Incretins are gut hormones that potentiate glucose-stimulated insulin secretion (GSIS) after meals. Glucagon-like peptide-1 (GLP-1) is the most investigated incretin hormone, synthesized mainly by L cells in the lower gut tract. GLP-1 promotes β-cell function and survival and exerts beneficial effects in different organs and tissues. Irisin, a myokine released in response to a high-fat diet and exercise, enhances GSIS. Similar to GLP-1, irisin augments insulin biosynthesis and promotes accrual of β-cell functional mass. In addition, irisin and GLP-1 share comparable pleiotropic effects and activate similar intracellular pathways. The insulinotropic and extra-pancreatic effects of GLP-1 are reduced in type 2 diabetes (T2D) patients but preserved at pharmacological doses. GLP-1 receptor agonists (GLP-1RAs) are therefore among the most widely used antidiabetes drugs, also considered for their cardiovascular benefits and ability to promote weight loss. Irisin levels are lower in T2D patients, and in diabetic and/or obese animal models irisin administration improves glycemic control and promotes weight loss. This review aims to describe the similarities between GLP-1 and irisin and to propose a new potential axis involving the gut, muscle, and endocrine pancreas that controls energy homeostasis.
- Irisin
- incretin hormones
- type 2 diabetes
- metabolic disease
1. Introduction
Incretins are gut hormones that potentiate insulin secretion after meal ingestion in a glucose-dependent manner. In particular, the “incretin effect” refers to the ability of oral glucose to elicit a greater insulin secretory response than does intravenous glucose, despite inducing similar levels of glycaemia[1]. The two best-studied incretins, glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1), exert insulinotropic actions through distinct G-protein-coupled receptors (GIP-R and GLP-1R respectively).
On the other hand, irisin is a myokine firstly described in 2012 by Boström et al.[2] as a peroxisome proliferator-activated receptor gamma coactivator 1-α (PGC1-α)-dependent myokine, secreted following physical activity and able to drive brown fat-like development of white adipose tissue and thermogenesis. Many studies have explored the pleiotropic properties of irisin, demonstrating its pivotal role in the regulation of energy metabolism, by acting on several tissues and intervening in numerous biochemical pathways. Recently, it has been proposed that irisin could exert its effects via αV integrin receptors[3]. Although skeletal muscle accounts for approximatively 72% of the total amount of irisin in the circulation[2], several studies suggest that irisin can also be produced by the pancreatic islets[4], thus emerging as a new potential intra-islet hormone.
Interestingly, irisin and GLP-1 show comparable pancreatic and pleiotropic effects and activate similar intracellular pathways.
2. Irisin and Incretin Hormones: Similarities and Differences Not to Be Underestimated
By definition, incretins are hormones with low basal plasma concentrations that are released after the ingestion of physiological nutrients to reach concentrations that augment the insulin secretory responses at a permissive degree of hyperglycaemia, although they are ineffective at low glucose concentrations[5]. According to this definition, irisin can be considered an incretin-like hormone, as its secretion appears to be also affected by meals and, once secreted, it enhances insulin secretion in a glucose-dependent manner[6]. In addition, both the GLP-1 insulinotropic effects and irisin levels are defective in T2D, and their exogenous administration is able to improve glycemic control. Importantly, irisin and GLP-1 share numerous direct pancreatic effects (Figure1a), including the ability to induce insulin biosynthesis and glucose-dependent insulin secretion, as well as improving β-cell proliferation and survival. Albeit through different pathways, irisin and GLP-1 activate the same intracellular signaling proteins (e.g., AKT, CREB, ERK1/2; Figure1b)[6][7][8].
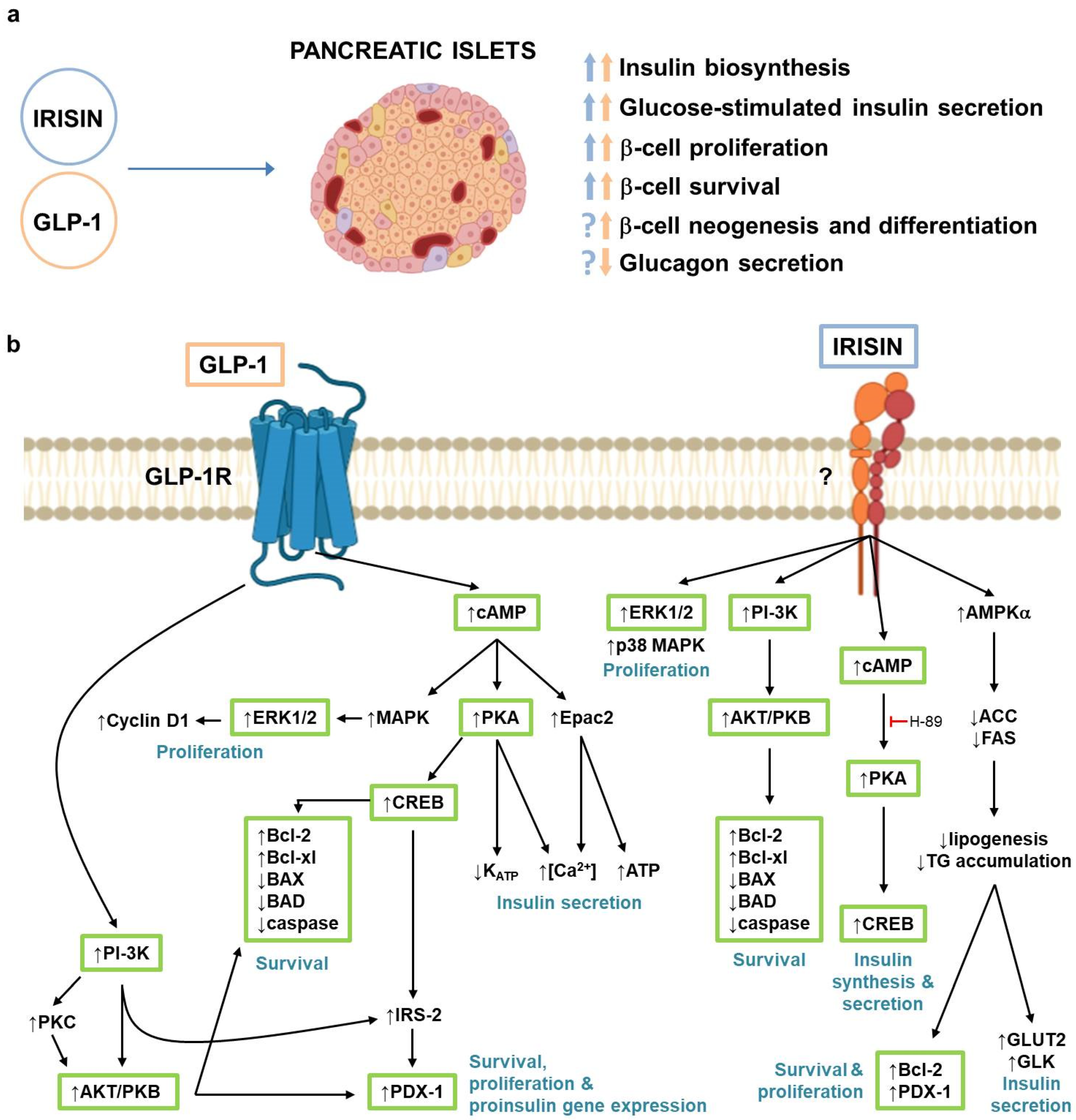
Figure 1. (a) GLP-1 and irisin effects in pancreatic islets. Blue arrows indicate irisin effects; orange arrows indicate GLP-1 effects; (b) Signaling pathways activated by GLP-1 and irisin in pancreatic β-cells. Green boxes indicate intracellular mediators activated by both GLP-1 and irisin. ACC, Acetyl-CoA carboxylase; AMPKα, adenosine monophosphate-activated protein kinase α; AKT/PKB, protein kinase B; BAD, Bcl-2 associated agonist of cell death; BAX, Bcl-2-like protein 4; Bcl-2, B-cell lymphoma-2; Bcl-xl, B-cell lymphoma-xl; cAMP, cyclic adenosine monophosphate; CREB, cAMP response element-binding protein; Epac2, exchange protein activated by cAMP 2; ERK1/2, extracellular signal-regulated kinases 1/2; FAS, GLK, glucokinase; GLP-1, glucagon-like peptide-1; GLP-1R, glucagon-like peptide-1 receptor; GLUT2, glucose transporter 2; IRS-2, insulin receptor substrate 2; MAPK, mitogen-activated protein kinase; PDX-1, pancreatic and duodenal homeobox 1; PI-3K, phospatidylinositol-3 kinase; PKA, protein kinase A; PKC, protein kinase C; TG, triglycerides.
Interestingly, irisin shows cardiovascular[9] and anorexigenic effects[10] similar to those of GLP-1, while demonstrating a more pronounced beneficial metabolic effect in insulin-dependent organs, such as liver, skeletal muscle, and adipose tissue (Figure2)[11]. Additionally, like GLP-1, irisin promotes bone formation[12]. Of note, because GLP-1 and irisin signal through different receptors that nevertheless converge on very similar pathways, an additive effect of the two molecules cannot be excluded.
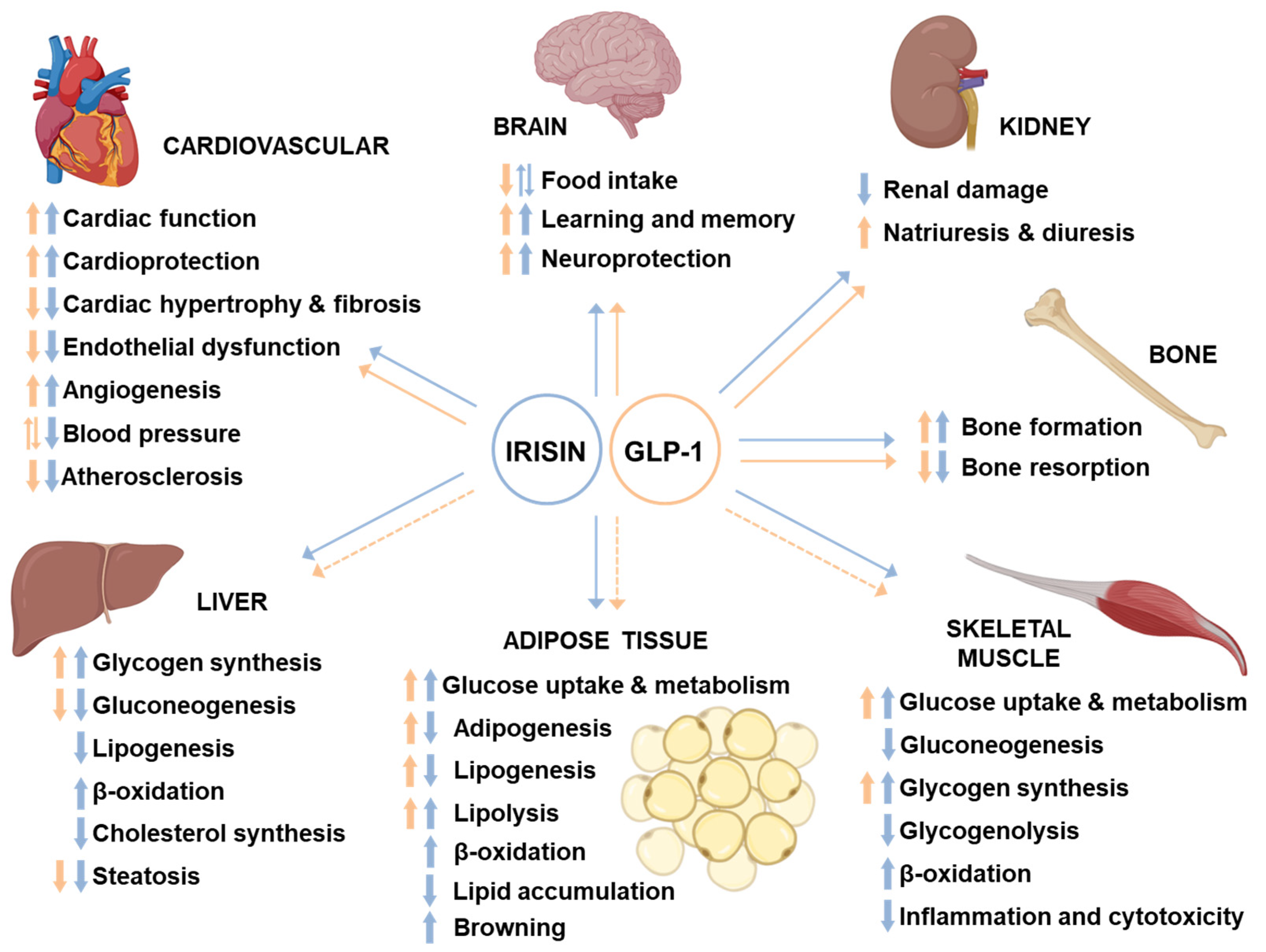
Figure 2. Pleiotropic effects of GLP-1 and irisin. Blue arrows indicate irisin effects; orange arrows indicate GLP-1 effects; dotted arrows indicate indirect effects.
3. Conclusions
In conclusion, due to its modalities of secretion and its pancreatic and extra-pancreatic effects, irisin could be considered an incretin-like hormone with an action similar to that of GLP-1, with the addition of an anabolic GIP-like effect at the bone level and a marked antilipogenic action. This evidence highlights the promising antidiabetic and antiobesity potential of irisin, possibly in combination therapeutic regimens with GLP-1RAs.
References
- Nauck, M.A.; Meier, J.J. The incretin effect in healthy individuals and those with type 2 diabetes: Physiology, pathophysiology, and response to therapeutic interventions. Lancet Diabetes Endocrinol. 2016, 4, 525–536.
- Boström, P.;Wu, J.; Jedrychowski, M.P.; Korde, A.; Ye, L.; Lo, J.C.; Rasbach, K.A.; Bostroem, E.A.; Choi, J.H.; Long, J.Z.; et al. A PGC1-alpha-dependent myokine that drives brown-fat-like development of white fat and thermogenesis. Nat. Cell Biol. 2012, 481, 463–468.
- Kim, H.; Wrann, C.D.; Jedrychowski, M.; Vidoni, S.; Kitase, Y.; Nagano, K.; Zhou, C.; Chou, J.; Parkman, V.J.A.; Novick, S.J.; et al. Irisin Mediates Effects on Bone and Fat via alphaV Integrin Receptors. Cell 2018, 175, 1756–1768.e17.
- Li, Q.; Jia, S.; Xu, L.; Li, B.; Chen, N. Metformin-induced autophagy and irisin improves INS-1 cell function and survival in high-glucose environment via AMPK/SIRT1/PGC-1alpha signal pathway. Food Sci. Nutr. 2019, 7, 1695–1703.
- Creutzfeldt, M.W. The incretin concept today. Diabetologia 1979, 16, 75–85.
- Natalicchio, A.; Marrano, N.; Biondi, G.; Spagnuolo, R.; Labarbuta, R.; Porreca, I.; Cignarelli, A.; Bugliani, M.; Marchetti, P.; Perrini, S.; et al. The Myokine Irisin Is Released in Response to Saturated Fatty Acids and Promotes Pancreatic Beta-Cell Survival and Insulin Secretion. Diabetes 2017, 66, 2849–2856.
- Liu, S.; Du, F.; Li, X.; Wang, M.; Duan, R.; Zhang, J.; Wu, Y.; Zhang, Q. Effects and underlying mechanisms of irisin on the proliferation and apoptosis of pancreatic beta-cells. PLoS ONE 2017, 12, e0175498.
- Zhang, D.; Xie, T.; Leung, P.S. Irisin Ameliorates Glucolipotoxicity-Associated Beta-Cell Dysfunction and Apoptosis via AMPK Signaling and Anti-Inflammatory Actions. Cell. Physiol. Biochem. 2018, 51, 924–937.
- Li, J.; Xie, S.; Guo, L.; Jiang, J.; Chen, H. Irisin: linking metabolism with heart failure. Am J Transl Res. 2020 Oct 15;12(10):6003-6014.
- Natalicchio, A.; Marrano, N.; Biondi, G.; DiPaola, L.; Spagnuolo, R.; Cignarelli, A.; Perrini, S.; Laviola, L.; Giorgino, F. Irisin increases the expression of anorexigenic and neurotrophic genes in mouse brain. Diabetes Metab. Res. Rev. 2019, 36.
- Polyzos, S.A.; Anastasilakis, A.D.; Efstathiadou, Z.A.; Makras, P.; Perakakis, N.; Kountouras, J.; Mantzoros, C.S. Irisin in metabolic diseases. Endocrine. 2018 Feb;59(2):260-274.
- Briganti, S.I.; Gaspa, G.; Tabacco, G.; Naciu, A.M.; Cesareo, R.; Manfrini, S.; Palermo, A. Irisin as a regulator of bone and glucose metabolism. Minerva Endocrinol. 2018 Dec;43(4):489-500.