Monoclonal antibodies, biologics, are a relatively new treatment option for severe chronic airway diseases, asthma, allergic rhinitis, and chronic rhinosinusitis (CRS).
- airways
- monoclonal antibody
- asthma
- chronic rhinosinusitis
1. Introduction
Chronic inflammatory airway diseases include several overlapping morbidities, such as asthma and chronic obstructive pulmonary disease (COPD) in the lower airways; and allergic rhinitis (AR), nonallergic rhinitis (NAR), and chronic rhinosinusitis (CRS) in the upper airways. AR has a prevalence of 20–30%, NAR has a prevalence of 10%, and CRS has a prevalence of 10–20%, and these common diseases cause remarkable suffering and costs [1][2][3][1,2,3]. They can be subdivided based on such as age of onset, presence of allergy (skin prick test or systemic allergen specific immunoglobulin E (IgE)), with or without nasal polyps and/or T helper (Th) cell 2 prominent inflammation. Exposure to environmental irritants (such as smoking and occupational exposure), recurrent infections, lifestyle factors (such as obesity, stress), co-existing diseases, and genetic/epigenetic factors play a role in disease onset and progression [4][5][4,5]. The diagnostic methods include clinical examination, lung function tests, allergy tests, and paranasal sinus computed tomography scans [5][6][7][5,6,7]. Symptom control of mild cases can be well achieved by the basic treatment such as inhaled/intranasal corticosteroids, inhaled beta agonists, antihistamines, and nasal lavage [5][6][5,6]. Patients with moderate to severe forms often suffer from recurrent infective exacerbations and disease recurrence/progression despite maximal baseline therapy and surgeries. Hence, they require advanced diagnostic methods and therapeutics. Antibodies are an important part of humoral adaptive immunity and homeostasis. They also play a role in airway diseases such as IgE in allergy and CRS with nasal polyps (CRSwNP), antibody deficiency in CRS, and aberrant antiviral IgG responses in asthma exacerbations [5][8][5,8]. Since their introduction about five decades ago, a wide range of monoclonal antibodies are nowadays commercially available and have been largely used in basic and clinical science of airways.
2. Monoclonal Antibodies
Antibodies (immunoglobulin (Ig) A, IgD, IgE, IgG, IgM) are secreted by B-cells that are activated to plasma cells after antigen presentation in regional lymph nodes or secondary lymphoid organs (Figure 1) [9]. Monoclonal antibodies (mAbs) come from a single B-cell parent clone and recognize specifically a single epitope per antigen [10]. Antibodies are crucial to make leukocytes (such as T killer cells) to detect and destroy pathogens and infected host cells. MAbs are made for laboratory and therapeutic use by various techniques. The first technique described in 1975 was based on creating a hybridoma by combining an activated B-cell from an immunized animal spleen and immortalized myeloma cell, resulting in a stable hybrid cell line producing monoclonal antibody [11]. The first mAbs used in therapeutic purposes were of murine origin, which generated unwanted immunogenic reactions and human anti-mouse antibody formation [12]. The revolution of molecular biology techniques has enabled the production of humanized and fully human mAbs that have helped to tackle this problem, although anti-drug antibodies are still one of the outcomes of immunogenicity [12]. For research and laboratory use, there are exponential numbers of commercially available specific monoclonal antibodies for immunoassays such as immunohistochemistry, immunofluorescence and enzyme-linked immunosorbent assay (ELISA) [13]. Since their invention about 50 years ago, there has been a large interest to use monoclonal antibodies in experiments to discover relevant proteins and pathways behind airway pathologies [14][15][14,15].
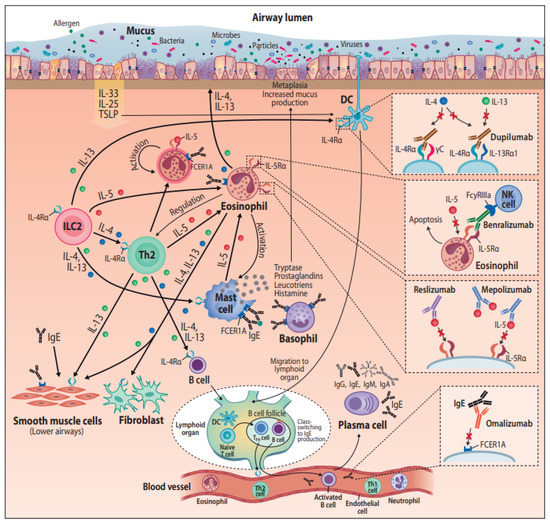
Figure 1. Monoclonal antibodies in the treatment of airway diseases, with their postulated pathways. Abbreviations: DC = dendritic cell, FCER1A = Fc fragment of Immunoglobulin E receptor 1A, FcyRIIIa = Fc fragment of IgG low affinity IIIa receptor, IgA = Immunoglobulin A, IgE = Immunoglobulin E, IgG = Immunoglobulin G, IgM = Immunoglobulin M, IL(-4, -4Rα, -5, -5Rα, -13, -13Rα, -25, -33) = Interleukin(-type), ILC2 = Group 2 innate lymphoid cells, NK cell = Natural killer cell, TFH cell = T follicular helper cell, Th1 = T helper type 1, Th2 = T helper type 2, TSLP = Thymic stromal lymphopoietin.
3. Monoclonal Antibodies and Treatment of Airway Diseases
Unraveling the pathogenesis of diseases has provided the basis for the pharmaceutical industry to develop protein drugs, or “biologics”, with higher specificity and mechanism of action than small molecule drugs. In 2015, monoclonal antibodies were the most important class of biologics approved by the United States Food and Drug Administration (FDA) [16], and their utilization in therapy has rapidly increased since. Personalized medicine is addressing the issue of providing targeted treatment for the right patient [17]. The endotype-driven treatment approach requires careful selection of the patient population who might benefit from a treatment by advanced therapies [18][19]. In the following chapter, mAbs used to treat asthma and CRSwNP are introduced; their main mechanisms of actions are illustrated in Figure 1.
3.1. Commercially Available Monoclonal Antibodies and Their Mechanisms of Action
I
Un the fast phase of allergic reaction, allergen-specific IgE produced by B-cells binds to high affinity FcR (FceRI) expressed on immune cells such as basophils and mast cells. Then, allergen exposure can lead to antigen cross-linking IgE molecules on the same mast cell, receptor aggregation, and initiation of the intracellular signal cascade leading to degranulation and the release of histamine, prostaglandins, and cytokines that mediate the clinical manifestations of atopy [20]. Omalizumab, a humanized IgG1/k monoclonal antibody, taaveling the pathogenesis of diseases has prgets the Fc region of IgE, and by binding to free IgE in blood and body fluids, it neutralizes the ability of IgE to bind to its receptor (FcεRI, high-affinity receptor and FcεRII, low-affinity receptor) [21]. On top of inhibiting the crosvided the bas-linking on mast cells, this induces the down-regulation of IgE receptor expression on other immune cells such as basophils and dendritic cells [22][23]. Os for the pharmalizumab was the first biological therapy developed for asthma, and it has now been used for 15 years. During these years, the functions of IgE in bronchial asthma have proven to be more complex than that of the classical role in allergy and anaphylaxis (reviewed in [89]). For example, smooth meutical induscle cells in lung tissue have receptors for IgE, and it is involved in their proliferation, independent of the presence of allergens. IgE also plays a role in non-allergic diseases such as chronic idiopathic urticaria and CRSwNP and is involved in eosinophilic inflammation [24].
3.1.2. Mepolizumab and Reslizumab—Anti-IL-5
Type 2 inflammation present in asthma anry to d CRSwNP is featured with airway eosinophilic infiltration, particularly in nasal polyps. Eosinophils are also frequently elevated in peripheral blood in type 2 asthma. High eosinophil levels are associated with exacerbations and bronchial obstruction [25]. The key mediator of eosinophils is interleukin-5 (IL5), beinvelop protein drug responsible for their differentiation, growth, activation, and survival as well as recruitment to airways [26][27]. Mepolizuma, or “b is a humanized IgG1/k monoclonal antibody toward IL-5, binding to it with high affinity and preventing its linkage to IL-5Rα [28][29]. Reslizumab is a humanized IgG4/κ monoologiclonal antibody specifically interacting with the epitope IL-5 uses to bind its receptor IL-5Ra, thereby blocking its bioactivity [30].
3.1.3. Benralizumab—Anti-IL-5Ralpha
Different from mepolizumab and reslizumab, benralizumab binds to IL-5-receptor instead of its ligand. Benralizumab is an afucosylated ”, with highumanized IgG1/κ monoclonal antibody, selectively recognizing the IL-5Rα subunit [31]. The interaction of benralizumab with IL-5Rα r sprevents IL-5 binding to target cells and impedes the heterodimerization of IL-5Rα and βc subunits, thus inhibiting the activation of IL-5-dependent signaling cascades. In addition, benralizumab binds to the FcγRIIIa membrane receptor expressed by natural killer cells through the constant Fc region. FcγRIIIa activation induces the eosinophil apoptosis cificity and mechanism called antibody-dependent cell-mediated cytotoxicity, which is amplified by afucosylaof action [32], resulting in depletion of the blood eosinophils. A recent study describes also reduction in the number of basophiles after treatment with benralizumab [33].
3.1.4. Dupilumab—Anti IL-4Ralpha
Dupian smallumab is a fully human monoclonal antibody to the interleukin-4 receptor α subunit, IL-4Ralpha, which is utilized by two cytokines IL-4 and IL-13 [34]. IL-4 mediates its biological effects by binding to IL-4Rα, which is followed by the recmolecule druitment of either gamma c or IL-13 receptor alpha 1 (IL-13Rα1) to form a signaling complex [35]s. IL-13 binds to IL-13Rα1 and then forms a signaling complex by recruiting IL-4Rα [35]. Altogether 2015, IL-4Ralpha is involved in three different combinations of receptor complexes, and the intracellular response potencies are varied between the binding ligand, IL-4 vs. IL-13 [35][36].
Due to the shonoclonal ared receptor, IL-4 and IL-13 also have overlapping functions, and these sister cytokines act both cooperatively as well as independently in type 2 inflammation cascades. Both interleukins promote B-cell proliferation and class switch to IgG4 and IgE [37]. IL-13 tibodies were the most is a cytokine secreted by activated Th2 cells, and it acts as an important mediator of allergic inflammation pathogenesis. Distinct functions for IL-13 include tissue remodeling, goblet cell mucus hypersecretion, subepithelial fibrosis, and emphysematous changes [38]. IL-4 and IL-13 can both class of biologinduce Th2 cells and epithelial cells to produce eosinophil-promoting factors (i.e., IL-5 and eotaxins) and stimulate eosinophils to migrate to sites of inflammation from blood [39]. Howes approver, a recent murine model study shows that only dual IL-4/IL-13 blockade prevented type 2 inflammation broadly enough to prevent lung-function impairment—blocking only IL-4 or IL-13 alone was not enough to provide major clinical benefits [40]. This h by the United Stas been seen also in clinical experiments with IL-4 and IL-13 blockers for the treatment of type 2 diseaseses Food [41]. Dual blockade of IL-4/IL-13 with dupilumab halted eosinophil infiltration into lung tissue in mouse model without affecting circulating eosinophils, demonstrating that tissue, but not circulating eosinophils, contribute tod Drug Administration (FDA) [81], disease pathology [40].
3.2. Monoclonal Antibodies in Asthma Treatment
Monoclonal antibodies are considered as a treatment option for severe asthma [42]. First, th the patient’s symptoms are carefully assessed in order to estimate if the patient truly has asthma, if the current symptoms are associated with asthma, if the current asthma drug therapy is adequate, if the patient is adherent for the drug therapy, and that there are no environmental factors that should be considered [42][43]. Poor symptom contror utilization in therapy has rapidl, frequent yearly exacerbations or serious exacerbations, and diminished lung function are signs of uncontrolled asthma and an indication for biologicals if the situation is not controlled with other maximal medication [42] increased since. ControllPed asthma that deteriorates if high-dose inhaled corticosteroids or systemic corticosteroids are tapered is another indication for biologicals [42]. Thrsonalized medicine selection of a suitable drug is based both on allergy (whether the patient has allergic asthma to perennial allergens) but also on eosinophils (whether the patient has high or low blood eosinophils) [44]. Contradictos addry to biologicals in rheumatic diseases, the biologicals targeting IgE or Th2 cytokines have been well tolerated and safe to use [45][46].
3.3. Monoclonal Antibodies in CRS Treatment
Targeted monoclonal antssing the ibody therapies have shown encouraging results in the management of severe CRSwNP. As type 2 CRSwNP and asthma largely overlap, also therapeutics are in some cases targeted to both severe asthma and severe CRSwNP. According to the European Position Paper on Rhinosinusitis and Nasal polyps 2020 (EPOS 2020) guidelines, the indications for using biological sue of providing targeted treatment for CRSwNP include bilateral polyps and at least one previous endoscopic sinus surgery, together with at least three of the following criteria: evidence of type 2 inflammation, need for systemic corticosteroids (or contraindication for it), significantly impaired quality of life, significant loss of smell, or diagnosis of comorbid asthmathe right patient [82]. The effect of the treatment should be evaluated after 4 months and 1 year, and in case there is no response,dotype-driven treatment should be discontinued [5].
Anti-IgE therappy (omalizumab) is the second and latest biologic therapy approved for CRSwNP by the European Medicines Agency (EMA) in August 2020, and it is pending FDA approval for CRSwNP [47]. A study by Groach requirevaert et al. has shown a decrease of symptom score for nasal congestion, anterior rhinorrhoea, loss of sense of smell, wheeze and dyspnea, and a significant reductcareful selection of endoscopic nasal polyp score, radiologic Lund–MacKay score, and asthma symptoms [48]. Another rthe pandomized controlled trial (RCT) by Pinto et al. showed improvement in symptoms, but no significant improvement in Lund–Mackay score or other endpoints [49]. In a recent study ient population patients with N-ERD, both nasal and lung symptoms improved significantly with omalizumab treatment [50]. Howho might benever, these studfies were small, with only around 20 patients in each group. Recent results from two bigger phase 3 RCTs of 265 patients has shown that omalizumab significantly reduced endoscopic nasal polyp score, nasal congestion score, and SNOT-22 score compared to placebo at week 24 [51]. Patiet from a treatments with comorbid asthma reported significant improvement in Asthma Quality of Life Questionnaire scoresby advanced [51].
3.4. Future Monoclonal Antibody Treatments for Airway Diseases
3.4.1. Anti-TSLP
Thymic stromal lymphopoietin (TSLP) is produced by fibroblasts and epithelium and plays aerapies [83,84]. role iIn T cell maturation. TSLP enhances IL type2 cytokine production in mast cells and activates ILC2s together with IL-33 or IL-25. TSLP has shown to associate with asthma and CRSwNP after virus challenge [52]. Tezethe following chapelumab (AMG-157/MEDI9929) is a human anti-TSLP antibody. A DBRCT of 31 mild asthmatics has shown that AMG-157 attenuated allergen-induced early and late asthmatic responses, and it decreased blood and sputum eosinophils [53]. er, mAnti-OX40L promotebs regulatory T (Treg) cells and suppresses T-cell mediated inflammation, and hence, it might be a potential therapeutic target for severeused to treat asthma [54]. Yet, in a study that used a combination of anti-OX40L and anti-TSLP, the expected effects on Treg-mediated inflammation was not observed [55]. Tezepelumab (anti-TSLd CRSwNP) decreases exacerbations and improves lung function measured by FEV1 (forced expiratory volume in one second) statistically significantly compared to placebo in patients with medium-to-high dose inhaled corticosteroids and long-acting beta-2-agonist [56]. Tare introduced; the exacerbation rates were 61–71% lower than in the placebo group depending on the dose of the tezepelumab [56]. A rr main meduction in asthma exacerbations was found irrespective of eosinophil level.
3.4.2. Anti-TNF
Type 2 low pathways hanismight also comprise future targets for monoclonal antibody therapy [57]. A of actionti-TNF could have potential in patients with neutrophilic non-infectious COPD [58] and in severe asthma with mixed type 1/type2 [59][60]. ILC3s secrete IL-17, which ileads to airway mucosal neutrophilia in some forms of asthma and CRS. A randomized, placebo-controlled double-blindustrated in trial was performed in 300 patients with moderate to severe asthma by using anti-IL-17, brodalumab, and it did not show a remarkable effect [61]Figure 1.
3.1. Commercially Available Monoclonal Antibodies and Their Mechanisms of Action
3.1.1. Omalizumab—Anti-IgE
3.1.2. Mepolizumab and Reslizumab—Anti-IL-5
3.1.3. Benralizumab—Anti-IL-5Ralpha
3.1.4. Dupilumab—Anti IL-4Ralpha
3.2. Monoclonal Antibodies in Asthma Treatment
3.3. Monoclonal Antibodies in CRS Treatment
3.4.3. Anti-IL-8
3.4. Future Monoclonal Antibody Treatments for Airway Diseases
3.4.1. Anti-TSLP
3.4.2. Anti-TNF
3.4.3. Anti-IL-8
Neutrophils have surface IL-8 receptors and are the main target cells for IL-8 responses. Anti-IL-8R, CXCR2, has been shown to reduce airway neutrophilia [62]. Two placebo-controlled studies with CXCR2 antagonists have been performed in severe (neutrophilic) asthma patients [63][64]. The results did not show clinical effectiveness; however, in one of the studies, a reduction in sputum and blood neutrophils was observed [63].