Alzheimer’s Disease (AD) and Parkinson’s Disease (PD) represent two among the most frequent neurodegenerative diseases worldwide. A common hallmark of these pathologies is the misfolding and consequent aggregation of amyloid proteins into soluble oligomers and insoluble β-sheet-rich fibrils, which ultimately lead to neurotoxicity and cell death. After a hundred years of research on the subject, this is the only reliable histopathological feature in our hands. Since AD and PD are diagnosed only once neuronal death and the first symptoms have appeared, the early detection of these diseases is currently impossible. Several reasons could be associated with the lack of effective therapeutic treatments. One of the most important factors is the lack of selective probes capable of detecting, as early as possible, the most toxic amyloid species involved in the onset of these pathologies. In this regard, chemical probes able to detect and distinguish among different amyloid aggregates are urgently needed.
1. Introduction
Neurodegenerative diseases represent one of the main causes of public health concerns to date, affecting almost 179 million people worldwide and costing more than EUR 800 billion only in Europe
[1]. Alzheimer’s Disease (AD) and Parkinson’s Disease (PD) are the first and the second most common neurodegenerative diseases, respectively, both of them being amyloidopathies in which an amyloid protein misfolds and aggregates, causing neurotoxicity and cell death
[2]. In the case of AD, the amyloids involved are tubulin associated unit (Tau) and Aβ
1–42, while in PD, α-synuclein (αSyn) is the one whose misfolding and aggregation leads to toxic inclusions and neuronal death. Throughout the preceding century, researchers endeavored to elucidate the primary pathways and pathological features underlying the initiation and progression of AD and PD; although many hypotheses have been put forward, the only histopathological feature characterizing these diseases is still represented by amyloid inclusions. In particular, these entities are Lewy Bodies (LB) in PD, and intracellular neurofibrillary tangles (NFT) and extracellular amyloid plaques in AD
[3][4][3,4]. These histopathological hallmarks strictly correlate with the amyloid hypothesis, which represents the most studied, but also the most controversial one. The association of this hypothesis with the aforementioned histopathological features underscores its prominence as one of the primary hypotheses of neurodegeneration
[4].
Nowadays, AD diagnosis is based on a clinical evaluation and imaging investigation based on techniques such as positron emission tomography (PET), while a definitive diagnosis is confirmed only upon a post mortem examination of the patients’ brain. The diagnosis requires the detection of dopaminergic neuron loss, together with the presence of LB and Lewy neurites for PD. NFT and amyloid plaques are instead required to validate the diagnosis of AD
[5]. The diagnostic criteria and methods for other neurodegenerative diseases are even less reliable. CT (Computer Tomography) and MRI (Magnetic Resonance Imaging) scans of patients’ brains are employed to provide information about the shape, position, or volume of the tissue, thus offering an overview of the progress of central nervous system (CNS) tissue deterioration when the disease is at an advanced stage. Several molecular imaging compounds have been studied so far, with four of them being approved for clinical use. In particular, Florbetaben, Florbetapir, and Flutemetamol have been approved for the detection of beta-amyloid plaques in the brain, and Flortaucipir F18 for the detection of Tau neurofibrillary tangles
[6][7][6,7]. Even though amyloid plaques in the brain are a characteristic feature of AD, their detection through PET imaging cannot be used to diagnose the disease. Indeed, the presence of Tau neurofibrillary tangles correlates better with cognitive symptoms in AD with respect to that of amyloid plaques. Moreover, these latter aggregates are not easily detectable with Aβ PET tracers. In addition, Aβ aggregates cannot be considered as a specific hallmark of AD, as amyloid plaques are frequently also found in dementia with Lewy bodies (i.e., the second most common degenerative dementia), as well as in blood vessels in cerebral amyloid angiopathy. Therefore, patients with these conditions show high signals on amyloid PET scans that are similar in pattern to those seen in AD
[8][9][8,9].
2. Strategies for the Diagnosis of Pre-Symptomatic Neurodegenerative Diseases
Significant advances have been made in amyloidosis imaging so far; however, methods that can help to diagnose and differentiate among patients with neurodegenerative disorders, ideally pre-symptomatically, are still missing. The identification of novel strategies for diagnosis at the incipient stages of Alzheimer’s disease, i.e., before irreversible brain damage or mental decline has emerged, represents one of the most active research areas. Notably, research and clinical findings have highlighted features and biomarkers whose levels significantly change before the onset of early symptoms of these diseases. For example, amyloid beta peptides (Aβ), truncated Tau proteins, and phosphorylated forms of Tau (p-Tau) are few among the main pathological biomarkers whose detection has been progressively implemented, allowing for the detection of a prodromal form of the disease. Their quantification is commonly performed on cerebrospinal fluid (CSF), a medium collected through lumbar punctures. There are three main ELISA-based methods that have been approved as in vitro diagnostic kits for the quantification of Aβ peptides: Innotest
® ELISA, IBL International
® ELISA, and Euroimmun
® ELISA. Despite their good correlation with PET imaging, these methods still present pre-analytical issues, such as: (i) the absorption to the fluid collection tubes, generating false positive results; (ii) the pretreatment of CSF samples using denaturation in guanidine hydrochloride, and (iii) the time and volume of fluid collection not being fully standardized. In addition, even if immunoassay platforms making use of fluorescence, chemiluminescence, or electrochemiluminescence for detection are valuable approaches for quantification (due to their high sensitivity), they still have the disadvantages of inter- and intra-assay variability. This is mainly because of peptide detectability issues that can derive by the high propensity of amyloids to bind to other proteins, often hiding the epitopes recognised by the antibodies. Another drawback of ELISA-based approaches is their intrinsic inability to fully identify pathological oligomers, which may also be undetectable due to their incorporation into larger aggregates. Indeed, antibodies often detect only specific conformations of aberrant proteins; thus, structurally different Aβ species in the sample remain undetected
[8][10][8,10]. α-synuclein pathological species can be detected in CSF using real-time quaked induced-conversion (RT-QuIC) and protein-misfolding cyclic amplification (PMCA). Interestingly, αSyn pathological aggregates detected by these methods are proven to discriminate between PD and other synucleinopathies such as multiple system atrophy (MSA), suggesting that different polymorphs and strains are present in these diseases
[11][12][11,12]. In the last years, Tau aggregates have been observed in aberrant quantity within different fluids, the most studied being CSF
[13][14][15][13,14,15]. Notably, Tau oligomers aberrantly accumulate in the early phases of tauopathies, and their concentration reflects neurodegeneration progression
[13][14][15][13,14,15], particularly for AD
[16][17][16,17]. While the concentration of biomarkers such as total Tau (t-Tau) and phosphorylated Tau (p-Tau) have been observed to increase early in tauopathies, the diagnosis and discrimination of these pathologies from CSF fluid biomarking present several challenges, such as the invasiveness of fluids collection and the variability across different cohorts of patients
[13][16][18][19][13,16,18,19]. Another potential biofluid for the early detection of tauopathies is blood, whose analysis presents advantages in terms of the personnel and facilities required, being less invasive than CSF collection
[20][21][22][20,21,22]. Unfortunately, there are also several issues related to the identification of Tau biomarkers in blood, like the significantly lower concentration of Tau species in this medium compared to CSF
[15]. The introduction of ultrasensitive single molecule array (Simoa) technology and mesoscale discovery (MSD) ELISA methods recently enabled the identification of blood Tau biomarkers in large populations of patients
[23][24][25][23,24,25], demonstrating that p-Tau may help to discriminate AD from other tauopathies
[11][23][24][26][27][28][11,23,24,26,27,28]. However, it should be pointed out that most research related to the identification of Tau biomarkers in blood has been focused on AD
[23][26][27][28][29][23,26,27,28,29]. Therefore, further efforts are needed to fully understand the utility of blood Tau biomarkers for the early diagnosis and characterization of other tauopathies
[30]. Together with blood, urine has also become one of the most studied fluids for Tau biomarkers’ detection
[31][32][31,32]. For example, it has been recently demonstrated that t-Tau can be detected in urine samples from patients with acute neuronal and glial damage
[33]. Considering the low invasiveness and applicability of urine tests in routine controls, future efforts should be addressed towards the identification of biomarkers facilitating the monitoring of the development and progression of tauopathies. Additionally, saliva could also potentially be investigated for pathological Tau detection
[34][35][36][37][38][39][34,35,36,37,38,39]. For example, altered p-Tau/T-Tau ratios have been observed in saliva samples from patients with AD, with respect to the control population in a recent study
[34]. Similar results were observed by Marksteiner and co-workers
[35], who found significantly higher levels of p-Tau181 and lower t-Tau levels in salivary samples from AD patients
[35]. On the contrary, similar t-Tau concentrations were observed in saliva from patients with AD, MCI, or healthy controls in a recent study by Ashton et al.
[40]. These different outcomes may be explained by saliva composition heterogenicity, as well as restricted patient cohort analysis
[41]. Interestingly, multiple immunoassay platforms and cross-sectional studies have found that t-Tau and p-Tau levels vary in the tears of patients affected by neurodegeneration, with respect to healthy controls
[42][43][44][42,43,44]. As for saliva, further research in larger cohorts of patients is needed to confirm the predictive value of Tau biomarking in tears for the diagnosis of AD and other tauopathies. Finally, nasal secretions are currently under investigation for the possible detection of tauopathies biomarkers
[45][46][47][45,46,47]. Statistically different p-Tau/t-Tau ratios in AD patients were found with respect to the control population in Arrozi’s study, but further research in larger cohorts of patients is needed to confirm the validity of this biofluid for tauopathies monitoring
[48]. To date, the detection of Tau aggregates and tauopathies biomarkers in biofluids has gained interest, especially for cost-effective and non-invasive mediums. However, larger patient cohorts are needed, and variability problems still have to be addressed for the efficient early diagnosis of Tau-related diseases.
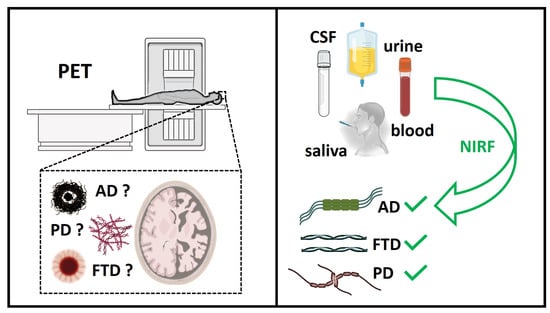
The use of fluorescent probes represents a valuable methodology for monitoring, in real time, the full-time course of aberrant protein aggregation, from monomeric peptide or protein to amyloid, having single-particle sensitivity. However, the expensiveness of the facilities needed for the analyses and the risk of radiation exposure for the current modalities of molecular imaging applied in clinical studies represent inevitable limitations. Therefore, Near-Infrared (NIR) fluorescent imaging (NIRF) has recently attracted attention as a promising non-invasive method for visualizing amyloid plaques in vivo (eye scan technology) or in biofluids (CSF, urine, and saliva) (
Figure 1)
[8]. Compared to PET and single-photon emission computed tomography (SPECT), NIRF has many advantages, such as safe and sensitive detection without radiation damage, moderate cost, and minimal auto fluorescence of the NIR probes from cellular and tissue components. Fluorescent amyloid-binding agents offer substantial opportunities for basic research on amyloid composition. Several efforts have been made in the field of bioimaging using non-invasive NIR probes in the frame of neurodegenerative diseases, particularly for AD diagnosis. Despite their favorable features for in vivo application, their translation into preclinical and clinical practices remains challenging, and further optical improvements and technological evolutions are still needed. In particular, there is a need for new NIR fluorescent probes based on new scaffolds, which are able not only to be selective for distinct amyloid aggregates (e.g., Aβ, Tau, hIAPP, or α-synuclein), but also to be selective over soluble species, such as oligomers. The exploration of new probes that selectively target oligomers of one type of amyloid protein is a priority for future research, because oligomers are produced before the accumulation of plaques and thus can be exploited as early biomarkers of the pathological process, long before symptoms have appeared. When new NIR fluorescent probes that are selective for oligomers and able to distinguish different amyloid aggregates are available, it will be possible to translate NIRF imaging into future clinical applications (
Figure 1).
Figure 1. Schematic representation of two different diagnostic approaches in neurodegeneration through PET (Positron Emission Tomography) and Near-Infrared (NIR) fluorescent imaging (NIRF)