Anterior cruciate ligament reconstruction (ACLR) is the recommended treatment in young and active patients to avoid such secondary damage to other knee structures. [1] Whereas still most surgeons prefer hamstring tendon (HT) autografts, quadriceps tendon (QT) autografts have become increasingly popular even for primary ACLR during the recent years. [2] Recently, numerous studies have shown the beneficial aspects of vancomycin by drastically reducing or even eliminating the risk of postoperative septic arthritis after ACLR. [3,4,5] In the present case series, we present a series of ten patients after undergoing ACLR by using a QT autograft with vancomycin soaking and developing early graft failure due to graft resorption (within 12 months) after the index operation. We then discuss the current literature and possible factors associated with this phenomenon.
- ACL, Anterior cruciate ligament, graft, resporption, graft failure
- ACL
- Anterior cruciate ligament
- graft
- resporption
- graft failure
Early graft failure (graft resorption) after quadriceps tendon autograft anterior cruciate ligament reconstruction – a series of 10 cases
1. Introduction
Patrick Weninger, MD
Veronika Weninger-Pfafl, MD
Andreas Herbst, BSc
Sports Medical Center
Am Hof 11/9
1010 Vienna
+43 699 172 42 838
Corresponding author :
Patri ck Weninger, MD
Abstract
Anterior cruciate ligament reconstruction (ACLR) is the recommended treatment in young and active patients to avoid such secondary damage to other knee structures. [1] Whereas still most surgeons prefer hamstring tendon (HT) autografts, quadriceps tendon (QT) autografts have become increasingly popular even for primary ACLR during the recent years. [2] Recently, numerous studies have shown the beneficial aspects of vancomycin by drastically reducing or even eliminating the risk of postoperative septic arthritis after ACLR. [3,4,5] In the present case series, we present a series of ten patients after undergoing ACLR by using a QT autograft with vancomycin soaking and developing early graft failure due to graft resorption (within 12 months) after the index operation. We then discuss the current literature and possible factors associated with this phenomenon.
List of Figures
Introduction
Anterior cruciate ligament (ACL) in) injuries are frequent orthopaedic injuries leading to knee instability and impaired knee mechanics [1][2][3][4][5][6]. [6] It is commonly accepted that knee instability after an ACL rupture subsequently leads to secondary damage of menisci and cartilage [7]. [7] ACL reconstruction (ACLR) therefore is the recommended treatment of choice in young and active patients to avoid such secondary damage to other knee structures [8]. [8] To reconstruct the torn ACL, various surgical options are available: preservation of the torn ACL by refixation or reconstruction by using autologous tendon grafts or allografts [9]. [9] If the native ACL is replaced by a tendon graft, most surgeons prefer autografts for primary repair whereas allografts are more used for revision cases [10]. [10] If autografts are used, the preferred graft type depends on the surgeon’s choice and is depending on preferences, learning curve and accompanying injuries as well as activity levels, type of preferred sports of a patient and considerations in terms of donor site morbidity [11]. [11]
Whereas still most surgeons prefer hamstring tendon (HT) autografts, quadriceps tendon (QT) autografts have become increasingly popular even for primary ACLR during the recent years [12][13]. [12,13] Rational considerations to use QT autografts for primary ACLR are the comparably easy harvest procedure, lower donor site morbidity and frequent accompanying injuries of the medial compartment including the medial collateral ligament [12]. [12] Some studies suggested lower rates of revision surgery after QT autografts were used for ACLR. Others found similar outcome when comparing QT autografts with other graft types [13][14][15]. [13,14,15] Probably the most important shift of paradigm in ACLR during the past decade was to use the antibiotic vancomycin to soak the tendon graft before implantation. Meanwhile, numerous studies have shown the beneficial aspects of vancomycin by drastically reducing or even eliminating the risk of postoperative septic arthritis after ACLR [3]. [3] In the present case series, we present a series of ten patients after undergoing ACLR by using a QT autograft and developing early graft failure (within 12 months) after the index operation. We then discuss the current literature and possible factors associated with this phenomenon.
2. Operation Method
Operation method
Patients were placed and draped in supine position on the operating table. 8 patients received general anaesthesia, 2 patients had spinal anaesthesia. Single-shot cephazoline was administered in every patient pre-operatively. The middle third of the QT was harvested after a 8 cm longitudinal skin incision. The graft was prepared with a femoral suspensory button device (Tight Rope RT, Arthrex, United States) and armed with tibial non-resorbable sutures (Fiber Wire no. 2, Arthrex, United States). Then, the graft was pre-soaked in 1% Vancomycin for fifteen minutes. Meanwhile, arthroscopic debridement was performed and the bone tunnels were created by using a 9 mm femoral and a 10 mm tibial reamer. The extended version of the surgical and postoperative protocol was recently described by Weninger et al.
3. Case series
Case series
All patients (3 female, 7 male) presented with recurrent knee instability after primary ACLR and after typical rotation-valgus trauma during sports activities. Patients were examined clinically by the first author, scheduled for magnetic resonance imaging to verify the injury and then consented for ACLR by using an ipsilateral QT autograft. None of the patients had an injury of the anterior lateral structures or relevant collateral ligament injuries that needed surgical repair. Six patients had meniscus injury and three had cartilage degeneration or defects. All patients underwent primary ACLR (7 HT and 3 patellar tendon autografts, mean 4.7 years ago (3.4-10.7)). Postoperatively, patients were followed-up for a minimum of twelve months and visited the office every two months for clinical examination. During the twelve months follow-up period, all ten patients reported discomfort and recurrent subjective instability during sports or every day activities. None of the patients reported adequate trauma as possible cause for a graft re-rupture and recurrent instability. As a consequence, all ten patients underwent MRI examination to assess graft integrity (Figures 1). In all ten patients, the MRI scans confirmed complete graft resorption (Figures 1). Arthroscopic evaluation further verified this finding, showing an empty notch with only small tibial remnants in the affected patients (Figure 2). As a result, eight patients underwent revision ACLR by using allografts. Two patients refused to undergo further surgical procedures and chose conservative treatment.
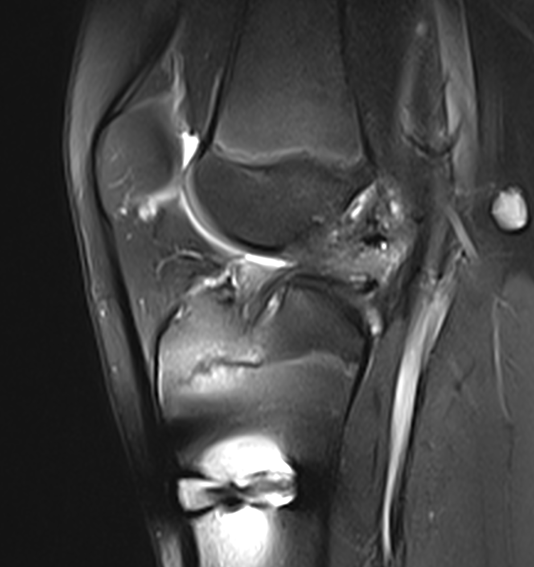
Figure 1: 16-year old male patient at follow-up MRI five months after QT autograft ACLR showing complete graft resorption and missing graft signal.
Figure 1.16-year old male patient at follow-up MRI five months after QT autograft ACLR showing complete graft resorption and missing graft signal.
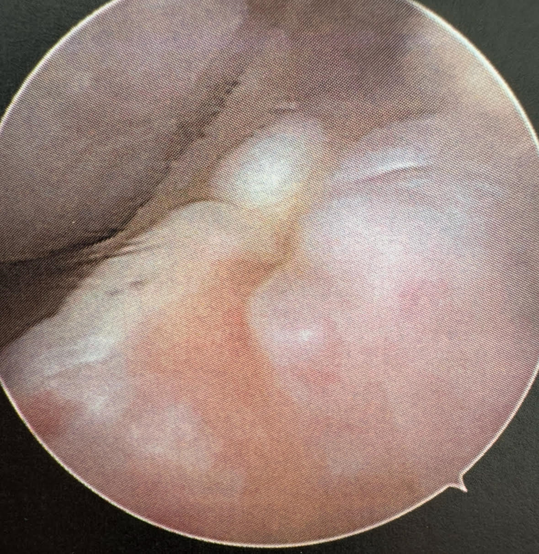
FigureFigure 2. 2: Arthroscopic view into the empty notch of the patient of Figure 1 showing the missing QT autograft with only a little tibial remnant visible. The graft is completely resorbed.
4. Discussion
Discussion
The use of QT autografts for ACLR has become increasingly popular during the last years [1][13]. [1,13] Not only for revision cases but also for primary ACLR the QT seems to be an optimal graft option: easy to harvest also for low-volume surgeons, low donor-site morbidity and customizable grafts in terms of graft diameter and length very useful for individualized ACLR and revision cases [1][12][13]. [1,12,13] Furthermore, some authors even found QT autografts to be superior to HT autografts in terms of revision rates after ACLR. Nevertheless, when overlooking current literature, outcome after ACLR seems to be comparable when comparing QT and HT autografts [13][14][15]. [13,14,15] Probably one of the greatest efforts in ACLR was the publication by Vertullo et al. who firstly described the routine of pre-soaking the graft with the antibiotic vancomycin to reduce septic arthritis after ACLR [16]. [16] Meanwhile, numerous studies showed the beneficial aspects of vancomycin in ACLR de facto eliminating septic arthritis [1]. [1] Not long ago, concerns have been raised by some authors that vancomycin might have cytotoxic effects on cartilage or on graft integrity after inta-articular administration. In this context, Jahier V 2024 et al. published that vancomycin soaking of HT autografts has no negative effects on knee stability and has no negative effects on mechanical strength [17]. [17] In an experimental setting using rat tendons, Thierbach M 2023 et al. showed that the concentration of 5 mg/ml had no negative effect on cell viability in the tendons or the isolated tenocytes [18]. [18] This is also in accordance with Papalia R 2021 et al. who found that vancomycin is useful and safe up to 5 mg/ml which is the clinically relevant concentration [19]. [19] Hees T 2021 et al. reported no increased re-rupture rates after using vancomycin in concentrations of 1 mg/ml [20]. [20] Also Lamplot JD et al. 2021 investigated the biomechanical properties of tendons (bovine patella tendon) after vancomycin exposure (5 mg/ml) and concluded that vancomycin wrapping has no adverse effects on the biomechanical properties of ACL grafts [21]. [21] Perez-Prieto et al. 2021 concluded that wrapping the ACL graft is a safe procedure and does not increase re-rupture rate after ACLR [22]. [22] Due to the beneficial aspects of vancomycin on septic arthritis after ACLR we highly recommend its use and have implemented this into our routine protocol during ACLR. Nevertheless, we critically have to refer to the here presented cases developing early graft failure after QT autograft ACLR. We also need to point out that we did not experience graft resorption after using HT autografts. After having carefully analyzed the current literature, we did not find a single study, be it clinical or experimental, explicitly investigating the effects of vancomycin on QT autografts for ACLR. In all studies evaluating the effect of vancomycin on tendon autografts 100% HT autografts were used or at least were the dominating tendon type. The safety of using vancomycin in QT autograft ACLR has not been evaluated, yet. In contrast, safety and efficacy has been proven for HT autograft ACLR in which the routine use of vancomycin eliminates postoperative arthritis [23]. [23] This and the missing data on safety of vancomycin in QT autograft ACLR lets us conclude not to use QT autografts for ACLR. As a result of unproven safety of vancomycin use in QT autograft ACLR and the undoubtful and proven benefits in HT autograft ACLR and also considering the herein described cases of graft resorption we recommend the routine use of HT autografts in combination with vancomycin for ACLR.
References:
- Mayo Clinic Sports Medicine Center.Achieving optimal outcomes for teen athletes with ACL injury [Internet]. Rochester (MN): Mayo Clinic; 2024 Feb 16 [cited 2025 Feb 13]. Available from: https://www.mayoclinic.org/medical-professionals/orthopedic-surgery/news/achieving-optimal-outcomes-for-teen-athletes-with-acl-injury/mac-20562450
- Slone HS, Romine SE, Premkumar A, Xerogeanes JW. Quadriceps tendon autograft for anterior cruciate ligament reconstruction: a comprehensive review of current literature and systematic review of clinical results. 2015 Mar;31(3):541-54. doi: 10.1016/j.arthro.2014.11.010. Epub 2014 Dec 25. PMID: 25543249
- Naendrup JH, Marche B, de Sa D, et al. Vancomycin-soaking of the graft reduces the incidence of septic arthritis following ACL reconstruction: results of a systematic review and meta-analysis. Knee Surg Sports Traumatol Arthrosc. 2020;28(4):1005-1013
- Banios K, Komnos GA, Raoulis V, et al. Soaking of autografts with vancomycin is highly effective on preventing postoperative septic arthritis in patients undergoing ACL reconstruction with hamstrings autografts. Knee Surg Sports Traumatol Arthrosc. 2020;28(8):2592-2598
- Schuster P, Busch A, Vogt PM, et al. Soaking of the graft in vancomycin dramatically reduces the incidence of postoperative septic arthritis after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc.2020;28(8):2587-2591
- Kohn L, Rembeck E, Rauch A. Verletzung des vorderen Kreuzbandes beim Erwachsenen: Diagnostik und Therapie. Orthopade. 2020;49(11):1013–1028
- Mehl J, Otto A, Baldino JB, et al. The ACL-deficient knee and the prevalence of meniscus and cartilage lesions: a systematic review and meta-analysis (CRD42017076897). Arch Orthop Trauma Surg. 2019;139(6):819–841
- Sanders TL, Maradit Kremers H, Bryan AJ, et al. Incidence of anterior cruciate ligament tears and reconstruction: a 21-year population-based study. Am J Sports Med. 2016;44(6):1502-1507
- Hu J, Qu J, Xu D, Zhou J, Lu H. Allograft versus autograft for anterior cruciate ligament reconstruction: an up-to-date meta-analysis of prospective studies. Int Orthop. 2013 Feb;37(2):311-20. doi: 10.1007/s00264-012-1720-5. Epub 2012 Dec 4. PMID: 23207581; PMCID: PMC3560895
- Grassi A, Nitri M, Ardern CL, et al. Does the type of graft affect the outcome of revision anterior cruciate ligament reconstruction? Bone Joint J. 2017;99-B(6):714-723
- MARS Group. Factors Influencing Graft Choice in Revision Anterior Cruciate Ligament Reconstruction in the MARS Group. J Knee Surg. 2016 Aug;29(6):458-63. doi: 10.1055/s-0035-1564723. Epub 2015 Nov 20. PMID: 26588108; PMCID: PMC5467877
- Xerogeanes JW, Mitchell PM, Karasev PA, et al. Anatomic and morphological evaluation of the quadriceps tendon using 3-dimensional magnetic resonance imaging reconstruction: applications for anterior cruciate ligament autograft choice and procurement. Am J Sports Med. 2013;41(10):2392-2399
- Mouarbes D, Menetrey J, Marot V, et al.Anterior Cruciate Ligament Reconstruction: A Systematic Review and Meta-analysis of Outcomes for Quadriceps Tendon Autograft Versus Bone-Patellar Tendon-Bone and Hamstring-Tendon Autografts. Am J Sports Med. 2019;47(14):3531-3540
- Ashy C, Bailey E, Hutchinson J, et al.Quadriceps tendon autograft has similar clinical outcomes when compared to hamstring tendon and bone-patellar tendon-bone autografts for revision ACL reconstruction: a systematic review and meta-analysis. Knee Surg Sports Traumatol Arthrosc. 2023;31(12):5463-5476
- Runer A, Wierer G, Herbst E, et al.There is no difference between quadriceps- and hamstring tendon autografts in primary anterior cruciate ligament reconstruction: a 2-year patient-reported outcome study. Knee Surg Sports Traumatol Arthrosc. 2018;26(2):605-614
- Vertullo CJ, Quick M, Jones A, Grayson JE. The effect of a vancomycin paste for hamstring graft preparation on the incidence of infection after anterior cruciate ligament reconstruction. 2012;28(3):341-345
- Jahier V, Maximen J, Guillemont P, Bidard Q, Ropars M, Common H.Acta Orthop Belg. 2024 Sep;90(3):415-420. doi: 10.52628/90.3.12980.PMID: 39851012
- Thierbach M, Müller M, Stange R, Kronenberg D, Aurich M, Wildemann B. Wrap It! Preventive Antimicrobial Treatment Shows No Negative Effects on Tenocytes and Tendons—A Comprehensive Approach. J Clin Med. 2023;12(12):4104 doi:10.3390/jcm12124104
- Papalia R, Cicione C, Russo F, Ambrosio L, Di Giacomo G, Vadalà G, Denaro V. Does Vancomycin Wrapping in Anterior Cruciate Ligament Reconstruction Affect Tenocyte Activity In Vitro? Antibiotics (Basel). 2021 Sep 8;10(9):1087. doi: 10.3390/antibiotics10091087. PMID: 34572669; PMCID: PMC8466500
- Hees T, Abdelatif Y, Karpinski K, Bierke S, Häner M, Park HU, Petersen W. Soaking ACL grafts in vancomycin solution (1 mg/ml) reduces the infection rate without increasing the risk for re-rupture and arthrofibrosis. Arch Orthop Trauma Surg. 2022 Jun;142(6):1141-1146 doi: 10.1007/s00402-021-04004-w. Epub 2021 Jul 3
- Lamplot JD, Liu JN, Hutchinson ID, Chen T, Wang H, Wach A, Rodeo SA, Warren RF. Effect of Vancomycin Soaking on Anterior Cruciate Ligament Graft Biomechanics. Arthroscopy. 2021 Mar;37(3):953-960 doi: 10.1016/j.arthro.2020.10.040. Epub 2020 Oct 29. PMID: 33130059
- Pérez-Prieto D, Torres-Claramunt R, Gelber PE, Shehata TM, Pelfort X, Monllau JC. The vancomycin soaking technique: no differences in autograft re-rupture rate. A comparative study. Arch Orthop Trauma Surg. 2021;141(1):41-45
- Figueroa F, Figueroa D, Calvo R, Vaisman A, Espregueira-Mendes J. Vancomycin presoaking of hamstring autografts to prevent infection in anterior cruciate ligament reconstruction: a narrative review. EFORT Open Rev. 2021 Mar 1;6(3):211-216. doi: 10.1302/2058-5241.6.200059. PMID: 33841920; PMCID: PMC8025705
References
- Mayo Clinic Sports Medicine Center.Achieving optimal outcomes for teen athletes with ACL injury [Internet]. Rochester (MN): Mayo Clinic; 2024 Feb 16 [cited 2025 Feb 13]. Available from: https://www.mayoclinic.org/medical-professionals/orthopedic-surgery/news/achieving-optimal-outcomes-for-teen-athletes-with-acl-injury/mac-20562450
- Slone HS, Romine SE, Premkumar A, Xerogeanes JW. Quadriceps tendon autograft for anterior cruciate ligament reconstruction: a comprehensive review of current literature and systematic review of clinical results. 2015 Mar;31(3):541-54. doi: 10.1016/j.arthro.2014.11.010. Epub 2014 Dec 25. PMID: 25543249
- Naendrup JH, Marche B, de Sa D, et al. Vancomycin-soaking of the graft reduces the incidence of septic arthritis following ACL reconstruction: results of a systematic review and meta-analysis. Knee Surg Sports Traumatol Arthrosc. 2020;28(4):1005-1013
- Banios K, Komnos GA, Raoulis V, et al. Soaking of autografts with vancomycin is highly effective on preventing postoperative septic arthritis in patients undergoing ACL reconstruction with hamstrings autografts. Knee Surg Sports Traumatol Arthrosc. 2020;28(8):2592-2598
- Schuster P, Busch A, Vogt PM, et al. Soaking of the graft in vancomycin dramatically reduces the incidence of postoperative septic arthritis after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc.2020;28(8):2587-2591
- Kohn L, Rembeck E, Rauch A. Verletzung des vorderen Kreuzbandes beim Erwachsenen: Diagnostik und Therapie. Orthopade. 2020;49(11):1013–1028
- Mehl J, Otto A, Baldino JB, et al. The ACL-deficient knee and the prevalence of meniscus and cartilage lesions: a systematic review and meta-analysis (CRD42017076897). Arch Orthop Trauma Surg. 2019;139(6):819–841
- Sanders TL, Maradit Kremers H, Bryan AJ, et al. Incidence of anterior cruciate ligament tears and reconstruction: a 21-year population-based study. Am J Sports Med. 2016;44(6):1502-1507
- Hu J, Qu J, Xu D, Zhou J, Lu H. Allograft versus autograft for anterior cruciate ligament reconstruction: an up-to-date meta-analysis of prospective studies. Int Orthop. 2013 Feb;37(2):311-20. doi: 10.1007/s00264-012-1720-5. Epub 2012 Dec 4. PMID: 23207581; PMCID: PMC3560895
- Grassi A, Nitri M, Ardern CL, et al. Does the type of graft affect the outcome of revision anterior cruciate ligament reconstruction? Bone Joint J. 2017;99-B(6):714-723
- MARS Group. Factors Influencing Graft Choice in Revision Anterior Cruciate Ligament Reconstruction in the MARS Group. J Knee Surg. 2016 Aug;29(6):458-63. doi: 10.1055/s-0035-1564723. Epub 2015 Nov 20. PMID: 26588108; PMCID: PMC5467877
- Xerogeanes JW, Mitchell PM, Karasev PA, et al. Anatomic and morphological evaluation of the quadriceps tendon using 3-dimensional magnetic resonance imaging reconstruction: applications for anterior cruciate ligament autograft choice and procurement. Am J Sports Med. 2013;41(10):2392-2399
- Mouarbes D, Menetrey J, Marot V, et al.Anterior Cruciate Ligament Reconstruction: A Systematic Review and Meta-analysis of Outcomes for Quadriceps Tendon Autograft Versus Bone-Patellar Tendon-Bone and Hamstring-Tendon Autografts. Am J Sports Med. 2019;47(14):3531-3540
- Ashy C, Bailey E, Hutchinson J, et al.Quadriceps tendon autograft has similar clinical outcomes when compared to hamstring tendon and bone-patellar tendon-bone autografts for revision ACL reconstruction: a systematic review and meta-analysis. Knee Surg Sports Traumatol Arthrosc. 2023;31(12):5463-5476
- Runer A, Wierer G, Herbst E, et al.There is no difference between quadriceps- and hamstring tendon autografts in primary anterior cruciate ligament reconstruction: a 2-year patient-reported outcome study. Knee Surg Sports Traumatol Arthrosc. 2018;26(2):605-614
- Vertullo CJ, Quick M, Jones A, Grayson JE. The effect of a vancomycin paste for hamstring graft preparation on the incidence of infection after anterior cruciate ligament reconstruction. 2012;28(3):341-345
- Jahier V, Maximen J, Guillemont P, Bidard Q, Ropars M, Common H.Acta Orthop Belg. 2024 Sep;90(3):415-420. doi: 10.52628/90.3.12980.PMID: 39851012
- Thierbach M, Müller M, Stange R, Kronenberg D, Aurich M, Wildemann B. Wrap It! Preventive Antimicrobial Treatment Shows No Negative Effects on Tenocytes and Tendons—A Comprehensive Approach. J Clin Med. 2023;12(12):4104 doi:10.3390/jcm12124104
- Papalia R, Cicione C, Russo F, Ambrosio L, Di Giacomo G, Vadalà G, Denaro V. Does Vancomycin Wrapping in Anterior Cruciate Ligament Reconstruction Affect Tenocyte Activity In Vitro? Antibiotics (Basel). 2021 Sep 8;10(9):1087. doi: 10.3390/antibiotics10091087. PMID: 34572669; PMCID: PMC8466500
- Hees T, Abdelatif Y, Karpinski K, Bierke S, Häner M, Park HU, Petersen W. Soaking ACL grafts in vancomycin solution (1 mg/ml) reduces the infection rate without increasing the risk for re-rupture and arthrofibrosis. Arch Orthop Trauma Surg. 2022 Jun;142(6):1141-1146 doi: 10.1007/s00402-021-04004-w. Epub 2021 Jul 3
- Lamplot JD, Liu JN, Hutchinson ID, Chen T, Wang H, Wach A, Rodeo SA, Warren RF. Effect of Vancomycin Soaking on Anterior Cruciate Ligament Graft Biomechanics. Arthroscopy. 2021 Mar;37(3):953-960 doi: 10.1016/j.arthro.2020.10.040. Epub 2020 Oct 29. PMID: 33130059
- Pérez-Prieto D, Torres-Claramunt R, Gelber PE, Shehata TM, Pelfort X, Monllau JC. The vancomycin soaking technique: no differences in autograft re-rupture rate. A comparative study. Arch Orthop Trauma Surg. 2021;141(1):41-45
- Figueroa F, Figueroa D, Calvo R, Vaisman A, Espregueira-Mendes J. Vancomycin presoaking of hamstring autografts to prevent infection in anterior cruciate ligament reconstruction: a narrative review. EFORT Open Rev. 2021 Mar 1;6(3):211-216. doi: 10.1302/2058-5241.6.200059. PMID: 33841920; PMCID: PMC8025705