The disposition index, abbreviated DI, is an important concept in both theoretical and clinical diabetology. Serving as a biomarker for the function of the insulin-glucose feedback control system, it can be determined using various methods and provides an estimate of the loop gain of the homeostatic system. Generally, it is calculated as the product of pancreatic beta-cell function times insulin sensitivity.
- Disposition index
- hidradenitis suppurativa
- acne inversa
- prediabetes
- SPINA-GBeta
- SPINA-GR
- SPINA-DI
- Glucose clamp
- fsIGT
- fsOGT
1. Background
Under physiological conditions, insulin sensitivity and beta cell function adapt to each other over a prolonged period[1]. This means that in cases of ‘healthy’ obesity, i.e. without diabetes mellitus, beta cell mass slowly increases as insulin sensitivity decreases (i.e. insulin resistance increases). Conversely, beta cell function decreases in conditions of high insulin sensitivity (e.g., in prolonged starvation). This long-term adaptation of glandular mass to demand is a general principle in endocrinology, which is referred to as dynamical compensation.
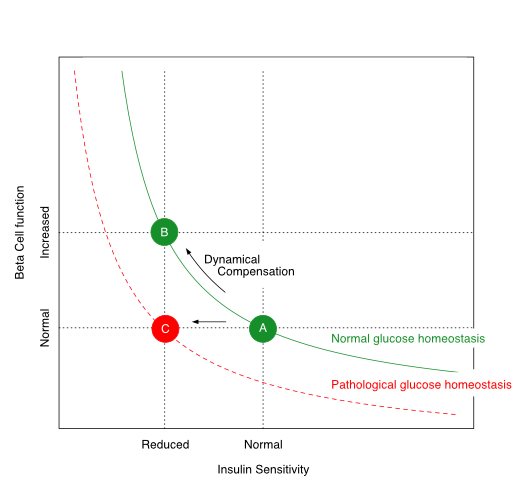
The relationship between insulin sensitivity and beta-cell function is hyperbolic in a ‘metabolically healthy’ organism. Via dynamic compensation, beta-cell mass increases with progressive insulin resistance, whereas the disposition index, which is the product of insulin sensitivity and beta-cell function (green line), remains constant (transition from A to B). If this does not happen or is insufficient (transition from A to C), the result is prediabetes or type 2 diabetes mellitus.
The disposition index, which is the product of insulin sensitivity and beta-cell function, remains constant in healthy organisms despite variations in body composition and insulin resistance. If, however, the pancreatic beta cells are no longer able to compensate for increasing insulin resistance by increased cell mass, the disposition index decreases and glucose homeostasis is impaired. This is the case in advanced metabolic syndrome. Depending on the extent of the reduction in the disposition index, prediabetes or type 2 diabetes mellitus may develop.
2. How to Determine the Disposition Index
For determining the disposition index, data on insulin sensitivity and beta-cell function have to be obtained. This can be done in various ways:
- via a glucose clamp investigation
- via a frequently-sampled intravenous glucose tolerance test (fsIGT)
- an oral glucose tolerance test with a narrow temporal grid of measurement (‘frequently-sampled oral glucose tolerance test’, fsOGT) or
- based on fasting concentrations for glucose and insulin (SPINA Carb).
3. Calculation
3.1. Glucose Clamp
If based on a glucose clamp investigation, the disposition index is calculated as the product of the insulin response curve (AUCΔInsulin) and the insulin sensitivity index (ISIClamp) with
 [2]
[2]
ISIClamp is the ratio of the mean glucose infusion rate and the mean insulin concentration during the clamp:
3.2. Intravenous Glucose Tolerance Test
Using the frequently sampled intravenous glucose tolerance test (fsIGT), the time series of insulin and glucose concentration are to be fitted to the minimal model of glucose homeostasis by Bergman and Cobelli. Then the disposition index can be calculated with

from the first phase of the insulin response (φ1) and the insulin sensitivity index (S1)[3].
3.3. Oral Glucose Tolerance Test
If the frequently sampled oral glucose tolerance test (fsOGT) is used, it is to be coupled with the approach of Matsuda and DeFronzo. Then, the disposition index can be calculated with

from the insulinogenic index (IGI) and the insulin sensitivity index (ISIcomposite)[4].
3.4. SPINA Carb
This method delivers a static disposition index that requires fasting concentrations of insulin and glucose only. It is calculated with

as the product of the secretory capacities of pancreatic beta cells (SPINA-GBeta) and the reconstructed insulin receptor gain (SPINA-GR)[5][6].
4. Interpretation
The approaches presented provide similar but slightly different information. Even though the results of the four methods correlate significantly with each other[6], several biological factors may cause certain deviations. These are rooted, for example, in the different mechanisms that determine static and dynamic insulin secretion patterns. In a comparative study, the discriminatory power of the static disposition index for the diagnosis of diabetes mellitus was higher than that of the oGTT-based disposition index according to Matsuda and DeFronzo[6].
5. Clinical Significance
The disposition index is reduced in diabetes mellitus and prediabetes[6][7].It is also reduced in certain chronic and inflammatory conditions, including cystic fibrosis[8], reduced PCSK9 expression[9], obstructive sleep apnea[10] and hidradenitis suppurativa (aka acne inversa)[11].
6. Prognostic aspects
A reduced disposition index predicts the evolution of type 2 diabetes[12]. In a prospective evaluation of the NHANES study, a reduced static disposition index (SPINA-DI) predicted all-cause mortality over 10 years[13].
7. Therapeutic interventions
Therapeutic measures leading to an improved disposition index include physical activity and nutritional interventions[14]. In carriers of the risk allele of the gene for the transcription factor TCF7L2 increased dietary fibre intake led to a rising disposition index[15].
References
- Bergman RN, Ader M, Huecking K, Van Citters G. Accurate assessment of beta-cell function: the hyperbolic correction. Diabetes. 2002, 51 Suppl 1, S212-20.
- Shah SS, Ramirez CE, Powers AC, Yu C, Shibao CA, Luther JM. Hyperglycemic clamp-derived disposition index is negatively associated with metabolic syndrome severity in obese subjects. Metabolism. 2016, 65(6), 835-42.
- Bergman RN. Origins and History of the Minimal Model of Glucose Regulation. Front Endocrinol (Lausanne). 2021, 11, 583016.
- Matsuda M, DeFronzo RA. Insulin sensitivity indices obtained from oral glucose tolerance testing: comparison with the euglycemic insulin clamp. Diabetes Care. 1999, 22, 1462-70.
- Dietrich JW, Dasgupta R, Anoop S, Jebasingh F, Kurian ME, Inbakumari M, Boehm BO, Thomas N. SPINA Carb: a simple mathematical model supporting fast in-vivo estimation of insulin sensitivity and beta cell function. Sci Rep. 2022, 12, 17659.
- Dietrich JW, Abood A, Dasgupta R, Anoop S, Jebasingh FK, Spurgeon R, Thomas N, Boehm BO. A novel simple disposition index (SPINA-DI) from fasting insulin and glucose concentration as a robust measure of carbohydrate homeostasis. J Diabetes. 2024, 16, e13525.
- Narayan KMV, Kondal D, Chang HH, Mohan D, Gujral UP, Anjana RM, Staimez LR, Patel SA, Ali MK, Prabhakaran D, Tandon N, Mohan V. Natural History of Type 2 Diabetes in Indians: Time to Progression.. Diabetes Care. 2024, 47, 858-863.
- Nielsen BU, Mathiesen IHM, Krogh-Madsen R, Katzenstein TL, Pressler T, Shaw JAM, Rickels MR, Almdal TP, Faurholt-Jepsen D, Stefanovski D. Insulin sensitivity, disposition index and insulin clearance in cystic fibrosis: a cross-sectional study. Diabetologia. 2024, 67, 2188-2198.
- Cyr Y, Lamantia V, Bissonnette S, Burnette M, Besse-Patin A, Demers A, Wabitsch M, Chrétien M, Mayer G, Estall JL, Saleh M, Faraj M. Lower plasma PCSK9 in normocholesterolemic subjects is associated with upregulated adipose tissue surface-expression of LDLR and CD36 and NLRP3 inflammasome. Physiol Rep. 2021, 9, e14721.
- Abu Youssef HA, Elshazly MI, Rashed LA, Sabry IM, Ibrahim EK. Insulin resistance in obstructive sleep apnea. Egyptian Journal of Chest Diseases and Tuberculosis. 2014, 63, 133-9.
- Abu Rached N, Dietrich JW, Ocker L, Stockfleth E, Haven Y, Myszkowski D, Bechara FG. Endotyping Insulin-Glucose Homeostasis in Hidradenitis Suppurativa: The Impact of Diabetes Mellitus and Inflammation. J Clin Med. 2025, 14, 2145.
- Lorenzo C, Wagenknecht LE, Rewers MJ, Karter AJ, Bergman RN, Hanley AJ, Haffner SM. Disposition index, glucose effectiveness, and conversion to type 2 diabetes: the Insulin Resistance Atherosclerosis Study (IRAS). Diabetes Care. 2010, 33, 2098-103.
- Dietrich JW. P4-Endokrinologie – Kybernetische Perspektiven eines neuen Ansatzes. Leibniz Online. 2024, 54, 20.
- Solomon TP, Malin SK, Karstoft K, Kashyap SR, Haus JM, Kirwan JP. Pancreatic β-cell function is a stronger predictor of changes in glycemic control after an aerobic exercise intervention than insulin sensitivity. JCEM. 2013, 98, 4176-86.
- Tolonen UK, Lankinen MA, Laakso M, Schwab US. Association of dietary fibre with type 2 diabetes risk is modified by transcription factor 7 like 2 genotype in men with impaired fasting glucose: The T2D-GENE study. Clin Nutr. 2025, 53, 262-269.