Mutations that occur within the AMPD1 gene are one of the most common defects detected in the Caucasian population with a likelihood of having the mutations as 1-2%. Several studies indicate that certain variants can cause fatigue, muscle weakness and muscular cramps, however some even with these variants remain asymptomatic. Some studies have shown that oral dosages of ribose can alleviate symptoms and can improve exercise performance in those with AMPD1 deficiency, ribose may provide a direct source of energy for cells. The aim of this preliminary study was to see if oral supplementary ribose can improve the performance of a 3 minute press-up test that is aimed to test muscle stamina and muscle fatigue in healthy Caucasian males against a control of healthy Caucasian males. The results show that having a T in rs17602729 may affect press-up performance in a 3 minute test and that supplemental ribose may improve performance, however the following results need to be correlated with current literature in the area and the conclusions are still debatable.
- AMPD1
- Muhdo
- DNA
- ribose
- D-ribose
- nutrition
- genetics
- exercise performance
1. Introduction
*This is a preliminary search for correlations to allow for further study.
Introduction
Adenosine monophosphate deaminase 1 (AMPD1) plays a vital role in the purine nucleotide cycle, the gene encodes an enzyme of the same name. The enzyme coverts adenosine monophosphate to inosine monophosphate which frees an ammonia molecule during the process. Mutations that occur within the AMPD1 gene are one of the most common defects detected in the Caucasian population with a likelihood of having the mutations as 1-2%
[1]
. Several studies indicate that certain variants can cause fatigue, muscle weakness and muscular cramps
[2]
[3]
, however some even with these variants remain asymptomatic.
The disorder caused by mutations is known as adenosine monophosphate deaminase deficiency type 1 (AMPD1 deficiency) or myoadenylate deaminase deficiency (MADD). The most common symptoms of AMPD1 deficiency are:
- Exercise intolerance – symptoms of fatigue and fast onset weakness on the commencement of exertion or prolonged exertion.
- Fatigue – general fatigue is poorly understood and may have multiple pathways, however a surplus of adenosine reduces alertness [4].
- Muscle cramping – this is may be due to an increased lactate [5].
Those who have AMPD1 deficiency should maintain fitness levels for general health but also maintain the strength of muscles to keep proper function. Some studies have shown that oral dosages of ribose can alleviate symptoms and can improve exercise performance in those with AMPD1 deficiency, ribose may provide a direct source of energy for cells
[6].
.
Aim & Methods
*This is a e aim of this preliminary search for correlatitudy was to see if oral supplementary ribose can improve the performance of a 3 minute press-up test that is aimed to test muscle stamina and muscle fatigue in healthy Caucasian males (n= 55, 28-35y/o) agains to allt a control of healthy Caucasian males (n=14, 28-35y/o) w for further studyhilst analysing the variants in rs17602729 (AMPD1). Two press-up tests done a week apart were conducted with participants taking 10g of oral ribose daily split into 2 5g doses, before the second press-up test 10g as the single dosage of that day was taken 30minutes prior to the test. The control group participants had no supplementary nutrition.
2. Aim & Methods
Results
The aim of this preliminary study was to see if oral supplementary ribose can improve the performance of a 3 minute press-up test that is aimed to test muscle stamina and muscle fatigue in healthy Caucasian males (n= 55, 28-35y/o) against a control of healthy Caucasian males (n=14, 28-35y/o) whilst analysing the variants in rs17602729 (AMPD1). Two press-up tests done a week apart were conducted with participants taking 10g of oral ribose daily split into 2 5g doses, before the second press-up test 10g as the single dosage of that day was taken 30minutes prior to the test. The control group participants had no supplementary nutrition.
The results show that 24 in the non-control group and 4 in the control group had CC (fwd/fwd) in rs17602729, 15 in the non-control group and 5 in the control group had CT (fwd/fwd) in rs17602729, 15 in the non-control group and 5 in the control group had TT (fwd/fwd) in rs17602729. The pre-test press-up and post-test press-up results are in the tables below:
The results show that 24 in the non-control group and 4 in the control group had CC (fwd/fwd) in rs17602729, 15 in the non-control group and 5 in the control group had CT (fwd/fwd) in rs17602729, 15 in the non-control group and 5 in the control group had TT (fwd/fwd) in rs17602729. The pre-test press-up and post-test press-up results are in the tables below:
|
Press-up max in 3 minutes pre |
Press-up max in 3 minutes post 7 day rest + D-ribose |
|
|
CC |
72 |
73 |
|
CC |
91 |
91 |
|
CC |
88 |
86 |
|
CC |
75 |
78 |
|
CC |
79 |
82 |
|
CC |
101 |
99 |
|
CC |
88 |
92 |
|
CC |
110 |
108 |
|
CC |
92 |
83 |
|
CC |
94 |
96 |
|
CC |
96 |
98 |
|
CC |
88 |
90 |
|
CC |
73 |
75 |
|
CC |
80 |
79 |
|
CC |
91 |
89 |
|
CC |
87 |
90 |
|
CC |
94 |
100 |
|
CC |
99 |
101 |
|
CC |
101 |
105 |
|
CC |
110 |
101 |
|
CC |
62 |
72 |
|
CC |
73 |
75 |
|
CC |
90 |
88 |
|
CC |
91 |
93 |
|
CT |
100 |
101 |
|
CT |
98 |
105 |
|
CT |
88 |
92 |
|
CT |
85 |
91 |
|
CT |
93 |
96 |
|
CT |
95 |
95 |
|
CT |
92 |
101 |
|
CT |
100 |
103 |
|
CT |
75 |
78 |
|
CT |
62 |
71 |
|
CT |
90 |
93 |
|
CT |
82 |
84 |
|
CT |
68 |
72 |
|
CT |
72 |
78 |
|
CT |
69 |
78 |
|
TT |
89 |
98 |
|
TT |
71 |
89 |
|
TT |
65 |
75 |
|
TT |
58 |
69 |
|
TT |
71 |
79 |
|
TT |
69 |
72 |
|
TT |
70 |
70 |
|
TT |
81 |
92 |
|
TT |
83 |
92 |
|
TT |
71 |
84 |
|
TT |
74 |
80 |
|
TT |
72 |
75 |
|
TT |
79 |
88 |
|
TT |
68 |
75 |
|
TT |
63 |
79 |
|
rs17602729 fwd/fwd D-Ribose group |
Press-up max in 3 minutes pre |
Press-up max in 3 minutes post 7 day rest + D-ribose |
|
CC |
72 |
73 |
|
CC |
91 |
91 |
|
CC |
88 |
86 |
|
CC |
75 |
78 |
|
CC |
79 |
82 |
|
CC |
101 |
99 |
|
CC |
88 |
92 |
|
CC |
110 |
108 |
|
CC |
92 |
83 |
|
CC |
94 |
96 |
|
CC |
96 |
98 |
|
CC |
88 |
90 |
|
CC |
73 |
75 |
|
CC |
80 |
79 |
|
CC |
91 |
89 |
|
CC |
87 |
90 |
|
CC |
94 |
100 |
|
CC |
99 |
101 |
|
CC |
101 |
105 |
|
CC |
110 |
101 |
|
CC |
62 |
72 |
|
CC |
73 |
75 |
|
CC |
90 |
88 |
|
CC |
91 |
93 |
|
CT |
100 |
101 |
|
CT |
98 |
105 |
|
CT |
88 |
92 |
|
CT |
85 |
91 |
|
CT |
93 |
96 |
|
CT |
95 |
95 |
|
CT |
92 |
101 |
|
CT |
100 |
103 |
|
CT |
75 |
78 |
|
CT |
62 |
71 |
|
CT |
90 |
93 |
|
CT |
82 |
84 |
|
CT |
68 |
72 |
|
CT |
72 |
78 |
|
CT |
69 |
78 |
|
TT |
89 |
98 |
|
TT |
71 |
89 |
|
TT |
65 |
75 |
|
TT |
58 |
69 |
|
TT |
71 |
79 |
|
TT |
69 |
72 |
|
TT |
70 |
70 |
|
TT |
81 |
92 |
|
TT |
83 |
92 |
|
TT |
71 |
84 |
|
TT |
74 |
80 |
|
TT |
72 |
75 |
|
TT |
79 |
88 |
|
TT |
68 |
75 |
|
TT |
63 |
79 |
|
rs17602729 fwd/fwd D-Ribose group |
Table 1. Non-control group results.
Table 1. Non-control group results.
|
rs17602729 fwd/fwd control |
Press-up max in 3 minutes pre |
Press-up max in 3 minutes post 7 day rest |
|
CC |
88 |
89 |
|
CC |
89 |
88 |
|
CC |
91 |
90 |
|
CC |
74 |
74 |
|
CT |
78 |
77 |
|
CT |
88 |
86 |
|
CT |
86 |
89 |
|
CT |
84 |
85 |
|
CT |
71 |
73 |
|
TT |
68 |
70 |
|
TT |
73 |
70 |
|
TT |
82 |
81 |
|
TT |
71 |
70 |
|
TT |
67 |
66 |
|
rs17602729 fwd/fwd control |
Press-up max in 3 minutes pre |
Press-up max in 3 minutes post 7 day rest |
|
CC |
88 |
89 |
|
CC |
89 |
88 |
|
CC |
91 |
90 |
|
CC |
74 |
74 |
|
CT |
78 |
77 |
|
CT |
88 |
86 |
|
CT |
86 |
89 |
|
CT |
84 |
85 |
|
CT |
71 |
73 |
|
TT |
68 |
70 |
|
TT |
73 |
70 |
|
TT |
82 |
81 |
|
TT |
71 |
70 |
|
TT |
67 |
66 |
Table 2. Control group results.
Table 2. Control group results.
|
Average |
pre |
post |
|
rs17602729 CC |
88.5 |
89.3 |
|
rs17602729 CT |
84.6 |
89.2 |
|
rs17602729 TT |
72.2 |
81.1 |
|
rs17602729 CONTROL CC |
85.5 |
85.25 |
|
rs17602729 CONTROL CT |
81.4 |
82 |
|
rs17602729 CONTROL TT |
72.4 |
71.4 |
|
Average |
pre |
post |
|
rs17602729 CC |
88.5 |
89.3 |
|
rs17602729 CT |
84.6 |
89.2 |
|
rs17602729 TT |
72.2 |
81.1 |
|
rs17602729 CONTROL CC |
85.5 |
85.25 |
|
rs17602729 CONTROL CT |
81.4 |
82 |
|
rs17602729 CONTROL TT |
72.4 |
71.4 |
Table 3. Average results.
Table 3. Average results.
From the results we can see that in all 3 outcome control groups there was no significant change in press-up results. Within the d-ribose group that had CC there was no significant difference is scores, within the CT group there was a difference of + 4 press-ups on average however the significance of this is debatable, for the TT group there was a difference of +9 reps which is a significant difference which is unlikely to come down to placebo affect alone.
From the results we can see that in all 3 outcome control groups there was no significant change in press-up results. Within the d-ribose group that had CC there was no significant difference is scores, within the CT group there was a difference of + 4 press-ups on average however the significance of this is debatable, for the TT group there was a difference of +9 reps which is a significant difference which is unlikely to come down to placebo affect alone.
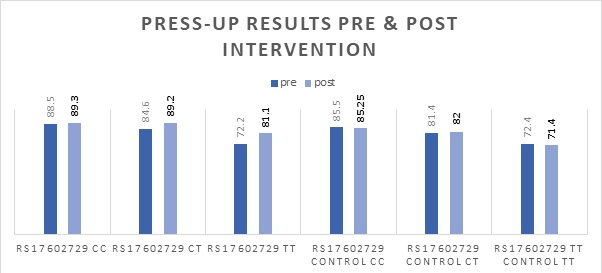
Graph 1. Average results.
Conclusion
The results show that having a T in rs17602729 may affect press-up performance in a 3 minute test and that supplemental ribose may improve performance, however the following results need to be correlated with current literature in the area, with further analysis including larger subject numbers. Whilst there is a significant difference between groups the exact cause is debatable with other factors requiring consideration.
References
- Adenosine monophosphate deaminase deficiency . Genetics Home Reference. Retrieved 2020-5-7
- Christopher Collins; Resistance Training, Recovery and Genetics: AMPD1 the Gene for Recovery. Journal of Athletic Enhancement 2017, 6, 1, 10.4172/2324-9080.1000256.
- Xinhui Li; Carsten Bantel; Dawn Conklin; Steven R. Childers; James C. Eisenach; Repeated dosing with oral allosteric modulator of adenosine A1 receptor produces tolerance in rats with neuropathic pain.. Anesthesiology 2004, 100, 956-961, 10.1097/00000542-200404000-00028.
- Hiroko Morisaki; Takayuki Morisaki; [AMPD genes and urate metabolism].. Nihon rinsho. Japanese journal of clinical medicine 2008, 66, 771-7.
- Ronnie Blazev; Graham D. Lamb; Adenosine inhibits depolarization-induced Ca(2+) release in mammalian skeletal muscle.. Muscle & Nerve 1999, 22, 1674-1683, 10.1002/(sici)1097-4598(199912)22:12<1674::aid-mus9>3.0.co;2-0.
- N Zöllner; S Reiter; M Gross; D Pongratz; C D Reimers; K Gerbitz; I Paetzke; T Deufel; G Hübner; Myoadenylate deaminase deficiency: successful symptomatic therapy by high dose oral administration of ribose.. Klinische Wochenschrift 1986, 64, 1281-91.