Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 2 by Lily Guo and Version 1 by Chien-Chin Chen.
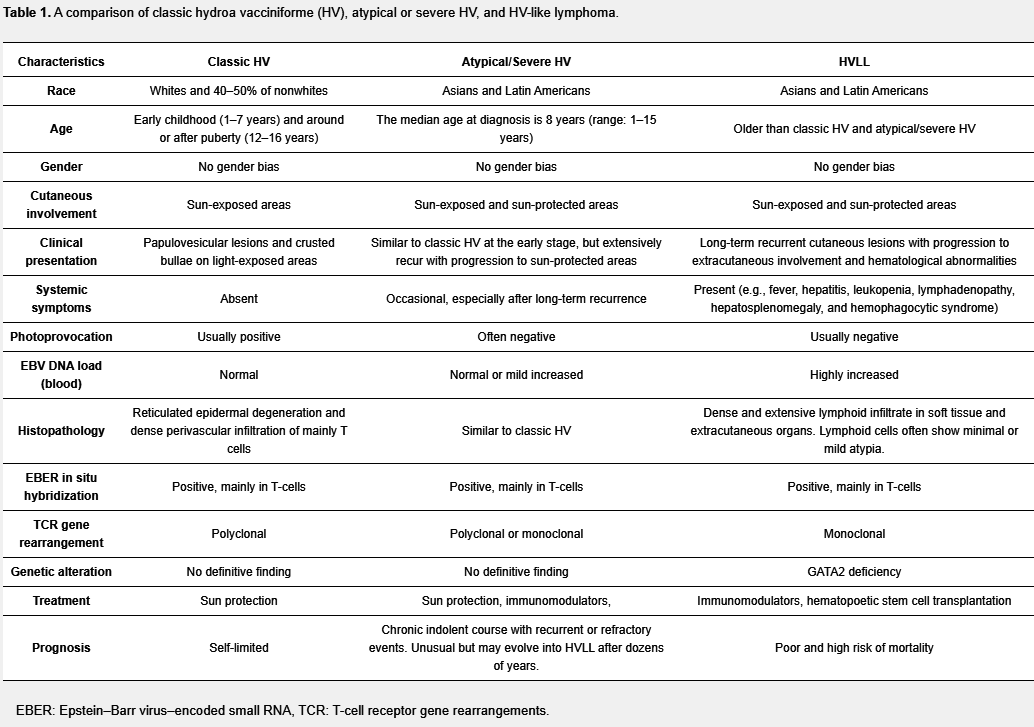
Hydroa vacciniforme (HV) is a rare form of photosensitivity disorder in children or adolescence and is frequently associated with Epstein–Barr virus (EBV) infection, whereas HV-like lymphoproliferative disorders (HVLPD) describe a spectrum of EBV-associated T-cell or natural killer (NK)-cell lymphoproliferations with HV-like cutaneous manifestations, including EBV-positive HV, atypical HV, and HV-like lymphoma.
- Hydroa Vacciniforme
- Epstein-Barr Virus
- Skin
- Lymphoma
- Photosensitive
- Dermatology
- Sunlight
1. Introduction
1.1. Hydroa Vacciniforme
Hydroa vacciniforme (HV), first described in 1862, is a rare idiopathic photosensitive cutaneous disorder [1]. Photodermatoses are a heterogeneous group of cutaneous disorders involving abnormal reactions to sunlight, usually caused or aggravated by ultraviolet (UV) components [2,3]. Initially, HV was believed to be a photodermatosis, intermediate in severity between hydroa aestivale and xeroderma pigmentosum [4]. Currently, HV is classified within the group of immunologically mediated (idiopathic) photodermatoses [2]. The prevalence of HV is 0.5 cases per 100,000 people in the Scottish population [5]. In the United States, HV constitutes 0.37% of all patients with photodermatoses and is more prevalent in non-white, non-black patients [6]. In most cases, HV occurs in childhood with a bimodal distribution of early childhood (1–7 years old) and around or after puberty (12–16 years old) [7]. Classically, HV is characterized by chronic recurrent papulovesicles or vesiculobullous eruptions on sun-exposed areas after sunlight exposure, and is usually self-limited in adolescents or young adults. Patients may be sensitive to one kind of sunlight or to a wider range of wavelengths. Some studies suggest that UVB is the causal agent [4], whereas other studies report that longer wavelengths in the UVA spectrum are the more likely cause [7,8]. HV is seasonal and occurs typically in the summer.
1.2. Hydroa Vacciniforme-Like Lymphoproliferative Disorders
Patients with atypical or severe HV can present with eruptions similarly to those of patients with classic HV in the early phase of the disease, but recurrent cutaneous eruptions become more severe with age, progressing to involve both sun-protected and sun-exposed areas with facial swelling, ulcers, scarring, fever, hepatitis, hematologic abnormalities, and lymphadenopathy [9]. After a protracted clinical course with many recurrences, a subset of patients with atypical or severe HV may develop a systemic and often fatal EBV-positive T cell or NK cell lymphoma, although development of lymphoma is uncommon [10]. Regarding this phenomenon, the 2008 edition of the World Health Organization (WHO) classification of hematopoietic and lymphoid tumors described the HV-like lymphoma (HVLL) mostly carrying clonal rearrangements of the T-cell receptor (TCR) genes and monoclonal Epstein–Barr virus (EBV) [11]. However, because of the inability to predict which patients will behave in an indolent fashion versus those patients who will develop overt lymphoma, the new designation hydroa vacciniforme-like lymphoproliferative disorder (HVLPD) was established in the 2016 edition of the WHO classification [12,13]. This term encompasses chronic HV-like EBV-positive lymphoproliferative disorders of childhood with an increased risk of developing systemic lymphoma. By definition, HVLPD should include EBV-positive HV subtypes, particularly atypical or severe HV cases, and HVLL with a broad spectrum of clinical severity and a long disease course. HVLPD occurs mainly in children in Asia and Latin America without a significant sex bias [14], and the median age at diagnosis is 8 years (range: 1–15 years) [13].
In the early phase of the disease, patients with HVLPD present with cutaneous disorders involving sun-exposed areas characterized by chronic papulovesicular skin lesions, ulcers, and scarring with an indolent behavior, similar to classic HV. However, some patients experience a long course of recurrences with disease extending to sun-protected skin areas, and progressing to systemic manifestations, including fever, hepatitis, lymphadenopathy, hepatosplenomegaly, and hemophagocytic syndrome [10,15,16]. Non-white patients with HVLPD are more likely to develop systemic disease than white patients [17]. Moreover, HVLPD may persist for dozens of years and over time about 15% of patients with HVLPD will develop HVLL with a higher mortality rate [10,18,19,20]. HVLL is predominantly reported in Latin America (Peru, Mexico, and Guatemala) and Asia (Korea, Japan, and Taiwan), and rarely occurs in whites [17,21]. In Taiwan, Lee et al. reported that HVLL constitutes 1% of all primary cutaneous lymphomas [22].
2. Pathological Features and Immunochemical Profiles
Histopathological features of HV can vary according to clinical stage and the severity of different lesions. In early stages of HV, characteristic histologic features in the skin include intraepidermal spongiotic vesiculation, varying degrees of lymphocytic infiltrate in the upper dermis (Figure 2) and areas of keratinocyte necrosis [7,10]. A histologic hallmark of HV, suggested by Iwatsuki et al., is a dense perivascular lymphocytic infiltration with reticulated degeneration of the epidermis [9]. The histologic features of classic HV and atypical/severe HV are essentially indistinguishable, such as reticulated epidermal degeneration and dense perivascular infiltration of mainly T cells, although the lymphoid infiltrate is often more dense and extensive, and extends deeply into subcutaneous tissue in atypical/severe HV [9]. Moreover, the clinical manifestations often deviate from the pathological features. Even with clinical features of aggressive disease or systemic involvement, lymphoid cells often show minimal or mild atypia (Figure1) [44,45,46]. Thus, the diagnosis of HV versus HVLPD relies greatly on a careful history, physical examination, and phototesting, whereas histopathologic examination and laboratory tests are helpful in ruling out other photodermatoses.
Notably, in situ hybridization for EBER in skin biopsy specimens shows positive cells in over 95% of patients with classic HV and atypical/severe HV [9] and 100% patients with HVLPD [19]. Immunohistochemically, expression of CD5, CD7, CD43, and CD25 is variable, whereas CD57 is negative [37]. The lymphoid infiltrate is composed most frequently of cytotoxic CD8+ T cells, but in one-third of cases the infiltrate is derived from CD56+ NK cells [46]. The T cells can be positive for either T-cell receptor αβ or γδ. The Ki-67 index is variable, and can be very low or as high as 50% [37].
Monoclonal rearrangement of TRG and/or TRB is regarded as a useful tool for distinguishing classic HV from severe HV [29]. In a large cohort study of HVLPD, 88% of patients carried monoclonal T-cell receptor gene rearrangements [19]. Xie et al. further recommended that clonal rearrangements of the T-cell receptor genes is a prognostic indicator. In their study all patients with monoclonal T-cell receptor gene rearrangements died [45]. In our previous study, all classic HV patients showed no evidence of a monoclonal T-cell population in the initial skin specimens [10]. Thus, T-cell monoclonality would be unusual in classic HV and might be an important clue to herald progression to atypical HV or HVLL, especially combined with an atypical or aggressive clinical presentation [10,20]. Notably, a subset of HV-like eruptions is one of the clinical manifestations of chronic active EBV infection (CAEBV), and clinicopathologic survey with fulfillment of diagnostic criteria is the key to reach the diagnosis of CAEBV [13]. Direct immunofluorescence is usually nonspecific, although there are a few reports describing granular deposition of C3 below the basement membrane and in the dermal papillae [8,42].

Figure1. Clinical and pathologic features of a patient with HVLPD and development of HVLL. (A,B) The patient was a 31-year-old man who presented recurrent vesicles and papules on the face, hands and legs for 17 years. The cutaneous lesions extended to sun-protected areas, including upper arms and feet. (C) This patient had intermittent fevers, pancytopenia, and palpable neck lymph nodes, and the abdominal computerized tomography (CT) scan with contrast enhancement showed splenomegaly. (D) In the skin biopsy specimen, double staining of CD3 and EBER in situ hybridization proved EBV infection in many T cells (green arrows, 400×). Scale bar = 50 μM.
3. Molecular and Genetic Characteristics
Given the rare occurrence of HVLPDs, the reports regarding molecular and genetic features of these lesions are limited. Since Zhang et al. reported chromosome 6q deletion in a cell line (SNK-11) from a patient with HV [47], some genomic breakthroughs have been explored. In 2016, Cohen et al. reported that GATA2 deficiency is associated with EBV-positive HVLL [48]. GATA2 is a transcription factor crucial for both cellular immune responses and controlling the latent infection of herpesviruses, and is expressed in hematopoietic progenitors. Because one of GATA2 binding sites in EBV is located in a latency promoter, the Cp promoter for EBNA latency proteins, insufficiency of GATA2 may impair virus latency and result in more viral replication with prolonged active EBV infection and low numbers of monocytes, CD4 T cells, B cells, and NK cells [48]. To date, only one 24-year-old Cantonese woman with HVLL was proven to have GATA2 deficiency and was successfully treated with a haplo-identical hematopoietic cell transplant from her unaffected sister [48]. Except the aforementioned case, Cohen et al. found no mutations in GATA2 or other genes associated with severe EBV disease or repair of DNA in HVLPD patients [17].
Cohen and colleagues performed RNAseq analysis on a skin specimen of one patient with HVLPD. Compared with normal control tissue, skin of HVLPD revealed upregulation of genes encoding multiple chemokines [17], with the most upregulated genes being CXCL11, CXCL9, CXCL10, and CCL4. These genes encode chemoattractants for activated T cells, activated monocytes, and NK cells. Other upregulated genes include IFNG, which encodes interferon γ to inhibit EBV outgrowth, and APOBEC3A, which encodes a member of the cytidine deaminase family to suppress replication of cytomegalovirus [17].
Moreover, Cohen et al. conducted a whole-exome sequencing study on a Caucasian patient with HVLPD and did not identify any pathogenic variants [17]. However, by performing a whole-exome sequencing study in five Chinese patients with HVLPD, Xie et al. reported eight mutant genes that might correlate with development of HVLPD [45]. The eight mutant genes include five driver mutations involving STAT3, IKBKB, ELF3, CHD7, and KMT2D, as well as three passenger mutations involving ELK1, RARB, and HPGDS. All of these mutant genes and their downstream signaling pathways have been shown to be pathogenic factors in lymphoproliferative diseases [45]. The occurrence of these mutant genes and the potential mechanisms employed by these genes in HVLPD warrants further study.
4. Treatment and Therapeutic Agents
Traditionally, HV is treated conservatively, since classic HV usually undergoes spontaneous remission before adulthood. The therapeutic strategies consist of broad-spectrum sunscreens with a high sun protection factor and avoidance of sunlight exposure [7,28,40]. In patients who do not respond to conservative treatment or have a prolonged refractory course, dermatologists should consider the possibility of HVLPD, particularly atypical/severe HV or HVLL. Currently, there are no guidelines to treat patients with HVLPD, mostly owing to the rarity of the disease. Several regimens, including phototherapy [41], immunomodulatory agents (antiviral agents, interferon, thalidomide, hydroxychloroquine, intravenous immunoglobulin, etc.) [17,19,49,50,51,52], systemic corticosteroids [17,19], chemotherapy [19,53], and hematopoietic stem cell transplantation [19,53] have been used with variable rates of success. Regarding phototherapy, narrowband UVB (NBUVB) phototherapy three times weekly for five weeks is most often recommended [41], whereas psoralen-UVA (PUVA) photochemotherapy is not recommended for younger patients. In a report of 41 cases with HVLPD, Liu et al. suggested conservative treatment for most Chinese patients with HVLPD, and that chemotherapy should not be used as a first-line treatment [19]. Similarly, studies from Latin American nations have reported poor outcomes in patients receiving chemotherapy [54]. If chemotherapy fails to eradicate lymphoma cells, this therapy may worsen the prognosis by inducing immunosuppression and reactivating EBV replication. Among a variety of therapeutic modalities, immunomodulatory therapy for HVLPD is often recommended [37]. Immunomodulator agents can modulate the host inflammatory response by enhancing innate immunity against viral replication, and can suppress disease aggressiveness.