SPINA Carb is a physiological approach for the quantitative evaluation of insulin-glucose homeostasis. It delivers calculated biomarkers for pancreatic beta-cell function (SPINA-GBeta) and insulin sensitivity (SPINA-GR), and a static disposition index (SPINA-DI) as an estimate for the loop gain of the feedback loop.
- insulin
- glucose
- diabetes mellitus
- prediabetes
- homeostasis
- structure parameter inference approach (SPINA)
- Disposition index
- SPINA-GBeta
- SPINA-GR
- SPINA-DI
1. Fundamentals
Like the HOMA and QUICKI indices, the structure parameters are calculated from fasting concentrations of insulin and glucose[1]. The equations are derived from a platform for nonlinear modelling of endocrine feedback loops (MiMe-NoCoDI approach)[2].
The calculations require simultaneous measurements of insulin and glucose concentrations in the blood after eight hours of fasting. The approach delivers estimates for the secretory capacity of pancreatic beta cells (Gβ or SPINA-GBeta, the maximum amount of insulin that can be secreted in one second), the insulin receptor gain (GR or SPINA-GR) and a static disposition index (SPINA-DI) as an estimate for the loop gain of the feedback control system.
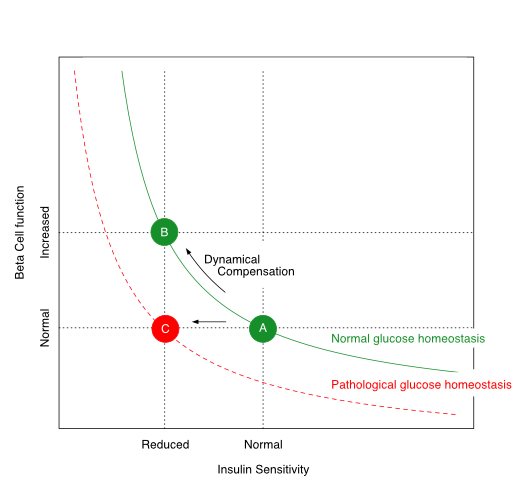
Relation between insulin receptor gain (SPINA-GR as a measure of insulin sensitivity),
secretory capacity of pancreatic beta cells (SPINA-GBeta as a biomarker for beta-cell function)
and the static disposition index (SPINA-DI)
The calculated biomarkers correlate with the M value in euglycaemic clamp investigations, the two-hour result of the oral glucose tolerance test (OGTT), the glucose rise in OGTT, the proportion of glycated haemoglobin, and the abdominal fat mass. In three independent cohorts, it was demonstrated that the parameters have higher reliability and diagnostic accuracy than alternative methods for assessing glucose homeostasis[1][3].
Calculating SPINA-GBeta and SPINA-GR has helped to identify a new type of MODY diabetes characterised by insulin resistance and caused by a mutation in the gene encoding the ryanodine receptor type 2[4].
In hidradenitis suppurativa (acne inversa), an inflammatory skin disease, SPINA-GR is reduced and often uncompensated by SPINA-GBeta, so that a subset of affected patients has low SPINA-DI with subsequent type 2 diabetes[5].
2. Calculation
The parameters are calculated as follows[1][3]:
[math]\displaystyle{\hat{G}_\beta=\frac{I_0(D_\beta+G_0)}{G_3 G_0}}[/math]
[math]\displaystyle{\hat{G}_R=\frac{G_1 P_0(D_R+I_0)}{G_E I_0 G_0}-\frac{D_R}{G_E I_0}-\frac{1}{G_E}}[/math]
[math]\displaystyle{DI=\hat{G}_\beta \hat{G}_R}[/math]
with:
I0: fasting insulin concentration (mol/L)
G0: fasting glucose concentration (mol/L)
DBeta: EC50 of glucose at pancreatic beta cells (7 mmol/L)
G1: parameter for pharmacokinetics (154,93 s/L)
G3: parameter for pharmacokinetics (58,8 s/L)
DR: association constant of the insulin receptor (1,6 nmol/L)
GE: effector gain (50 s/mol)
P0: constitutive endogenous glucose production (150 µmol/s)
3. Interpretation
Reference ranges have been defined based on the NHANES 2009/2010 cohort and are 0.64–3.73 pmol/s for SPINA-GBeta, 1.41–9.00 mol/s for SPINA-GR and 4.01–7.65 for SPINA-DI. Of note, SPINA-GBeta is elevated if SPINA-GR is low in order to compensate for low insulin sensitivity. In this situation, the static disposition index (SPINA-DI) remains constant. In prediabetes and type 2 diabetes, this capacity of dynamical compensation is impaired[6].
References
- Johannes W. Dietrich; Riddhi Dasgupta; Shajith Anoop; Felix Jebasingh; Mathews E. Kurian; Mercy Inbakumari; Bernhard O. Boehm; Nihal Thomas; SPINA Carb: a simple mathematical model supporting fast in-vivo estimation of insulin sensitivity and beta cell function. Sci. Rep.. 2022, 12, 1-13.
- Dietrich, J. W.; Boehm, B. O. Die MiMe-NoCoDI-Plattform: Ein Ansatz für die Modellierung biologischer Regelkreise; GMDS 2015: 60. Jahrestagung der Deutschen Gesellschaft für Medizinische Informatik, Biometrie und Epidemiologie e. V., Eds.; gmds: Köln, 2015; pp. DocAbstr. 284.
- Johannes W. Dietrich; Assjana Abood; Riddhi Dasgupta; Shajith Anoop; Felix K. Jebasingh; R. Spurgeon; Nihal Thomas; Bernhard O. Boehm; A novel simple disposition index (SPINA‐DI) from fasting insulin and glucose concentration as a robust measure of carbohydrate homeostasis. J. Diabetes. 2024, 16, e13525.
- Vikas Bansal; Bernhard R. Winkelmann; Johannes W. Dietrich; Bernhard O. Boehm; Whole-exome sequencing in familial type 2 diabetes identifies an atypical missense variant in the RyR2 gene. Front. Endocrinol.. 2024, 15, 1258982.
- Nessr Abu Rached; Johannes W. Dietrich; Lennart Ocker; Eggert Stockfleth; Yannik Haven; Daniel Myszkowski; Falk G. Bechara; Endotyping Insulin–Glucose Homeostasis in Hidradenitis Suppurativa: The Impact of Diabetes Mellitus and Inflammation. J. Clin. Med.. 2025, 14, 2145.
- E. Ferrannini; A. Mari; Beta cell function and its relation to insulin action in humans: a critical appraisal. Diabetol.. 2004, 47, 943-956.