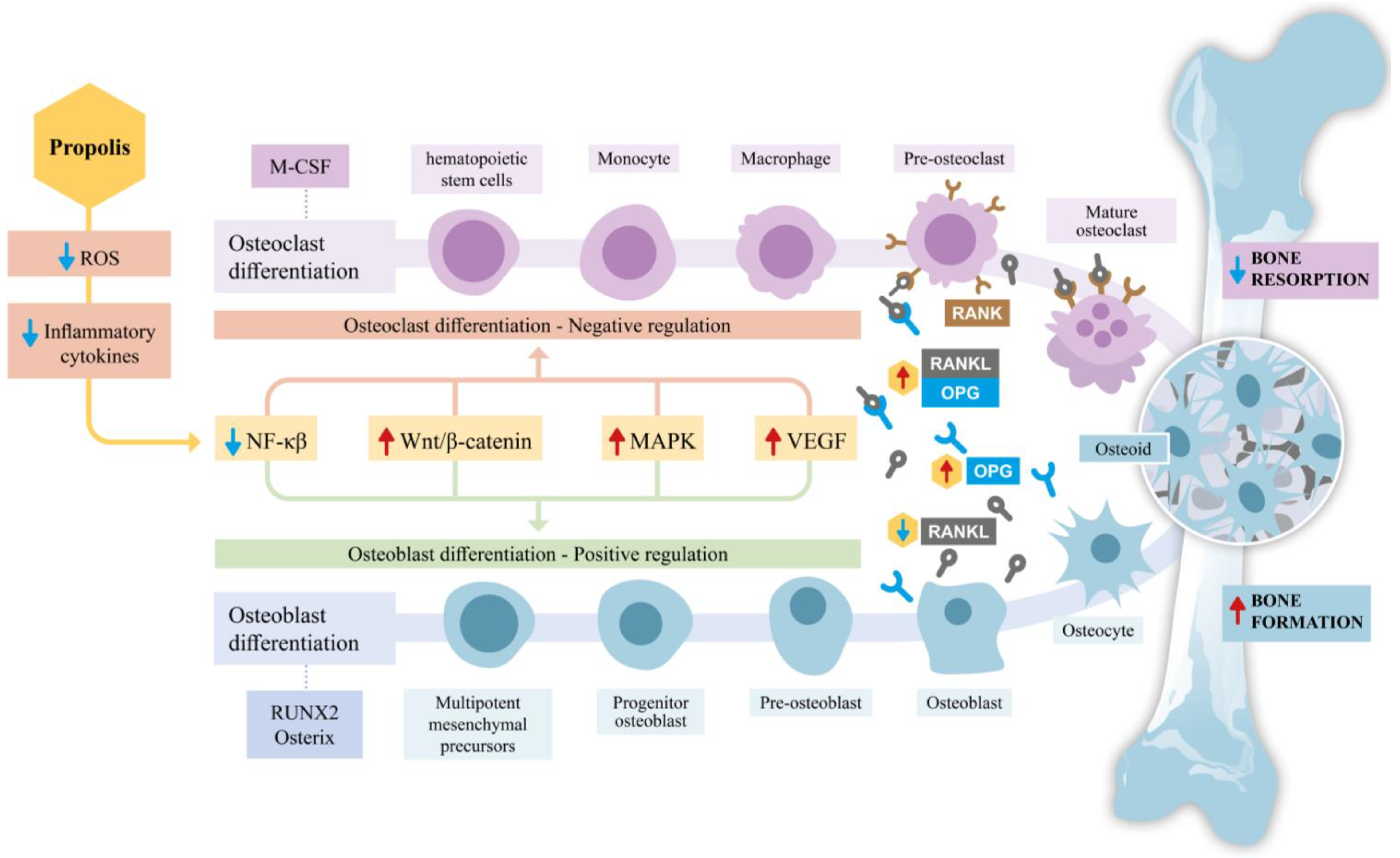
Propolis bioactive compounds in bone homeostasis comprise a diverse set of flavonoids, phenolic acids, and related polyphenols that act on the coupled processes of bone formation and resorption through antioxidant, anti‑inflammatory, and signaling‑modulatory mechanisms. By targeting key pathways such as RANKL/RANK/OPG, NF‑κB, Wnt/β‑catenin, MAPK, and the NRF2/KEAP1/HO‑1 axis, these compounds promote osteoblast differentiation and mineralization while inhibiting osteoclastogenesis, thereby counteracting oxidative and inflammatory drivers of bone loss in conditions like postmenopausal osteoporosis, glucocorticoid exposure, and diabetes‑related bone disease.
Chemogeographic variation (e.g., Brazilian green and red, European poplar‑type, Chinese and Pacific propolis) shapes distinct bioactive fingerprints enriched in CAPE, quercetin, kaempferol, apigenin, pinocembrin, and phenolic acids, each contributing complementary osteoanabolic and antiresorptive effects supported by in vitro and in vivo models. Despite robust preclinical evidence for improved bone microarchitecture, mineral density, and repair, clinical translation is still limited by heterogeneous composition, bioavailability constraints, and the absence of standardized, multi‑center randomized trials; future work should integrate untargeted LC‑MS/MS metabolomics, optimized delivery systems, and sex‑stratified clinical studies in high‑risk populations to clarify therapeutic value and positioning alongside established osteoporosis therapies.
- bioactive compounds
- bone homeostasis
- osteogenesis
- osteoclastogenesis
- antioxidant
- osteoporosis
- flavonoids
- propolis
- Oxidative Stress and Bone
- RANKL/RANK/OPG System
This entry is adapted from the peer-reviewed paper https://doi.org/10.3390/antiox14010081
Pr1. Compolis Bioactive Compounds in Bone Homeostasis
Defsition and Chemogeographic Variniation
Propolis bioactive compounds in bone homeostasis refers to the pharmacological and molecular actions of propolis-derived polyphenols, flavonoids, and phenolic acids on the cellular and signaling mechanisms that regulate bone formation (osteoblastogenesis) and bone resorption (osteoclastogenesis). Propolis is a resinous substance produced by honeybees (Apis mellifera) from plant exudates and is characterized by its antimicrobial, anti-inflammatory, and antioxidant properties. Its bioactive composition varies according to geographic origin and botanical source, yet converges on a conserved capacity to modulate the RANKL/RANK/OPG axis, NF-κB signaling, Wnt/β-catenin pathway, and reactive oxygen species (ROS) balance — all central to bone homeostasis [1][2].
1. Composition and Chemogeographic Variation
Propolis contains hundreds of constituents, including flavonoid aglycones, phenolic acids, terpenoids, aromatic esters, amino acids, and trace elements (Mg, Ca, Zn, Fe). The chemogeographic profile determines which bioactive compounds predominate and directly shapes its osteogenic potential:[2]
|
Region / Type |
Botanical Source |
Characteristic Compounds |
Bone-Relevant Activity |
|
Brazilian Green |
Baccharis dracunculifolia |
Artepillin C, p-Coumaric acid, Ferulic acid |
OPG upregulation, growth plate stimulation[1][2] |
|
Brazilian Red |
Dalbergia ecastophyllum |
Formononetin, isoflavones |
Estrogen-like osteogenic signaling[1][2] |
|
European / Temperate |
Populus spp. |
CAPE, Caffeic acid, Quercetin, Pinocembrin |
NF-κB inhibition, RUNX2 upregulation[2] |
|
Chinese |
Populus spp. |
Pinocembrin, Chrysin, Galangin |
Anti-inflammatory, ROS scavenging[2] |
|
Pacific (Japan/Taiwan) |
Macaranga tanarius |
Prenylated flavanones |
Antioxidant, anti-resorptive[1] |
Advanced analytical methods — including HPLC-DAD, UHPLC-QqQ-MS/MS, LC-ESI-MS/MS, and QTOF-MS — enable high-resolution identification and quantification of these compounds, supporting both chemogeographic characterization and pharmacological investigation.[1][2]
2. Mechanisms of Action on Bone Cells
2.1. Anabolic Effects on Osteoblasts
Propolis extracts and isolated compounds stimulate osteoblast differentiation and mineralization through multiple convergent pathways. Key osteoblastogenic effects include:[1][2]
- Upregulation of RUNX2 and Osterix — transcription factors essential for mesenchymal stem cell commitment to the osteoblast lineage
- Increased alkaline phosphatase (ALP) activity — a functional marker of osteoblast maturation and bone matrix mineralization
- Wnt/β-catenin activation — β-catenin stabilization promotes osteoprogenitor differentiation and inhibits osteoblast apoptosis
- Growth factor upregulation — FGF-2 and VEGF expression is enhanced, supporting the osteogenesis–angiogenesis coupling critical for bone repair
- MAPK/ERK and JNK activation — ERK cascade stimulation facilitates osteoblast proliferation and differentiation in response to growth factors
2.2. Anticatabolic Effects on Osteoclasts
Propolis exerts potent anti-osteoclastogenic effects, reducing bone resorption through:
- UpregRANKL/RANK/OPG modulation of RUNX2 and Osterix — tincranscription factors essential for mesenchymal stem cell commitment to theeased OPG expression competitively inhibits RANKL binding to RANK, suppressing osteoblast lineageclast precursor differentiation[1]
- IncreasedNF-κB alkaline phosphatase (ALP) activitypathway suppression — inhibition of TNF-α– a functional marker of osteoblast maturation and bone matrix mineralizationd IL-1β–induced NF-κB activation reduces NFATc1 expression, a master transcription factor for osteoclastogenesis[1]
- WntNRF2/KEAP1/β-cateninHO-1 axis activation — β-cupregulatenin stabilization promotesion of antioxidant enzyme HO-1 attenuates ROS-driven osteoprogenitorclast differentiation and inhibits osteoblast apoptosi; NRF2 also negatively regulates NFATc1 and is thus a key target in estrogen-deficiency bone loss[1][2]
- GProwth factor upregula-inflammatory cytokine reduction — decreased IL-6, IL-12, TNFGF-2 and VEGF expression is enhanced, supporting the osteogenesis–angiogenesis coupling critical for bone repair-α, IFN-γ, GM-CSF and IL-1β; increased regulatory cytokines IL-4, IL-10, and TGF-β[1]
- MAPK/ERKCOX-2 and JNK activaprostaglandin E2 inhibition — ERK cascade stmimulation facilitattigates osteoblast proliferation and differentiation in response clast-promoting inflammatory microenvironmento growth factors[1][2]
2.2 Anticatabolic Effects on Osteoclasts
Propolis exerts potent anti-osteoclastogenic effects, reducing bone resorption through:
- RANKL/RANK/OPG modulation — increased OPG expression competitively inhibits RANKL binding to RANK, suppressing osteoclast precursor differentiation[1]
- NF-κB pathway suppression — inhibition of TNF-α– and IL-1β–induced NF-κB activation reduces NFATc1 expression, a master transcription factor for osteoclastogenesis[1]
- NRF2/KEAP1/HO-1 axis activation — upregulation of antioxidant enzyme HO-1 attenuates ROS-driven osteoclast differentiation; NRF2 also negatively regulates NFATc1 and is thus a key target in estrogen-deficiency bone loss[1][2]
- Pro-inflammatory cytokine reduction — decreased IL-6, IL-12, TNF-α, IFN-γ, GM-CSF and IL-1β; increased regulatory cytokines IL-4, IL-10, and TGF-β[1]
- COX-2 and prostaglandin E2 inhibition — mitigates osteoclast-promoting inflammatory microenvironment[1][2]
2.3. Oxidative Stress and Bone Homeostasis
Chronic oxidative stress disrupts the balance between osteoblastogenesis and osteoclastogenesis, favoring net bone loss. Propolis compounds scavenge ROS and reactive nitrogen species (RNS), activate the NRF2 antioxidant response element, and reduce malondialdehyde levels, thereby protecting bone cell viability and function. This redox-protective mechanism is particularly relevant in postmenopausal osteoporosis, glucocorticoid-induced osteoporosis, and diabetes-associated bone disease.[1][2][3][4][5]
3. Key Bioactive Compounds and Bone-Specific Effects
3.1. Caffeic Acid Phenethyl Ester (CAPE)
CAPE (C₁₇H₁₆O₄; MW 284.31 g/mol) is the most extensively studied propolis compound in bone biology. As a specific NF-κB inhibitor, CAPE suppresses osteoclastogenesis by blocking RANKL-induced signaling and inducing osteoclast apoptosis. In osteoblasts, CAPE upregulates RUNX2 and activates the Wnt/β-catenin pathway, improving bone mineral density in osteoporosis models. Activation of the NRF2/HO-1 pathway by CAPE confers chondroprotection in osteoarthritis and reduces ROS-driven bone resorption in glucocorticoid- and periodontitis-induced models.[1][2]
3.2. Quercetin
Quercetin is a ubiquitous flavonol with bidirectional regulatory activity in bone metabolism. It promotes osteoblast differentiation by upregulating BMP-2, RUNX2, Osterix, and ALP, while simultaneously inhibiting osteoclastogenesis via Wnt/β-catenin stabilization and MAPK pathway modulation. In ovariectomized animal models — a surrogate for postmenopausal estrogen deficiency — quercetin restores bone mineral density and reduces osteolytic activity.[1]
3.3. Kaempferol
Kaempferol modulates the JNK/p38-MAPK axis to suppress osteoclast differentiation and promotes osteoblast activity via Wnt/β-catenin signaling and downregulation of miR-10a-3p. Preclinical evidence supports its role in osseointegration, scaffold-supported bone regeneration, and prevention of inflammatory bone loss.[1]
3.4. Apigenin
Apigenin (C₁₅H₁₀O₅; MW 270.24 g/mol) promotes mesenchymal stem cell commitment to the osteoblast lineage via RUNX2 upregulation and Wnt/β-catenin activation, while inhibiting osteoclastogenesis and pro-inflammatory cytokine secretion (TNF-α, IL-1β, IL-6). Its therapeutic potential in osteoporotic osteoarthritis has been demonstrated in comparative in vivo models.[1][2]
3.5. Pinocembrin, p-Coumaric Acid, Ferulic Acid, and Galangin
These emerging compounds exhibit complementary mechanisms:[1]
- Pinocembrin — activates BMP signaling and estrogen receptor pathways in osteoblasts; suppresses NFATc1 and ROS-dependent osteoclastogenesis
- p-Coumaric acid — increases OPG expression, stimulates growth plate chondrogenesis, and reduces resorption markers
- Ferulic acid — inhibits NF-κB and RANKL expression; activates ERK/MAPK to promote osteoblast survival
- Galangin — anti-inflammatory via NF-κB suppression; osteogenic under inflammatory conditions
4. Translational and Clinical Perspectives
The therapeutic potential of propolis and its bioactive compounds in bone diseases — including osteoporosis, fracture healing impairment, periodontitis-associated bone loss, and peri-implant osteolysis — is well-supported by preclinical evidence across in vitro (MC3T3-E1, BMSCs, RAW264.7) and in vivo (ovariectomy, tibial defect, diabetes, periodontitis rodent models) systems. However, the translation to human clinical trials remains limited, primarily due to chemogeographic variability in propolis composition, challenges in bioavailability and pharmacokinetic standardization, and the absence of multicenter randomized controlled studies.[1][3]
Future research priorities include:
- Standardized extraction and compositional profiling using untargeted LC-MS/MS metabolomics to define bioactive fingerprints
- Nanoformulation and delivery systems to overcome low aqueous solubility and poor intestinal absorption of flavonoids
- Clinical trials in high-risk populations: postmenopausal women, glucocorticoid users, and patients with diabetes-related bone disease
- Combinatorial approaches evaluating synergy between propolis compounds and conventional bone therapies (bisphosphonates, denosumab)
- Sex-stratified analyses, given the estrogen-responsive nature of key propolis targets (ERα, NRF2-NFATc1 axis, RANKL/OPG ratio)[1][5]
References
- Bioactive Compounds from Propolis on Bone Homeostasis: A Narrative Review. https://www.mdpi.com/2076-3921/14/1/81. Retrieved 2026-5-4
- Application of Propolis in Protecting Skeletal and Periodontal Health—A Systematic Review. https://www.mdpi.com/1420-3049/26/11/3156. Retrieved 2026-5-4
- https://dergipark.org.tr/en/pub/ijdor/article/1803201. https://dergipark.org.tr/en/pub/ijdor/article/1803201. Retrieved 2026-5-4
- https://www.mdpi.com/2075-1729/15/5/764. https://www.mdpi.com/2075-1729/15/5/764. Retrieved 2026-5-4
- https://www.tandfonline.com/doi/full/10.1080/27697061.2024.2436515. https://www.tandfonline.com/doi/full/10.1080/27697061.2024.2436515. Retrieved 2026-5-4