Several performance-enhancing or ergogenic drugs have been linked to both significant adverse cardiovascular effects and increased cardiovascular risk. Even with increased scrutiny on the governance of performance-enhancing drugs (PEDs) in professional sport and heightened awareness of the associated cardiovascular risk, there are some who are prepared to risk their use to gain competitive advantage. Caffeine is the most commonly consumed drug in the world and its ergogenic properties have been reported for decades. Thus, the removal of caffeine from the World Anti-Doping Agency (WADA) list of banned substances, in 2004, has naturally led to an exponential rise in its use amongst athletes.
- sports cardiology
- athlete
- caffeine
1. Introduction
Caffeine (1,3,7-Trimethylxanthine) is a popular workplace substance that has been well-researched, with its ergogenic effects being known for centuries [1]. Caffeine has a wide range of acute benefits that includes an increase in alertness and concentration, accompanied by a reduction in fatigue and pain perception [2][3]. As a result, its use has become highly prevalent amongst athletes, especially after 2004, when it was removed from the World Anti-Doping Agency (WADA) list of banned substances; it was, therefore unsurprising when a study reported that 74% of urine samples from athletes, between 2004 to 2008, demonstrated measurable levels [1]. Common physiological effects of caffeine on the body include an increase in heart rate, catecholamine levels, blood lactate, free fatty acids and glycerol [4]. More significantly, its use has illustrated benefits in both endurance-based and high-intensity exercise, permitting the athlete to train longer and at a greater intensity. A recent meta-analysis yielded a positive relationship of caffeine on muscle strength, muscle endurance and anaerobic power [5]. As a result, it is recommended that ingestion of 3–9 mg/kg approximately 60 min prior to exercise may provide the extra competitive advantage for the athlete [1]. Nonetheless, the response to caffeine is multifaceted, influenced by both genetic and non-genetic predilections, with there being inter-subject variation in response to caffeine consumption, and this heterogeneous response makes it difficult to extrapolate the objective impact of caffeine as a vital ingredient to athletic prowess.
In contrast, anabolic androgenic steroids (AASs), synthetic derivatives of testosterone, have been abused by athletes since the 1950s for their ability to increase muscle mass and improve athletic performance. The terms anabolic and androgenic refer to muscle hypertrophy and increased male sex characteristics, respectively. AASs are artificial substances that act on androgen receptors and are commonly used in the treatment of metabolic or catabolic disorders and other chronic conditions related to low testosterone [6]. More significantly, its misuse stems from the means of achieving a lean and muscular body type, with the potential of shielding the user from muscle fibre damage, through enhanced protein synthesis during recovery. There are multiple manufactured forms, most of which are designed to optimise muscle growth whilst minimising the undesired androgenic effects [6]. Steroid abuse has dramatically increased over the past two decades in the general population who live in an increasingly image-obsessed era. Its users are typically 20–30-year-old males, who participate in recreational exercise largely composed of weight training [6]. Globally, it is estimated that 6.4% of males and 1.6% of females use AASs [7]. The second highest prevalence of users beyond recreational sportspeople (18.4%) are athletes (13.4%) [8]. Whilst anabolic androgenic steroids can play an important role in clinical treatment of endocrine disorders there are several established adverse outcomes, if misused, that includes an increased risk of cardiovascular disease (CVD), risk of tendon ruptures, hepatorenal disorders and psychiatric symptoms. The doses are often 5–15 times higher than recommended levels, with athletes experiencing a higher probability of adverse cardiovascular events that includes stroke and myocardial infarction (MI) [9]. Preceding these events are hypertension and left ventricular (LV) hypertrophy, both independent predictors of cardiovascular mortality and morbidity [10][11]. There are, however, many obstacles to the investigation of the dangers of AASs, due to the dose never being reliably known, to polypharmacy or the ethical restrictions of conducting research studies [6].
2. Caffeine as a Performance Enhancing Agent
In many sports, changes in performance of 1% may be the difference between first or second place [12]. Caffeine is a readily available performance enhancing aid that improves athletic ability across virtually all sporting disciplines. Historically, it was recommended to be banned in 1939, due to its ergogenic properties that may influence sporting accomplishments. Since its legalisation in 2004, it has become a major source for athletes, commonly being in the form of energy drinks, but may vary in the form of a gum, gel, pill or inhaler. Through fat mobilisation and thus sparing of the glycogen reserve, it diminishes the impact of fatigue, pain and effort that is associated with exercise, leading to the more significant motives of athletes for its consumption. A typical 250 mL energy drink (ED) may contain up to 80 mg of caffeine, similar to that in filtered coffee (90 mg), and twice the amount of that in tea (30 mg); additional substances that complement the influence of caffeine include ginseng, taurine and guarana [13][14][15][16][17].
Caffeine use may be classified as low, moderate or high, with ingestion of ~3 mg/kg (~200 mg for a 70 kg individual; 1–2 small cups of coffee) being considered low, 5–6 mg/kg considered moderate and ~10–13 mg/kg viewed as high [17]. It should be noted that the dose-response relationship between caffeine and athletic performance has yet to be established, with low dose caffeine appearing to exhibit the most ergogenic effect on athletes. For instance, caffeine containing drinks, with a dose equivalence to 3 mg/kg, have shown an increased ability of football players in sprinting, jumping and the distance covered [18]. Further meta-analyses investigating the role of caffeine have demonstrated a significant increase in jump height, muscular endurance, aerobic endurance performance and muscle strength [19].
Like most substances, caffeine, when consumed in larger doses, may result in side effects that includes dehydration, seizures, migraines, insomnia, arrhythmias, gastrointestinal problems and psychological permutations [15][16][20].
2.1. Caffeine Pharmacology and Cardiac Physiology
Caffeine is rapidly absorbed by the body, with its concentration peaking between 40 to 80 min, and rising to ~15–20 µmol/L with a low caffeine dose, ~40 µmol/L with a moderate and ~60–70 µmol/L with a high dose. It appears in the blood within 5–15 min of ingestion and has a long half-life (3–5 h) [21]. For both female and male athletes, for a given dose of caffeine, it appears that the concentration of caffeine and its metabolites are the same [22][23].
The effects of caffeine are exerted primarily through the blockade of adenosine receptors (subtypes A1 and A2), which are found throughout the myocardium and coronary circulation; they are also found in the brain, adipocytes, skeletal and smooth muscle (Figure 1). The result in the competitive blockade of these receptors leads to an increase in peripheral vascular resistance, sympathetic tone and increase in renin, subsequently amplifying the heart rate, cardiac contractility and blood pressure [24]. Secondary metabolic changes of caffeine include stimulating the secretion of epinephrine.
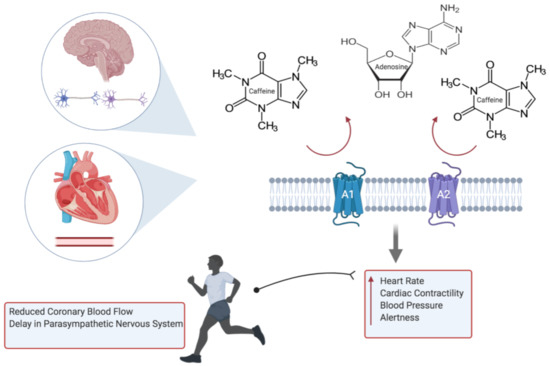
Figure 1. Caffeine inhibits the action of adenosine through the blockade of A1 and A2 receptors, resulting in elevated heart rate, blood pressure, cardiac contractility and alertness. Subsequent adverse cardiovascular events during exercise include potentiation of hypoxic damage to cardiac myocytes, through failure in relaxation of the coronary vessels, and arrhythmias (created with BioRender.com).
Whilst the concerns of caffeine on overall health has permeated through society, there are many epidemiological studies that have shown its benefit to overall mortality, and in particular cardiac disease [25]. Moreover, although historical studies have demonstrated an increased risk in MI and CVD [26][27], a study of 45,589 men and 85,747 women followed up for 2 and 10 years, respectively, did not show a substantial risk in CVD [28]. Caffeine may, however, conversely attenuate the physiological response to exercise, such that there may be reduced coronary blood flow or response of the endothelial cell in mediating the vascular tone during exercise, which signifies a potential risk to an athlete with silent coronary disease. Other impacts of caffeine include a delayed return of the parasympathetic nervous system, and with a state of sustained sympathetic activity, this may confer an increased risk of life-threatening arrhythmias [21].
2.2. Caffeine and Risk of Arrhythmia
Whilst many studies have reported the arrhythmogenic effect of caffeine, it has not been replicated on large population studies. With the consumption of caffeine being ubiquitous in Western society, the widely held belief that caffeine may contribute to arrhythmia or the risk and development of coronary heart disease may not be evidence-based [24][25][29][30][31][32]. Intoxication of caffeine, however, is still reported, demonstrating its potential in provoking fatal arrhythmias [33]. Physiologically, through the blockade of calcium reuptake into the sarcoplasmic reticulum, and thus a rise in intracellular calcium, the potential of atrial arrhythmia, through enhanced automaticity of atrial pacemaker cells, exists; three cups of coffee (250 mg) have shown to increase both epi- and norepinephrine [34]. More importantly, energy drinks often contain caffeine at a significantly higher concentration than either coffee or tea; the stimulant properties of other compounds in EDs, such as taurine, complicates matters further. Taurine, for instance, is suggested to increase calcium accumulation in the sarcoplasmic reticulum, favouring the excitation-contraction of skeletal muscles, but may also induce unfavourable arrhythmias [35].
It could be argued that the absence of risk may not relate to athletes or those who harbour an underlying abnormal cardiac substrate, especially as the amount of caffeine consumed through energy drinks may be invariably higher. For instance, there has been reports of EDs prolonging QTc and unmasking Brugada syndrome [34]. Another important impact of caffeine includes the augmentation of ryanodine receptors, that may further lead to an increase in calcium release within cardiac cells, affecting the heart’s ability to contract and use oxygen, which may predispose to arrhythmias [36].
On the other hand, when attempting to explore the relationship between caffeine and arrhythmias in those with pre-existing cardiac disease, there failed to be a connection, suggesting the complex pharmacodynamics of caffeine [33].
2.3. Caffeine Genetics
It is evident that genetic factors demonstrate a huge role on the individual response to the effects of caffeine [37][38][39]. Whilst its mechanisms may not be well defined, there are certain drivers of these individual differences; notable genes include CYP1A2, ADORA2A and catechol-O-methyltransferase (COMT) [40]. Of the most significance is CYP1A2, which is involved in the breakdown of caffeine and has two alleles (A & C), dichotomising into either fast or slow metabolisers, respectively. The significance of this phenomenon is that those who are slow metabolisers, who consume moderate (3–4 cups) amounts of coffee have a greater risk of hypertension and MI [1]. This is also reflected in athletes, with those who are fast metabolisers showing greater improvement in performance; this may be due a rapid accumulation of caffeine metabolites, and may reflect why timing of caffeine consumption becomes important [1].
In contrast, polymorphisms affecting ADORA2A could lead to an individual to experience greater sleep disturbance, impacting athletes that compete in the evening, or increased anxiety resulting in poor competition performance
.
2.4. Caffeine in Sudden Cardiac Death
Sudden cardiac death (SCD) is defined as an unexpected death or arrest, presumed to be secondary to a cardiac cause, within 1 hour of symptoms or, if unwitnessed, within 24. Energy drinks has been associated with coronary vasospasm and ischaemia, arrhythmias, endothelial dysfunction and increased platelet aggregation
. Its use has been a particular concern amongst the younger athletes, where case reports of sudden cardiac death were in part attributed to the consumption of energy drinks
. However, whilst no direct link between caffeine and its supposed harmful effects on the heart exist, further studies are required to establish its true safety, particularly in those with underlying electrical or structural cardiac abnormalities. Additional studies would be important in recognising the effects of strength and delivery of caffeine, and the effects of age and genetic expression on the individual’s response to caffeine.
References
- Pickering, C.; Kiely, J. Are the Current Guidelines on Caffeine Use in Sport Optimal for Everyone? Inter-individual Vari-ation in Caffeine Ergogenicity, and a Move Towards Personalised Sports Nutrition. Sports Med. 2018, 48, 7–16.
- Berglund, B.; Hemmingsson, P. Effects of Caffeine Ingestion on Exercise Performance at Low and High Altitudes in Cross-Country Skiers. Int. J. Sports Med. 1982, 3, 234–236.
- Stadheim, H.K.; Nossum, E.M.; Olsen, R.; Spencer, M.; Jensen, J. Caffeine improves performance in double poling during acute exposure to 2,000-m altitude. J. Appl. Physiol. 2015, 119, 1501–1509.
- Powers, S.K.; Byrd, R.J.; Tulley, R.; Callender, T. Effects of caffeine ingestion on metabolism and performance during graded exercise. Graefe’s Arch. Clin. Exp. Ophthalmol. 1983, 50, 301–307.
- Grgic, J.; Grgic, I.; Pickering, C.; Schoenfeld, B.J.; Bishop, D.J.; Virgile, A.; Pedisic, Z. Infographic. Wake up and smell the coffee: Caffeine supplementation and exercise performance. Br. J. Sports Med. 2020, 54, 304–305.
- Mullen, C.; Whalley, B.J.; Schifano, F.; Baker, J.S. Anabolic androgenic steroid abuse in the United Kingdom: An update. Br. J. Pharmacol. 2020, 177, 2180–2198.
- Sagoe, D.; Molde, H.; Andreassen, C.S.; Torsheim, T.; Pallesen, S. The global epidemiology of anabolic-androgenic steroid use: A meta-analysis and meta-regression analysis. Ann. Epidemiol. 2014, 24, 383–398.
- Reyes-Vallejo, L. Current use and abuse of anabolic steroids. Actas Urológicas Españolas (Engl. Ed.) 2020, 44, 309–313.
- Tsatsakis, A.; Docea, A.O.; Calina, D.; Tsarouhas, K.; Zamfira, L.-M.; Mitrut, R.; Sharifi-Rad, J.; Kovatsi, L.; Siokas, V.; Dardiotis, E.; et al. A Mechanistic and Pathophysiological Approach for Stroke Associated with Drugs of Abuse. J. Clin. Med. 2019, 8, 1295.
- McCullough, D.; Webb, R.; Enright, K.J.; Lane, K.E.; McVeigh, J.; Stewart, C.E.; Davies, I.G. How the love of muscle can break a heart: Impact of anabolic androgenic steroids on skeletal muscle hypertrophy, metabolic and cardiovascular health. Rev. Endocr. Metab. Disord. 2020, 1–17.
- Payne, J.R.; Kotwinski, P.J.; E Montgomery, H. Cardiac effects of anabolic steroids. Heart 2004, 90, 473–475.
- Southward, K.; Rutherfurd-Markwick, K.J.; Ali, A. The Effect of Acute Caffeine Ingestion on Endurance Performance: A Systematic Review and Meta-Analysis. Sports Med. 2018, 48, 1913–1928.
- Babu, K.M.; Church, R.J.; Lewander, W. Energy Drinks: The New Eye-Opener For Adolescents. Clin. Pediatr. Emerg. Med. 2008, 9, 35–42.
- Espinola, E.; Dias, R.; Mattei, R.; Carlini, E. Pharmacological activity of Guarana (Paullinia cupana Mart.) in laboratory animals. J. Ethnopharmacol. 1997, 55, 223–229.
- Glatter, K.A.; Myers, R.; Chiamvimonvat, N. Recommendations regarding dietary intake and caffeine and alcohol con-sumption in patients with cardiac arrhythmias: What do you tell your patients to do or not to do? Curr. Treat. Options Cardiovasc. Med. 2012, 14, 529–535.
- Seifert, S.M.; Schaechter, J.L.; Hershorin, E.R.; Lipshultz, S.E. Health Effects of Energy Drinks on Children, Adolescents, and Young Adults. Pediatrics 2011, 127, 511–528.
- Spriet, L.L. Exercise and Sport Performance with Low Doses of Caffeine. Sports Med. 2014, 44, 175–184.
- Del Coso, J.; Muñoz-Fernández, V.E.; Muñoz, G.; Fernández-Elías, V.E.; Ortega, J.F.; Hamouti, N.; Barbero, J.C.; Muñoz-Guerraet, J. Effects of a caffeine containing energy drink on simulated soccer performance. PLoS ONE 2012, 7, e31380.
- Pickering, C.; Grgic, J. Caffeine and Exercise: What Next? Sports Med. 2019, 49, 1007–1030.
- Trapp, G.S.; Allen, K.; O’Sullivan, T.A.; Robinson, M.; Jacoby, P.; Oddy, W.H. ENERGY DRINK CONSUMPTION IS ASSOCIATED WITH ANXIETY IN AUSTRALIAN YOUNG ADULT MALES. Depress. Anxiety 2013, 31, 420–428.
- Graham, T.E.; Rush, J.W.E.; Van Soeren, M.H. Caffeine and Exercise: Metabolism and Performance. Can. J. Appl. Physiol. 1994, 19, 111–138.
- Gonzaga, L.A.; Vanderlei, L.C.M.; Gomes, R.L.; Valenti, V.E. Caffeine affects autonomic control of heart rate and blood pressure recovery after aerobic exercise in young adults: A crossover study. Sci. Rep. 2017, 7, 14091.
- Skinner, T.L.; Desbrow, B.; Arapova, J.; Schaumberg, M.A.; Osborne, J.; Grant, G.D.; Anoopkumar-Dukie, S.; Leveritt, M.D. Women Experience the Same Ergogenic Response to Caffeine as Men. Med. Sci. Sports Exerc. 2019, 51, 1195–1202.
- Haller, C.A.; Jacob, P.; Benowitz, N.L. Pharmacology of ephedra alkaloids and caffeine after single-dose dietary supplement use*. Clin. Pharmacol. Ther. 2002, 71, 421–432.
- Loftfield, E.; Freedman, N.D.; Graubard, B.I.; Guertin, K.A.; Black, A.; Huang, W.-Y.; Shebl, F.M.; Mayne, S.T.; Sinha, R. Association of Coffee Consumption With Overall and Cause-Specific Mortality in a Large US Prospective Cohort Study. Am. J. Epidemiol. 2015, 182, 1010–1022.
- Rosenberg, L.; Palmer, J.R.; Kelly, J.P.; Kaufman, D.W.; Shapiro, S. Coffee drinking and nonfatal myocardial infarction in men under 55 years of age. Am. J. Epidemiol. 1988, 128, 570–578.
- Lacroix, A.Z.; Mead, L.A.; Liang, K.-Y.; Thomas, C.B.; Pearson, T.A. Coffee Consumption and the Incidence of Coronary Heart Disease. New Engl. J. Med. 1986, 315, 977–982.
- Happonen, P.; Voutilainen, S.; Salonen, J.T. Coffee Drinking Is Dose-Dependently Related to the Risk of Acute Coronary Events in Middle-Aged Men. J. Nutr. 2004, 134, 2381–2386.
- Goldfarb, M.; Tellier, C.; Thanassoulis, G. Review of Published Cases of Adverse Cardiovascular Events After Ingestion of Energy Drinks. Am. J. Cardiol. 2014, 113, 168–172.
- Avcı, S.; Sarıkaya, R.; Büyükcam, F. Death of a young man after overuse of energy drink. Am. J. Emerg. Med. 2013, 31, 1624.e3–1624.e4.
- Frost, L.; Vestergaard, P. Caffeine and risk of atrial fibrillation or flutter: The Danish Diet, Cancer, and Health Study. Am. J. Clin. Nutr. 2005, 81, 578–582.
- Sanchis-Gomar, F.; Pareja-Galeano, H.; Cervellin, G.; Lippi, G.; Earnest, C.P. Energy Drink Overconsumption in Adolescents: Implications for Arrhythmias and Other Cardiovascular Events. Can. J. Cardiol. 2015, 31, 572–575.
- Zuchinali, P.; Zimerman, A.; Giaretta, V.; Salamoni, J.; Fracasso, B.; Pimentel, M.; Souza, G.C.; Chemello, D.; I Zimerman, L.; E Rohde, L. Short-term Effects of High-Dose Caffeine on Cardiac Arrhythmias in Patients With Heart Failure: A Randomized Clinical Trial. JAMA Intern. Med. 2016, 176, 1752–1759.
- Voskoboinik, A.; Kalman, J.M.; Kistler, P.M. Caffeine and Arrhythmias: Time to Grind the Data. JACC Clin. Electrophysiol. 2018, 4, 425–432.
- Souza, D.B.; Del Coso, J.; Casonatto, J.; Polito, M.D. Acute effects of caffeine-containing energy drinks on physical perfor-mance: A systematic review and meta-analysis. Eur. J. Nutr. 2017, 56, 13–27.
- Fletcher, E.A.; Lacey, C.S.; Aaron, M.; Kolasa, M.; Occiano, A.; Shah, S.A. Randomized Controlled Trial of High-Volume Energy Drink Versus Caffeine Consumption on ECG and Hemodynamic Parameters. J. Am. Hear. Assoc. 2017, 6.
- Cornelis, M.C.; Monda, K.L.; Yu, K.; Paynter, N.; Azzato, E.M.; Bennett, S.N.; Berndt, S.I.; Boerwinkle, E.; Chanock, S.; Chatterjee, N.; et al. Genome-Wide Meta-Analysis Identifies Regions on 7p21 (AHR) and 15q24 (CYP1A2) As Determinants of Habitual Caffeine Consumption. PLoS Genet. 2011, 7, e1002033.
- Sulem, P.; Gudbjartsson, D.F.; Geller, F.; Prokopenko, I.; Feenstra, B.; Aben, K.K.H.; Franke, B.; den Heijer, M.; Kovacs, P.; Stumvoll, M.; et al. Sequence variants at CYP1A1- CYP1A2 and AHR associate with coffee consumption. Hum. Mol. Genet. 2011, 20, 2071–2077.
- Denden, S.; Bouden, B.; Khelil, A.H.; Ben Chibani, J.; Hamdaoui, M. Gender and ethnicity modify the association between the CYP1A2 rs762551 polymorphism and habitual coffee intake: Evidence from a meta-analysis. Genet. Mol. Res. 2016, 15.
- Happonen, P.; Voutilainen, S.; Tuomainen, T.-P.; Salonen, J.T. Catechol-O-Methyltransferase Gene Polymorphism Modifies the Effect of Coffee Intake on Incidence of Acute Coronary Events. PLoS ONE 2006, 1, e117.
- Enriquez, A.; Frankel, D.S. Arrhythmogenic effects of energy drinks. J. Cardiovasc. Electrophysiol. 2017, 28, 711–717.