescents, it has been found with device-based measurements that daily sitting time takes over 50% of the waking day at 7 years and 75% at 15 years [13]. This high level of sedentariness, combined with the fact that about 80% of children and adolescents are inactive (i.e., not reaching the physical activity recommendations) [14][15], led some scientists to propose the existence of what they called a “Sedentary & Inactive” profile [16]. Not only physical inactivity and sedentary behaviors have been found to be associated with early metabolic and cardiovascular risk in children and adolescents [17][18][19][20][21], they have also been found to be related to a decrease in cognitive performance and academic achievements [22][23][24].
Knowledge and behaviors developed during childhood have been shown to influence their future behaviors as adults [25]. In particular, children’s physical activity and sedentary behaviors have been shown to not only determine their actual health but also their adolescent and adult behaviors and health [26]. Since children spend at least one third of their waking time in class [27], school appears as an ideal setting to promote health and induce behavioral change [28]. Targeting school time and the school place to promote healthy active behaviors necessitates however to face the highly sedentary nature of the children’s class time. In that context, the literature shows a growing number of experiments trying to implement interventions aimed at breaking and reducing this sedentary time during class [29][30]. The use of active desks in the classroom (e.g., standing desks, sit-to-stand desks, cycling desks, stability balls) has been especially studied [31][32][33][34], with studies showing for instance that sit-to-stand desks seem to reduce sedentary time in the classroom [31] or increase energy expenditure with the use of bike desks [34]. These studies are providing some promising results and our aim is to conduct a systematic analysis of these works to have a better understanding of their effects.
Table 1. Active desks characteristics and range of price.
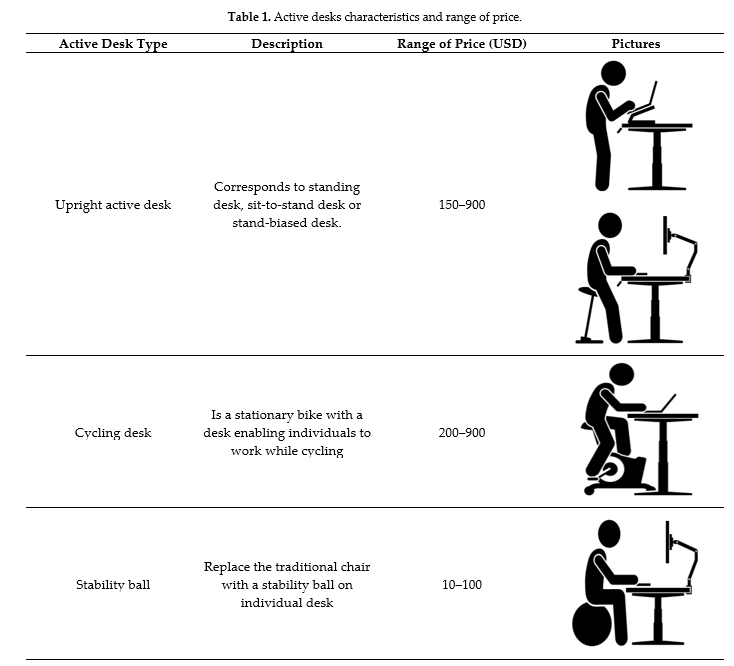
| Active Desk Type | Description | Range of Price (USD) | Pictures |
|---|---|---|---|
| Upright active desk | Corresponds to standing desk, sit-to-stand desk or stand-biased desk. | 150–900 |   |
| Cycling desk | Is a stationary bike with a desk enabling individuals to work while cycling | 200–900 |  |
| Stability ball | Replace the traditional chair with a stability ball on individual desk | 10–100 |  |
2. Search Strategy
A literature search was conducted for studies from year 1990 to October 2020 using the following electronic bibliographic databases: PubMed, ScienceDirect, ResearchGate, Google Scholar and Medline (Cochrane Library). The search terms included the key words “desk* or workstation* or work station” AND “treadmill OR pedaling OR cycling OR bicycl* OR bik* OR active OR exercise ball* OR swiss ball* OR stability ball* OR dynamic seating OR active sitting OR standing OR stepping OR stand up OR position, standing OR standing position* OR sit-to-stand OR sit stand OR stand/sit OR stand biased OR adjustable furniture OR height adjustable” AND “school* OR class* OR child* OR student* OR academic institution”. To identify articles potentially missed during the literature search, reference lists of candidate articles were reviewed.
3.Description of Studies
The PRISMA flow diagram presented in Figure 1 summarizes the study selection process. The search strategy initially found a total of 1677 references after removing duplicates. A total of 1635 articles were excluded after screening of titles and abstracts. Full text copies were obtained for 44 articles; of which 25 articles matched the inclusion criteria and were thus included in this systematic review. The main reasons for studies exclusion among the remaining were: (1) study design did not meet inclusion criteria (n = 8); (2) intervention did not use an active desk (n = 5); (3) population was not children without health issues (n = 3); (4) full texts were not available (n = 2); and (5) active desks were already integrated in classroom (n = 1). One article included two different study designs [31].
Ten studies were randomized controlled trials (RCT) [30][31][33][34][35][36][37][38][39][40] with four pilot studies [30][31][36][37]; seven were non-randomized controlled trials [31][41][42][43][44][45][46] with four pilot studies [31][44][45][46]; four were non-randomized trials [47][48][49][50] with two pilot studies [48][49]; one was a randomized trial [51] and four were crossover studies [32][52][53][54].
Among the included studies, 19 were conducted among primary school children aged 6–12 years [31][32][33][35][47][36][41][37][42][43][48][52][44][53][54][39][46][50][40], five took place among secondary level adolescents aged 12–17 years [30][34][53][39][50] and Verloigne et al. [38] enrolled children in both levels aged 10–16 years.
Two studies included boys only [32][52], three did not specify the gender [30][36][49] and the rest of the studies included both boys and girls [31][33][34][47][36][37][42][43][48][49][51][44][53][45][54][38][39][46][50][40].
Twenty studies assessed upright active desks (i.e., standing desk, sit-to-stand desk and stand-biased desk) [31][32][35][47][36][41][37][42][43][48][49][52][51][44][53][45][54][38][39][46]; three cycle desks [30][34][46] and two used stability balls [33][40]. Active desks have been described in Table 1.
In twenty-one studies, active desks were allocated to every individual [31][32][33][34][35][47][36][41][43][48][49][52][51][44][53][45][54][39][46][50][40]. Verloigne et al. [38] implemented three standing desks per classroom, Clemes et al. [37] provided six active desks in each class and Fedewa et al. [30] provided four active desks in interventional group. One study did not specify the number of implemented active desks [42].
All studies had an intervention duration from two weeks to two years. Verloigne et al. [38] suggested a rotation every half class while Clemes et al. [31] recommended to use active desks at least 30 min per day (Australian study) and one hour per day (English study). Some studies suggested also to practice active desks at least one hour per day [37][46] or for four class hours of 50 min per week [34]. Several studies did not indicate the active desks time and frequency use [48][52][44][50][55]. Some interventions enabled active desks to be free to use [30][35][47][36][41][43][48][49][53][45] or to use it for the entire school day [32][33][42][40]. In one study, active desks were only used for the evaluations [50].
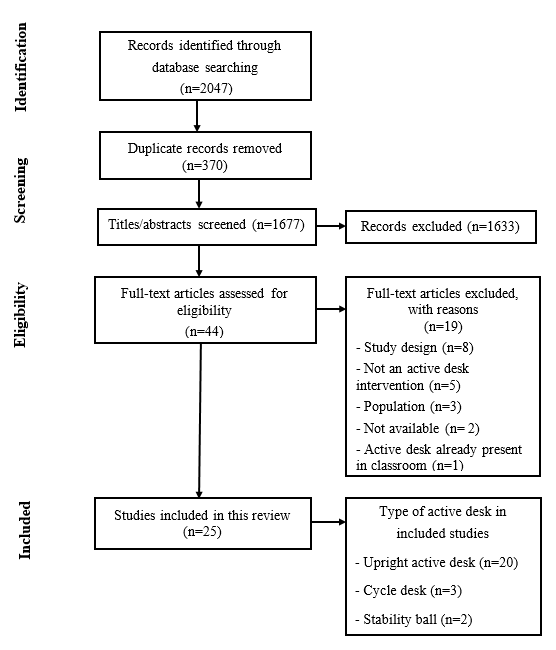
Figure 1. PRISMA flow chart
4. Data Synthesis by Outcome
4.1. Body Composition
Six studies assessed body composition when using upright active desks [35][47][36][37][48][39] and one with cycling desks [34]. However, one study did not detail their results on this outcome [35] (Table 6). Wendel et al. [39] found a significant difference in BMI for interventional group compared to the control group after two years of intervention (−5.24 for BMI percentile) (Table 3). Other studies did not report any change in BMI with the use of an upright active desk.
Torbeyns et al. [34] observed a significant effect of time for height, body weight, fat mass percentage and waist circumference without condition effect. However, traditional desks group reported a significantly higher BMI while cycling desks group did not find any difference.
4.2. Sedentary Behaviors
Thirteen articles using upright active desks assessed sedentary behaviors [31][32][41][37][43][52][51][44][53][45][54][38][46], while only one used cycling desks [30]. As presented in Table 3, two studies observed that children, when using upright active desks, spent significantly less time sedentary than the control group, using objective measurements [43][54]. Other studies did not find any difference for the interventional group [52][45]. Moreover, Ee et al. [32] observed no significant difference for whole day sedentary time but reported a significant reduction in sitting time during school hours for the intervention group compared to the control group. Similar results have been reported in four other articles [31][37][53][45]. Additionally, four studies reported a reduction of sitting time between T0 and T1 for the intervention group [37][43][44][50]. Similar results have been found in another study but were not statistically significant [52][53].
4.3. Physical Activity
Sixteen articles assessed physical activity using upright active desks [31][32][47][36][41][37][43][48][52][51][44][53][45][54][38][46], two with cycling desks [30][34] and one with stability balls [33]. Studies assessing the upright active desk effects on physical activity reported several different outcomes such as light physical activity, moderate-to-vigorous physical activity (MVPA), step counts, stepping, standing and walking time (Table 3).
For light physical activity, four studies reported no significant changes for interventional group compared to the control group [32][51][53][40][55]. For MVPA, studies found contradictory results while two studies did not find any change [32][52]. Kidokoro et al. [43] observed a significant increase in MVPA for the intervention group between pre- and post-intervention. Another study [54] found that MVPA decreased for the intervention group during school years but less than the control group. Additionally, they reported that the benefit of upright active desk was greater among students initially determined as less active.
Statistically significant increases were reported for the intervention group standing time in height studies [31][32][41][37][51][44][45][38][46]. Similar results have been reported but without reaching significance [52][53].
Regarding step counts, Benden et al. [47] reported an increase of this outcome without statistical analyses (Table 3 and Table 6). In another study, they reported similar results at mid intervention but not at the end [36]. No significant effects were observed in two other studies [48][51]. In the article of Clemes et al. [31], the study in Australian school reported no significant effect while the British ones showed an increase for the intervention group in post intervention.
For stepping time a significant decrease was reported for the intervention group [38] or no effect [31][46]. One study [44] observed a significant increase while Clemes et al. [37] found similar results but no statistical analyses have been reported.
Torbeyns et al. [34] assessed the effect of cycling desks on physical activity with a questionnaire. Interventional group and control group decreased their physical activity time between pre- and post-intervention but no condition effect was observed. Despite the lack of statistical analyses (Table 2 and Table 4), one study reported, with an objective measurement, an increase of light physical activity and MVPA for the intervention group compared to the control group [30].
One study using stability balls assessed physical activity and missed to observe any difference between the interventional group and the control group after the intervention [33]. Additionally, all groups decreased their physical activity level and their step count between pre- and post-intervention.
4.4. Energy Expenditure
Four studies assessed energy expenditure with the use of upright active desks [36][41][49][54] and two with cycling desks [30][34]. All upright active desks studies observed an increase between 15% and 25.7% in energy expenditure for interventional groups compared to control groups [36][41][49][54] (Table 2).
Cycling desk studies reported also an increase of energy expenditure. Torbeyns et al. [34] showed a significant increase in energy expenditure (36%) using cycling desks compared to traditional desks. Fedewa et al. [30] reported similar results without any statistical analyses (Table 3 and Table 6).
4.5. Physical Capacities and Cardiometabolic Health
Physical capacities were only evaluated in one study that used cycling desks [34]. The authors reported an increase in the performance during the 20 m shuttle run test in their interventional group compared to the control group (+0.6 interval) (Table 3). Moreover, there was a significantly lower rate of perceived exertion (RPE) in the interventional group compared to the control group after 22 weeks. For cardiometabolic health, only Clemes et al. [37] assessed blood pressure with the use of an upright active desks. They reported an increase in systolic blood pressure in the interventional group but the authors did not perform statistical analyses (Table 2 and Table 4).
4.6. Cognitive and Academic Performance
Seven studies assessed cognitive and academic performance when using upright active desks [37][49][52][44][45][38][39], two studies with cycling desks [34][50] and two with stability balls [33][40]. Concerning executive functions (working memory, inhibitor control, cognitive flexibility), visual working memory was assessed in two studies using upright active desk and two studies using cycling desks and no change was reported [34][45][39][46]. As detailed in Table 4, inhibitory control has been assessed in three studies, and the use of cycling desks shown to significantly increase the inhibitor control in the intervention group compared to the control group with an higher increase of accuracy for the intervention group (4.21%) [50]. One of the studies that used upright active desk reported an improvement in both reaction time and accuracy [46] while the other reported no significant change [49]. The reaction time for cognitive flexibility decreased after intervention in the study that used upright active desks [46]
Regarding to academic engagement and attention, two studies using upright active desks reported an increase in the intervention group compared to the control group [41][42] without any change in concentration and classroom management [33][37][38]. A study using stability balls reported more interaction time with teachers but the time working with other students or independently were reduced compared to the control group after intervention. Both groups observed improvement in mathematics and literacy but they were not related specifically to the intervention [40]. Mehta et al. [49] assessed several outcomes where they primarily observed a significant increase in cognitive performance with the use of upright active desks compared to traditional ones.
4.7. Fatigue and Musculoskeletal Pain Symptoms
Six studies, all with upright active desks, assessed fatigue and musculoskeletal pain symptoms [32][37][44][53][38][40]. Three studies reported no difference on those outcomes between upright active desks and traditional desks [37][44][38]. Significant changes have been reported in two studies [32][52] with a decrease of pain symptoms in the neck and shoulder area. Nonetheless, a study observed that 51% of children have experienced pain in legs and back area with the use of upright active desks [45] (Table 4).
4.8. Process Evaluation
Acceptability and feasibility have been assessed in several studies [30][41][37][43][44][45][38]; one was cycling desks [30] and others were upright active desks. One study reported retention rates of 100% for schools and 97% for children with an overall recruitment rate at 33% [37] (Table 4). Studies have shown a good acceptability of upright active desks in children [49][51][44], with a willingness to use it in the future and a reduction of sleepiness [43]. From teachers’ perspective, they have declared a positive influence of upright active desks to complete tasks and are willing to continue teaching with upright active desks [45]. One study reported that parents have felt a positive impact on their children’s behavior at school [41]. However, one study [38] reported some negative effects with the use of upright active desks such as a slight deterioration of the relation with classmates. Authors also reported, a decrease of the mean duration and habit to use upright active desks over time. Most of those observations were reported in primary schools; secondary schools observed an improvement of the attitude towards the desk [38].
For cycling desks, authors [30] observed no change in attention and task completion compared to traditional desks. Students also experimented a reduction of fidgeting. Their preference to sit on cycling desks compared to traditional desks was higher despite the lack of a comfortable seat. Overall, cycling desks have been perceived by teachers and students as a positive tool to improve the environment of school class.
It was determined by the review team that a meta-analysis was not possible due to high levels of heterogeneity across studies; narrative syntheses were employed instead. The overall quality of the included studies was low due to methodological inconsistencies, in addition of the heterogeneity in terms of statistical and clinical characteristics (Table 52 and Table 63).
5. Conclusions
Table 2. Study risks of bias.
| dies | Random Sequence Generation | Allocation Concealment | Performance Bias | Detection Bias | Attrition Bias | Reporting Bias | Other Bias |
|---|---|---|---|---|---|---|---|
| Upright active desk | |||||||
| Benden et al. (2011) [40] | Low risk | Unclear | High risk | High risk | Low risk | Low risk | Unclear |
| Benden et al. (2012) [41] | High risk | High risk | High risk | High risk | High risk | Low risk | Unclear |
| Benden et al. (2014) [42] | Low risk | Unclear | High risk | High risk | Low risk | Low risk | Low risk |
| Blake et al. (2012) [43] | High risk | High risk | High risk | High risk | High risk | High risk | Unclear |
| Clemes et al. (2016) (Bradford, England) [31] | High risk | Unclear | High risk | High risk | Low risk | Low risk | Unclear |
| Clemes et al. (2016) (Melbourne, Australia) [31] | Unclear | Unclear | High risk | High risk | Low risk | Low risk | Unclear |
| Clemes et al. (2020) [44] | Low risk | Low risk | High risk | High risk | Low risk | Low risk | Low risk |
| Dornhecker et al. (2015) [45] | Low risk | Unclear | High risk | High risk | Low risk | Low risk | Unclear |
| Ee et al. (2018) [32] | N/A | N/A | High risk | High risk | Low risk | Low risk | Low risk |
| Kidokoro et al. (2019) [46] | High risk | High risk | High risk | High risk | Low risk | Low risk | Low risk |
| Koepp et al. (2012) [47] | High risk | High risk | High risk | High risk | Low risk | Low risk | Unclear |
| Mehta et al. (2015) [48] | High risk | High risk | High risk | High risk | Low risk | Low risk | Low risk |
| Parry et al. (2019) [49] | N/A | N/A | High risk | High risk | Low risk | Low risk | Unclear |
| Pickens et al. (2016) [50] | High risk | Unclear | High risk | High risk | Low risk | Low risk | Unclear |
| Sherry et al. (2020) [51] | High risk | High risk | High risk | High risk | Low risk | Low risk | Low risk |
| Sprengeler et al. (2020) [52] | N/A | N/A | High risk | High risk | Low risk | Low risk | Low risk |
| Sudholz et al. (2016) [53] | High risk | High risk | High risk | High risk | Low risk | Low risk | Low risk |
| Swartz et al. (2019) [54] | N/A | N/A | High risk | High risk | Low risk | Low risk | Low risk |
| Verloigne et al. (2018) [55] | Low risk | Unclear | High risk | High risk | High risk | Low risk | Low risk |
| Wendel et al. (2016) [56] | Low risk | Low risk | High risk | High risk | Low risk | Low risk | Low risk |
| Wick et al. (2018) [57] | High risk | Unclear | High risk | High risk | Low risk | Low risk | Low risk |
| Cycling desk | |||||||
| Fedewa et al. (2017) [30] | Low risk | Unclear | High risk | High risk | Low risk | Low risk | Unclear |
| Ruiter et al. (2019) [58] | Low risk | Low risk | High risk | High risk | Low risk | Low risk | Unclear |
| Torbeyns et al. (2017) [34] | Low risk | Unclear | High risk | High risk | Low risk | Low risk | Low risk |
| Stability ball | |||||||
| Erwin et al. (2016) [33] | Low risk | Unclear | High risk | High risk | Low risk | Low risk | Unclear |
| Fedewa et al. (2015) [59] | Low risk | High risk | High risk | High risk | Low risk | Low risk | Unclear |
Table 3. Association between the use of active desks and outcomes of included studies for the systematic review.
| Outcome Assessment | No of Studies | Design | Quality Assessment | Quality | ||||
|---|---|---|---|---|---|---|---|---|
| Risk of Bias | Inconsistency | Indirectness | Imprecision | Other | ||||
| Body composition | School grade ranged between 1 and 10. Body composition was assessed objectively as body mass index, body mass, body fat percentage (bio-impedance), waist circumference. | |||||||
| 5 | RCT a | No serious risk of bias | No serious inconsistency | No serious indirectness | Serious imprecision b | None | MODERATE | |
| 2 | NRT c | Serious risk of bias d | Serious inconsistency e | No serious indirectness | No serious imprecision | None | VERY LOW | |
| Physical activity | School grade ranged between 1 and 12. Physical activity was assessed as light physical activity, MVPA, step counts, standing, stepping and walking time: by devices (accelerometers, inclinometers), self-reported questionnaires and/or external observations. | |||||||
| 7 | RCT f | No serious risk of bias | Serious inconsistency g | No serious indirectness | Serious imprecision h | None | LOW | |
| 6 | NRCT i | Serious risk of bias j | No serious inconsistency | No serious indirectness | Serious imprecision k | None | VERY LOW | |
| 2 | NRT l | Serious risk of bias m | No serious inconsistency | No serious indirectness | Serious imprecision n | None | VERY LOW | |
| 1 | RT o | No serious risk of bias | No serious inconsistency | No serious indirectness | No serious imprecision | None | LOW | |
| 4 | Cross-over p | No serious risk of bias | No serious inconsistency | No serious indirectness | No serious imprecision | None | LOW | |
| Sedentary behaviors | School grade ranged between 1 and 10. Sedentary behaviors were assessed by observations and/or self reporting questionnaires. | |||||||
| 3 | RCT q | No serious risk of bias | No serious inconsistency | No serious indirectness | Serious risk of imprecision r | None | MODERATE | |
| 6 | NRCT s | Serious risk of bias t | No serious inconsistency | No serious indirectness | Serious risk of imprecision u | None | VERY LOW | |
| 1 | RT v | No serious risk of bias | No serious inconsistency | No serious indirectness | No serious imprecision | None | LOW | |
| 4 | Cross-over w | No serious risk of bias | No serious inconsistency | No serious indirectness | No serious imprecision | None | LOW | |
| Energy expenditure | School grade ranged between 1 and 10. Energy expenditure was assessed by a portable device (armband) during school days and/or entire days. | |||||||
| 4 | RCT x | No serious risk of bias | No serious inconsistency | No serious indirectness | Serious risk of imprecision y | None | MODERATE | |
| 1 | NRCT z | Serious risk of bias aa | No serious inconsistency | No serious indirectness | Serious risk of imprecision ab | None | VERY LOW | |
| 1 | NRT ac | Serious risk of bias ad | No serious inconsistency | No serious indirectness | Serious risk of imprecision ae | None | VERY LOW | |
| Cognitive and academic performance | School grade ranged between 2 and 10. Cognitive performance was assessed by cognitive functions test (working memory, inhibitory control, flexibility, attention) and on-task behaviors (observations, interviews) | |||||||
| 4 | RCT af | Serious risk of bias ag | No serious inconsistency | No serious indirectness | No serious imprecision | None | MODERATE | |
| 4 | NRCT ah | Serious risk of bias ai | No serious inconsistency | No serious indirectness | No serious imprecision | None | VERY LOW | |
| 3 | NRT aj | Serious risk of bias ak | No serious inconsistency | No serious indirectness | No serious imprecision | None | VERY LOW | |
| Fatigue and musculoskeletal symptoms | School grade ranged between 4 and 10. Fatigue and musculoskeletal symptoms were assessed by questionnaires (Nordic Musculoskeletal Questionnaire, paper questionnaires), teacher observations, focus groups and/or interviews. | |||||||
| 1 | RCT al | No serious risk of bias | No serious inconsistency | No serious indirectness | Serious imprecision am | None | MODERATE | |
| 2 | NRCT an | Serious risk of bias ao | No serious inconsistency | No serious indirectness | Serious imprecision ap | None | VERY LOW | |
| 1 | NRT aq | Serious risk of bias ar | No serious inconsistency | No serious indirectness | No serious imprecision | None | VERY LOW | |
| 2 | Cross-over as | No serious risk of bias | No serious inconsistency | No serious indirectness | No serious imprecision | None | LOW | |
| Process evaluation | Mean age ranged between 6 and 17 year. Perceptions and experiences of participants was assessed by questionnaires, self-reporting answers and/or interviews. | |||||||
| 3 | RCT at | Serious risk of bias au | Serious inconsistency av | No serious indirectness | No serious imprecision | None | LOW | |
| 4 | NRCT aw | Serious risk of bias ax | No serious inconsistency | No serious indirectness | No serious imprecision | None | VERY LOW | |
| Physical capacities and cardiometabolic health | School grade ranged between 4 and 10. Physical capacities was assessed by the 20 m shuttle run test. Cardiometabolic health was assessed by blood pressure. |
|||||||
| 2 | RCT ay | No serious risk of bias | No serious inconsistency | No serious indirectness | Serious imprecision az | None | MODERATE | |
RCT: Randomized Controlled Trial; RT: Randomized Trial; NRCT: Non-Randomized Controlled Trial; NRT: Non-Randomized Trial. a Includes five randomized controlled studies [34][40][42][44][56]. b One study did not detail the age and sex of participants. Additionally, the results of body composition assessment were incomplete (the quality of evidence was downgraded from “high” to “moderate”). c Includes two non-randomized studies [41][47]. d Studies reported mixed findings (the quality of evidence was downgraded from “low” to “very low”). e Inconsistencies have been reported in the unit used in the results (the quality of evidence was downgraded from “low” to “very low”). f Includes seven randomized controlled studies [30][31][33][34][42][44][55]. g Inconsistencies have been reported in the number of participants (the quality of evidence was downgraded from “high to “moderate”). h Several studies did not achieve statistical analyses (the quality of evidence was downgraded from “moderate” to “low”). i Includes six non-randomized controlled studies [31][43][46][51][53][57]. j Studies reported mixed findings (the quality of evidence was downgraded from “low” to “very low”). k One study did not achieve statistical analyses (the quality of evidence was already at “very low”). l Includes two non-randomized studies [41][47]. m Studies reported mixed findings (the quality of evidence was downgraded from “low” to “very low”). n One study did not achieve statistical analyses (the quality of evidence was already at “very low”). o Includes one randomized study [50]. p Includes four cross-over studies [32][49][52][54]. q Includes three randomized controlled studies [31][44][55]. r One study did not achieve statistical analyses (the quality of evidence was downgraded from “high” to “moderate”). s Includes six non-randomized controlled studies [31][43][46][51][53][57]. t Studies reported mixed findings (the quality of evidence was downgraded from “low” to “very low”). u One study did not achieve statistical analyses (the quality of evidence was already at “very low”). v Includes one randomized study [50]. w Includes four cross-over studies [32][49][52][54]. x Includes four randomized controlled studies [30][34][40][42]. y One study did not achieve statistical analyses (the quality of evidence was downgraded from “high” to “moderate”). z Includes one non-randomized non-controlled study [43]. aa Studies reported mixed findings (the quality of evidence was downgraded from “low” to “very low”). ab One study did not achieve statistical analyses (the quality of evidence was already at “very low”). ac Includes one non-randomized study [41]. ad Studies reported mixed findings (the quality of evidence was downgraded from “low” to “very low”). ae One study did not achieve statistical analyses (the quality of evidence was already at “very low”). af Includes four randomized controlled studies [33][34][44][59]. ag One study did not achieve statistical analyses (the quality of evidence was downgraded from “high” to “moderate”). ah Includes four non-randomized controlled studies [43][45][51][57]. ai Studies reported mixed findings (the quality of evidence was downgraded from “low” to “very low”). aj Includes 3 non-randomized studies [47][48][58]. ak Studies reported mixed findings (the quality of evidence was downgraded from “low” to “very low”). al Includes one randomized controlled study [44]. am One study did not detail the number of participants for this outcome and did not achieve statistical analyses (the quality of evidence was downgraded from “high” to “moderate”). an Includes two non-randomized non-controlled study [51][53]. ao Studies reported mixed findings (the quality of evidence was downgraded from “low” to “very low”). ap One study did not achieve statistical analyses (the quality of evidence was already at “very low”). aq Includes one non-randomized study [47]. ar Studies reported mixed findings (the quality of evidence was downgraded from “low” to “very low”). as Includes two cross-over studies [32][49]. at Includes three randomized controlled studies [30][44][55]. au Studies reported mixed findings (the quality of evidence was downgraded from “high” to “moderate”). av Inconsistencies have been reported in the unit used in the results (the quality of evidence was downgraded from “moderate” to “low”). aw Includes four non-randomized controlled studies [43][46][51][53]. ax Studies reported mixed findings (the quality of evidence was downgraded from “low” to “very low”). ay Includes two randomized controlled studies [34][44]. az One study did not achieve statistical analyses (the quality of evidence was downgraded from “high” to “moderate”).
5. Conclusions
Active desks appear as a promising tool to reduce sedentary behaviors in school environment. In the present state of knowledge, the effects of all active desks appear not equivalent, mainly due to the difference in body activation and energy expenditure. Regarding the relatively low number of available studies and the high degree of heterogeneity in terms of quality, design and methods, comparisons and conclusions remain difficult at the moment. The present systematic analysis calls for further well-designed studies to better understand the effects of the use of active desks among children and adolescents in order to inform policy and practice.
References
- Patterson, R.; McNamara, E.; Tainio, M.; de Sá, T.H.; Smith, A.D.; Sharp, S.J.; Edwards, P.; Woodcock, J.; Brage, S.; Wijndaele, K. Sedentary Behaviour and Risk of All-Cause, Cardiovascular and Cancer Mortality, and Incident Type 2 Diabetes: A Systematic Review and Dose Response Meta-Analysis. Eur. J. Epidemiol. 2018, 33, 811–829.Benden, M.E.; Blake, J.J.; Wendel, M.L.; Huber, J.C. The Impact of Stand-Biased Desks in Classrooms on Calorie Expenditure in Children. Am. J. Public Health 2011, 101, 1433–1436.
- Stamatakis, E.; Ekelund, U.; Ding, D.; Hamer, M.; Bauman, A.E.; Lee, I.-M. Is the Time Right for Quantitative Public Health Guidelines on Sitting? A Narrative Review of Sedentary Behaviour Research Paradigms and Findings. Br. J. Sports Med. 2019, 53, 377–382.Benden, M.E.; Wendel, M.L.; Jeffrey, C.E.; Zhao, H.; Morales, M.L. Within-Subjects Analysis of the Effects of a Stand-Biased Classroom Intervention on Energy Expenditure. J. Exerc. Physiol. Online 2012, 15, 9–20.
- Sedentary Behaviour Research Network Letter to the Editor: Standardized Use of the Terms “Sedentary” and “Sedentary Behaviours.”. Appl. Physiol. Nutr. Metab. 2012, 37, 540–542.Benden, M.E.; Zhao, H.; Jeffrey, C.E.; Wendel, M.L.; Blake, J.J. The Evaluation of the Impact of a Stand-Biased Desk on Energy Expenditure and Physical Activity for Elementary School Students. Int. J. Environ. Res. Public Health 2014, 11, 9361–9375.
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.M.; Altenburg, T.M.; Chinapaw, M.J.M. SBRN Terminology Consensus Project Participants Sedentary Behavior Research Network (SBRN)—Terminology Consensus Project Process and Outcome. Int. J. Behav. Nutr. Phys. Act 2017, 14, 75.Blake, J.J.; Benden, M.E.; Wendel, M.L. Using Stand/Sit Workstations in Classrooms: Lessons Learned From a Pilot Study in Texas. J. Public Health Manag. Pract. 2012, 18, 412–415.
- Thivel, D.; Tremblay, A.; Genin, P.M.; Panahi, S.; Rivière, D.; Duclos, M. Physical Activity, Inactivity, and Sedentary Behaviors: Definitions and Implications in Occupational Health. Front. Public Health 2018, 6.Clemes, S.A.; Barber, S.E.; Bingham, D.D.; Ridgers, N.D.; Fletcher, E.; Pearson, N.; Salmon, J.; Dunstan, D.W. Reducing Children’s Classroom Sitting Time Using Sit-to-Stand Desks: Findings from Pilot Studies in UK and Australian Primary Schools. J. Public Health (Oxf.) 2016, 38, 526–533.
- Forouzanfar, M.H.; Afshin, A.; Alexander, L.T.; Anderson, H.R.; Bhutta, Z.A.; Biryukov, S.; Brauer, M.; Burnett, R.; Cercy, K.; Charlson, F.J.; et al. Global, Regional, and National Comparative Risk Assessment of 79 Behavioural, Environmental and Occupational, and Metabolic Risks or Clusters of Risks, 1990–2015: A Systematic Analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1659–1724.Clemes, S.A.; Bingham, D.D.; Pearson, N.; Chen, Y.-L.; Edwardson, C.L.; McEachan, R.R.C.; Tolfrey, K.; Cale, L.; Richardson, G.; Fray, M.; et al. Stand Out in Class: Restructuring the Classroom Environment to Reduce Sitting Time – Findings from a Pilot Cluster Randomised Controlled Trial. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 55.
- Ding, D.; Lawson, K.D.; Kolbe-Alexander, T.L.; Finkelstein, E.A.; Katzmarzyk, P.T.; van Mechelen, W.; Pratt, M. The Economic Burden of Physical Inactivity: A Global Analysis of Major Non-Communicable Diseases. Lancet 2016, 388, 1311–1324.Dornhecker, M.; Blake, J.J.; Benden, M.; Zhao, H.; Wendel, M. The Effect of Stand-Biased Desks on Academic Engagement: An Exploratory Study. Int. J. Health Promot. Educ. 2015, 53, 271–280.
- Friedenreich, C.M.; Ryder-Burbidge, C.; McNeil, J. Physical Activity, Obesity and Sedentary Behavior in Cancer Etiology: Epidemiologic Evidence and Biologic Mechanisms. Mol. Oncol. 2020, n/a.Ee, J.; Parry, S.; de Oliveira, B.I.; McVeigh, J.A.; Howie, E.; Straker, L. Does a Classroom Standing Desk Intervention Modify Standing and Sitting Behaviour and Musculoskeletal Symptoms during School Time and Physical Activity during Waking Time? Int. J. Environ. Res. Public Health 2018, 15.
- Ekelund, U.; Steene-Johannessen, J.; Brown, W.J.; Fagerland, M.W.; Owen, N.; Powell, K.E.; Bauman, A.; Lee, I.-M. Does Physical Activity Attenuate, or Even Eliminate, the Detrimental Association of Sitting Time with Mortality? A Harmonised Meta-Analysis of Data from More than 1 Million Men and Women. Lancet 2016, 388, 1302–1310.Kidokoro, T.; Shimizu, Y.; Edamoto, K.; Annear, M. Classroom Standing Desks and Time-Series Variation in Sedentary Behavior and Physical Activity among Primary School Children. Int. J. Environ. Res. Public Health 2019, 16, 1892.
- Schmid, D.; Ricci, C.; Leitzmann, M.F. Associations of Objectively Assessed Physical Activity and Sedentary Time with All-Cause Mortality in US Adults: The NHANES Study. PLoS ONE 2015, 10, e0119591.Koepp, G.A.; Snedden, B.J.; Flynn, L.; Puccinelli, D.; Huntsman, B.; Levine, J.A. Feasibility Analysis of Standing Desks for Sixth Graders. ICAN 2012.
- Lee, I.-M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T. ; Lancet Physical Activity Series Working Group Effect of Physical Inactivity on Major Non-Communicable Diseases Worldwide: An Analysis of Burden of Disease and Life Expectancy. Lancet 2012, 380, 219–229.Mehta, R.K.; Shortz, A.E.; Benden, M.E. Standing Up for Learning: A Pilot Investigation on the Neurocognitive Benefits of Stand-Biased School Desks. Int. J. Environ. Res. Public Health 2015, 13.
- Paffenbarger, R.S.; Hyde, R.T.; Wing, A.L.; Hsieh, C.C. Physical Activity, All-Cause Mortality, and Longevity of College Alumni. N. Engl. J. Med. 1986, 314, 605–613.Parry, S.; IR de Oliveira, B.; McVeigh, J.A.; Ee, J.; Jacques, A.; Straker, L. Standing Desks in a Grade 4 Classroom over the Full School Year. Int. J. Environ. Res. Public Health 2019, 16, 3590.
- Janssen, X.; Mann, K.D.; Basterfield, L.; Parkinson, K.N.; Pearce, M.S.; Reilly, J.K.; Adamson, A.J.; Reilly, J.J. Development of Sedentary Behavior across Childhood and Adolescence: Longitudinal Analysis of the Gateshead Millennium Study. Int. J. Behav. Nutr. Phys. Act 2016, 13, 88.Pickens, A.W.; Benden, M.E.; Schneider, D.E.; Zhao, H. Use of Stand-Biased Desks to Reduce Sedentary Time in High School Students: A Pilot Study. Int. J. Child Health Nutr. 2016, 5, 75–78.
- Farooq, M.A.; Parkinson, K.N.; Adamson, A.J.; Pearce, M.S.; Reilly, J.K.; Hughes, A.R.; Janssen, X.; Basterfield, L.; Reilly, J.J. Timing of the Decline in Physical Activity in Childhood and Adolescence: Gateshead Millennium Cohort Study. Br. J. Sports Med. 2018, 52, 1002–1006.Sherry, A.P.; Pearson, N.; Ridgers, N.D.; Johnson, W.; Barber, S.E.; Bingham, D.D.; Nagy, L.C.; Clemes, S.A. Impacts of a Standing Desk Intervention within an English Primary School Classroom: A Pilot Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 7048.
- Hallal, P.C.; Andersen, L.B.; Bull, F.C.; Guthold, R.; Haskell, W.; Ekelund, U. Global Physical Activity Levels: Surveillance Progress, Pitfalls, and Prospects. Lancet 2012, 380, 247–257.Sprengeler, O.; Hebestreit, A.; Gohres, H.; Bucksch, J.; Buck, C. Effects of Installing Height-Adjustable Standing Desks on Daily and Domain-Specific Duration of Standing, Sitting, and Stepping in 3rd Grade Primary School Children. Front. Public Health 2020, 8.
- Saunders, T.J.; Chaput, J.-P.; Tremblay, M.S. Sedentary Behaviour as an Emerging Risk Factor for Cardiometabolic Diseases in Children and Youth. Can. J. Diabetes 2014, 38, 53–61.Sudholz, B.; Timperio, A.; Ridgers, N.D.; Dunstan, D.W.; Baldock, R.; Holland, B.; Salmon, J. The Impact and Feasibility of Introducing Height-Adjustable Desks on Adolescents’ Sitting in a Secondary School Classroom. AIMS Public Health 2016, 3, 274–287.
- Andersen, L.B.; Harro, M.; Sardinha, L.B.; Froberg, K.; Ekelund, U.; Brage, S.; Anderssen, S.A. Physical Activity and Clustered Cardiovascular Risk in Children: A Cross-Sectional Study (The European Youth Heart Study). Lancet 2006, 368, 299–304.Swartz, A.M.; Tokarek, N.R.; Lisdahl, K.; Maeda, H.; Strath, S.J.; Cho, C.C. Do Stand-Biased Desks in the Classroom Change School-Time Activity and Sedentary Behavior? Int. J. Environ. Res. Public Health 2019, 16, 933.
- Carson, V.; Hunter, S.; Kuzik, N.; Gray, C.E.; Poitras, V.J.; Chaput, J.-P.; Saunders, T.J.; Katzmarzyk, P.T.; Okely, A.D.; Connor Gorber, S.; et al. Systematic Review of Sedentary Behaviour and Health Indicators in School-Aged Children and Youth: An Update. Appl. Physiol. Nutr. Metab. 2016, 41, S240–S265.Verloigne, M.; Ridgers, N.D.; De Bourdeaudhuij, I.; Cardon, G. Effect and Process Evaluation of Implementing Standing Desks in Primary and Secondary Schools in Belgium: A Cluster-Randomised Controlled Trial. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 94.
- Ekelund, U.; Luan, J.; Sherar, L.; Esliger, D.; Griew, P.; Cooper, A. Moderate to Vigorous Physical Activity and Sedentary Time and Cardiometabolic Risk Factors in Children and Adolescents. JAMA 2012, 307, 704–712.Wendel, M.L.; Benden, M.E.; Zhao, H.; Jeffrey, C. Stand-Biased Versus Seated Classrooms and Childhood Obesity: A Randomized Experiment in Texas. Am. J. Public Health 2016, 106, 1849–1854.
- Martinez-Gomez, D.; Eisenmann, J.; Gómez-Martínez, S.; Veses, A.; Marcos, A.; Veiga, O. Sedentary Behavior, Adiposity and Cardiovascular Risk Factors in Adolescents. The AFINOS Study. Revista Española de Cardiología 2010, 63, 277–285.Wick, K.; Faude, O.; Manes, S.; Zahner, L.; Donath, L. I Can Stand Learning: A Controlled Pilot Intervention Study on the Effects of Increased Standing Time on Cognitive Function in Primary School Children. Int. J. Environ. Res. Public Health 2018, 15, 356.
- Väistö, J.; Eloranta, A.-M.; Viitasalo, A.; Tompuri, T.; Lintu, N.; Karjalainen, P.; Lampinen, E.-K.; Ågren, J.; Laaksonen, D.E.; Lakka, H.-M.; et al. Physical Activity and Sedentary Behaviour in Relation to Cardiometabolic Risk in Children: Cross-Sectional Findings from the Physical Activity and Nutrition in Children (PANIC) Study. Int. J. Behav. Nutr. Phys. Act 2014, 11, 55.Fedewa, A.; Cornelius, C.; Ahn, S. The Use of Bicycle Workstations to Increase Physical Activity in Secondary Classrooms. Health Psychol. Rep. 2017, 6, 60–74.
- Esteban-Cornejo, I.; Martinez-Gomez, D.; Sallis, J.F.; Cabanas-Sánchez, V.; Fernández-Santos, J.; Castro-Piñero, J.; Veiga, O.L. Objectively Measured and Self-Reported Leisure-Time Sedentary Behavior and Academic Performance in Youth: The UP&DOWN Study. Prev. Med. 2015, 77, 106–111.Ruiter, M.; Eielts, C.; Loyens, S.; Paas, F. Comparing Cognitive Control Performance During Seated Rest and Self-Paced Cycling on a Desk Bike in Preadolescent Children. J. Phys. Act. Health 2019, 16, 533–539.
- Syväoja, H.J.; Kantomaa, M.T.; Ahonen, T.; Hakonen, H.; Kankaanpää, A.; Tammelin, T.H. Physical Activity, Sedentary Behavior, and Academic Performance in Finnish Children. Med. Sci. Sports Exerc. 2013, 45, 2098–2104.Torbeyns, T.; de Geus, B.; Bailey, S.; Decroix, L.; Cutsem, J.V.; Pauw, K.D.; Meeusen, R. Bike Desks in the Classroom: Energy Expenditure, Physical Health, Cognitive Performance, Brain Functioning, and Academic Performance. J. Phys. Act. Health 2017, 14, 429–439.
- Syväoja, H.J.; Kankaanpää, A.; Kallio, J.; Hakonen, H.; Kulmala, J.; Hillman, C.H.; Pesonen, A.-K.; Tammelin, T.H. The Relation of Physical Activity, Sedentary Behaviors, and Academic Achievement Is Mediated by Fitness and Bedtime. J. Phys. Act Health 2018, 15, 135–143.Erwin, H.E.; Fedewa, A.; Ahn, S.; Thornton, M. Elementary Students’ Physical Activity Levels and Behavior When Using Stability Balls. Am. J. Occup. Ther. 2016, 70, 700220010p1–700220010p7.
- Kuh, D.; Shlomo, Y.B. A Life Course Approach to Chronic Disease Epidemiology; OUP Oxford: Oxford, UK, 2004; ISBN 978-0-19-857815-4.Fedewa, A.; Davis, M.A.C.; Ahn, S. Effects of Stability Balls on Children’s On-Task Behavior, Academic Achievement, and Discipline Referrals: A Randomized Controlled Trial. Am. J. Occup. Ther. 2015, 69, 6902220020p1–6902220020p9.
- Thivel, D.; Chaput, J.P.; Duclos, M. Integrating Sedentary Behavior in the Theoretical Model Linking Childhood to Adulthood Activity and Health? An Updated Framework. Physiol. Behav. 2018, 196, 33–35.
- Patton, G.C.; Bond, L.; Carlin, J.B.; Thomas, L.; Butler, H.; Glover, S.; Catalano, R.; Bowes, G. Promoting Social Inclusion in Schools: A Group-Randomized Trial of Effects on Student Health Risk Behavior and Well-Being. Am. J. Public Health 2006, 96, 1582–1587.
- Pinel-Jacquemin, S.; Florin, A.; Guimard, P. Bien-Être Des Élèves à l’école et Promotion de Leur Santé; Ministère de l’éducation nationale et de la jeunesse; Conseil national d’évaluation du système scolaire (CNESCO): Paris, France, 2016.
- Ayala, A.M.C.; Sudholz, B.; Salmon, J.; Dunstan, D.W.; Ridgers, N.D.; Arundell, L.; Timperio, A. The Impact of Height-Adjustable Desks and Prompts to Break-up Classroom Sitting on Adolescents’ Energy Expenditure, Adiposity Markers and Perceived Musculoskeletal Discomfort. PLoS ONE 2018, 13, e0203938.
- Fedewa, A.; Cornelius, C.; Ahn, S. The Use of Bicycle Workstations to Increase Physical Activity in Secondary Classrooms. Health Psychol. Rep. 2017, 6, 60–74.
- Clemes, S.A.; Barber, S.E.; Bingham, D.D.; Ridgers, N.D.; Fletcher, E.; Pearson, N.; Salmon, J.; Dunstan, D.W. Reducing Children’s Classroom Sitting Time Using Sit-to-Stand Desks: Findings from Pilot Studies in UK and Australian Primary Schools. J. Public Health (Oxf.) 2016, 38, 526–533.
- Ee, J.; Parry, S.; de Oliveira, B.I.; McVeigh, J.A.; Howie, E.; Straker, L. Does a Classroom Standing Desk Intervention Modify Standing and Sitting Behaviour and Musculoskeletal Symptoms during School Time and Physical Activity during Waking Time? Int. J. Environ. Res. Public Health 2018, 15.
- Erwin, H.E.; Fedewa, A.; Ahn, S.; Thornton, M. Elementary Students’ Physical Activity Levels and Behavior When Using Stability Balls. Am. J. Occup. Ther. 2016, 70, 700220010p1–700220010p7.
- Torbeyns, T.; de Geus, B.; Bailey, S.; Decroix, L.; Cutsem, J.V.; Pauw, K.D.; Meeusen, R. Bike Desks in the Classroom: Energy Expenditure, Physical Health, Cognitive Performance, Brain Functioning, and Academic Performance. J. Phys. Act. Health 2017, 14, 429–439.
- Benden, M.E.; Blake, J.J.; Wendel, M.L.; Huber, J.C. The Impact of Stand-Biased Desks in Classrooms on Calorie Expenditure in Children. Am. J. Public Health 2011, 101, 1433–1436.
- Benden, M.E.; Zhao, H.; Jeffrey, C.E.; Wendel, M.L.; Blake, J.J. The Evaluation of the Impact of a Stand-Biased Desk on Energy Expenditure and Physical Activity for Elementary School Students. Int. J. Environ. Res. Public Health 2014, 11, 9361–9375.
- Clemes, S.A.; Bingham, D.D.; Pearson, N.; Chen, Y.-L.; Edwardson, C.L.; McEachan, R.R.C.; Tolfrey, K.; Cale, L.; Richardson, G.; Fray, M.; et al. Stand Out in Class: Restructuring the Classroom Environment to Reduce Sitting Time – Findings from a Pilot Cluster Randomised Controlled Trial. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 55.
- Verloigne, M.; Ridgers, N.D.; De Bourdeaudhuij, I.; Cardon, G. Effect and Process Evaluation of Implementing Standing Desks in Primary and Secondary Schools in Belgium: A Cluster-Randomised Controlled Trial. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 94.
- Wendel, M.L.; Benden, M.E.; Zhao, H.; Jeffrey, C. Stand-Biased Versus Seated Classrooms and Childhood Obesity: A Randomized Experiment in Texas. Am. J. Public Health 2016, 106, 1849–1854.
- Fedewa, A.; Davis, M.A.C.; Ahn, S. Effects of Stability Balls on Children’s On-Task Behavior, Academic Achievement, and Discipline Referrals: A Randomized Controlled Trial. Am. J. Occup. Ther. 2015, 69, 6902220020p1–6902220020p9.
- Blake, J.J.; Benden, M.E.; Wendel, M.L. Using Stand/Sit Workstations in Classrooms: Lessons Learned From a Pilot Study in Texas. J. Public Health Manag. Pract. 2012, 18, 412–415.
- Dornhecker, M.; Blake, J.J.; Benden, M.; Zhao, H.; Wendel, M. The Effect of Stand-Biased Desks on Academic Engagement: An Exploratory Study. Int. J. Health Promot. Educ. 2015, 53, 271–280.
- Kidokoro, T.; Shimizu, Y.; Edamoto, K.; Annear, M. Classroom Standing Desks and Time-Series Variation in Sedentary Behavior and Physical Activity among Primary School Children. Int. J. Environ. Res. Public Health 2019, 16, 1892.
- Sherry, A.P.; Pearson, N.; Ridgers, N.D.; Johnson, W.; Barber, S.E.; Bingham, D.D.; Nagy, L.C.; Clemes, S.A. Impacts of a Standing Desk Intervention within an English Primary School Classroom: A Pilot Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 7048.
- Sudholz, B.; Timperio, A.; Ridgers, N.D.; Dunstan, D.W.; Baldock, R.; Holland, B.; Salmon, J. The Impact and Feasibility of Introducing Height-Adjustable Desks on Adolescents’ Sitting in a Secondary School Classroom. AIMS Public Health 2016, 3, 274–287.
- Wick, K.; Faude, O.; Manes, S.; Zahner, L.; Donath, L. I Can Stand Learning: A Controlled Pilot Intervention Study on the Effects of Increased Standing Time on Cognitive Function in Primary School Children. Int. J. Environ. Res. Public Health 2018, 15, 356.
- Benden, M.E.; Wendel, M.L.; Jeffrey, C.E.; Zhao, H.; Morales, M.L. Within-Subjects Analysis of the Effects of a Stand-Biased Classroom Intervention on Energy Expenditure. J. Exerc. Physiol. Online 2012, 15, 9–20.
- Koepp, G.A.; Snedden, B.J.; Flynn, L.; Puccinelli, D.; Huntsman, B.; Levine, J.A. Feasibility Analysis of Standing Desks for Sixth Graders. ICAN 2012.
- Mehta, R.K.; Shortz, A.E.; Benden, M.E. Standing Up for Learning: A Pilot Investigation on the Neurocognitive Benefits of Stand-Biased School Desks. Int. J. Environ. Res. Public Health 2015, 13.
- Ruiter, M.; Eielts, C.; Loyens, S.; Paas, F. Comparing Cognitive Control Performance During Seated Rest and Self-Paced Cycling on a Desk Bike in Preadolescent Children. J. Phys. Act. Health 2019, 16, 533–539.
- Pickens, A.W.; Benden, M.E.; Schneider, D.E.; Zhao, H. Use of Stand-Biased Desks to Reduce Sedentary Time in High School Students: A Pilot Study. Int. J. Child Health Nutr. 2016, 5, 75–78.
- Parry, S.; IR de Oliveira, B.; McVeigh, J.A.; Ee, J.; Jacques, A.; Straker, L. Standing Desks in a Grade 4 Classroom over the Full School Year. Int. J. Environ. Res. Public Health 2019, 16, 3590.
- Sprengeler, O.; Hebestreit, A.; Gohres, H.; Bucksch, J.; Buck, C. Effects of Installing Height-Adjustable Standing Desks on Daily and Domain-Specific Duration of Standing, Sitting, and Stepping in 3rd Grade Primary School Children. Front. Public Health 2020, 8.
- Swartz, A.M.; Tokarek, N.R.; Lisdahl, K.; Maeda, H.; Strath, S.J.; Cho, C.C. Do Stand-Biased Desks in the Classroom Change School-Time Activity and Sedentary Behavior? Int. J. Environ. Res. Public Health 2019, 16, 933.
- Guyatt, G.H.; Oxman, A.D.; Vist, G.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Montori, V.; Akl, E.A.; Djulbegovic, B.; Falck-Ytter, Y.; et al. GRADE Guidelines: 4. Rating the Quality of Evidence—Study Limitations (Risk of Bias). J. Clin. Epidemiol. 2011, 64, 407–415.