Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 2 by Jessie Wu and Version 3 by Francesco Beritelli.
Early diagnosis of lung pathologies is crucial for improving patient prognosis. So far, chest X-rays are one of the most common imaging modalities used for diagnosing lung pathologies. However, diagnosing lung pathologies based on chest X-rays alone can be challenging and subjective, especially for diseases with similar symptoms.
- Digital Twin
- IoT sensors
- image processing
- lung healthcare
- smart healthcare
- convolutional neural network
1. Introduction
Early diagnosis of lung pathologies is crucial for improving patient prognosis. So far, chest X-rays are one of the most common imaging modalities used for diagnosing lung pathologies. However, diagnosing lung pathologies based on chest X-rays alone can be challenging and subjective, especially for diseases with similar symptoms.
In recent years, deep learning (DL) has shown significant potential in enhancing the diagnosis of lung pathologies based on chest X-rays. DL, a branch of artificial intelligence, utilizes artificial neural networks to learn complex patterns from data. DL systems for lung pathology recognition based on chest X-rays can be classified into two main categories:
-
Detection Systems: these systems are designed to identify the presence of anomalies in chest X-rays.
-
Classification Systems: these systems are designed to classify anomalies in chest X-rays based on the type of lung pathology.
Common DL techniques used for lung pathology recognition based on chest X-rays include
-
Convolutional Neural Networks (CNNs): CNNs are a class of artificial neural networks designed for image processing. They have been successfully employed in order to detect anomalies in chest X-rays, including lung nodules, lung infiltrates, and pneumonia.
-
Recurrent Neural Networks (RNNs): RNNs are a class of artificial neural networks designed for processing sequence data. RNNs have been successfully used to identify anomalies in chest X-rays that develop over time, such as the progression of lung cancer, for example.
-
Generative Adversarial Networks (GANs): GANs are a class of artificial neural networks designed to generate realistic data. GANs have been successfully used for synthesizing chest X-ray images containing anomalies, thus improving the training of DL systems.
Numerous studies have demonstrated the effectiveness of DL in analyzing chest X-rays, achieving remarkable results in the detection and classification of lung nodules, pneumonia, and other thoracic pathologies. For example, Wang et al. developed a DL-based system for lung nodule detection with promising results [1]. Similarly, Kermany et al. demonstrated the effectiveness of DL in classifying pneumonia from chest X-rays [2].
These advancements highlight the transformative potential of DL in chest X-ray analysis. As research efforts continue to refine DL algorithms and expand their range of application, this powerful technology is poised to revolutionize the detection, diagnosis, and treatment of lung diseases, ultimately improving patient outcomes.
Despite remarkable progress, several challenges are faced, impeding full realization of the DL potential in chest X-ray analysis. These challenges include the need for large sets of high-quality annotated image data, ensuring the generalizability of DL models to diverse patient populations, and addressing ethical and regulatory considerations associated with deploying AI in healthcare.
To address these challenges, research efforts should focus on creating comprehensive image datasets, developing robust DL models capable of effectively handling real clinical scenarios, and establishing clear guidelines for the ethical and responsible use of AI in healthcare.
The healthcare landscape is undergoing a profound transformation driven by the convergence of advanced technologies, including not only DL but also the Internet of Things (IoT) and Digital Twins (DTs). These innovations offer enormous potential to revolutionize healthcare delivery in general and, particularly, the field of monitoring lung pathologies.
IoT sensors integrated into wearable devices connected to the Internet enable real-time monitoring of physiological parameters such as heart rate, blood pressure, respiratory rate, and X-ray images of various organs. These continuous data streams enable proactive healthcare interventions, allowing for early detection of potential complications and facilitation of remote patient monitoring.
By providing virtual representations of physical objects or systems, DTs offer a holistic approach to monitoring lung pathologies. By integrating data from IoT sensors, clinical records, and other relevant sources, DTs can provide a comprehensive view of an individual’s lung health, allowing for early detection of subtle changes and personalized treatment recommendations.
2. Lung-Digital Twin Architecture
Lung architecture characterizes the DT based on the specific context. In lung pathology scenarios, input data may be of various types, including numerical data and X-ray images. Unlike the Heart-DT, the Lung-DT must be able to acquire images. Therefore, in addition to the two connectors, there are two distinct Acquisition blocks to process raw data from the real world.
The two present connectors are dedicated to acquiring the SpO2 value from a smartwatch and data from lung X-rays. In addition to the connectors, the data Acquisition block related to the X-ray connector performs resize and categorization operations on the images before storing them in the Storage block. Subsequently, the Storage block is responsible for storing preprocessed data for future use.
The Agent block initiates different decisionmaking processes based on the input data in the storage and programmatically triggers data analysis. Depending on the nature of the analysis, the agent will activate the AI Process block, which processes images or saturation data.
The AI Process block can download various models from the AI Service block, i.e. the reference model for making inferences based on the required analysis. The following chapters will describe the methodology and results of the inference process in which the Lung-DT is required to process lung images.
Finally, once the Agent block obtains the result of processing, it will assess the necessary actions, such as sharing information with other DTs or implementing actions in the real world through the implementation block. Similar to the heart case, the Policy block holds all policies and thresholds to prevent actions that may be harmful to the organ itself.
As shown in Figure 1, the implementation provided in this research on the Lung-DT involves two distinct connectors, both designed to interface directly with the physical world for data acquisition. The first connector is used to acquire SpO2 values from wearable medical devices, such as a smartwatch, while the second is dedicated to acquiring X-ray images from the real world.
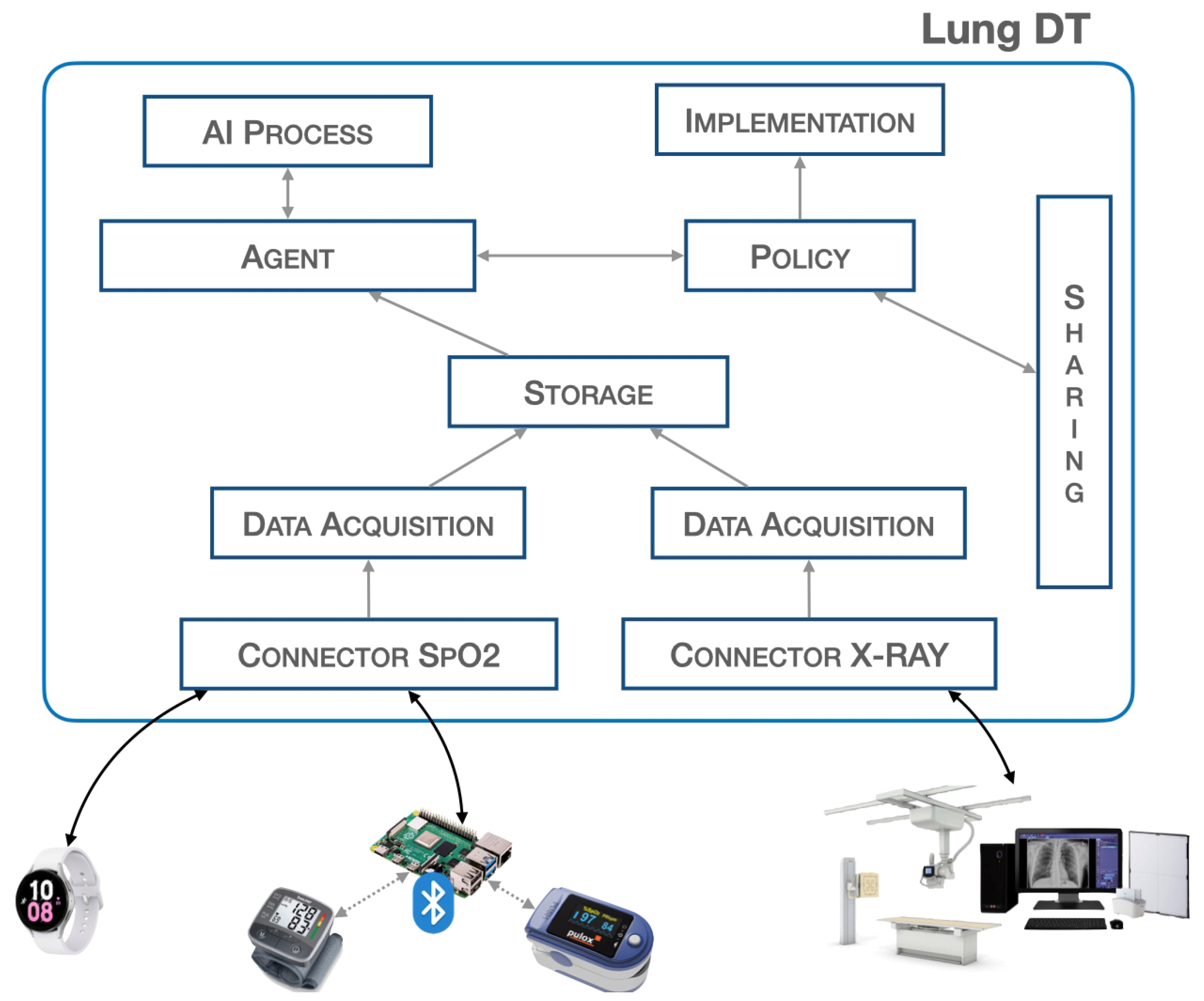
Figure 1. Lung-DT architecture.
3. Lung-Digital Twin Workflow
The workflow related to the Lung-DT is illustrated below. Data from the real world are acquired through a single endpoint that IoT devices and various systems can connect to. The platform exposes various services, as shown in Figure 2, with two connectors (1) dedicated to data acquisition. For saturation data, they are sent via REST API or MQTT, while, for X-ray images, there is an FTP repository where files can be uploaded. It is essential to emphasize that medical personnel uploading the clinical report will only have access to the Lung-DT repository specific to the individual patient.
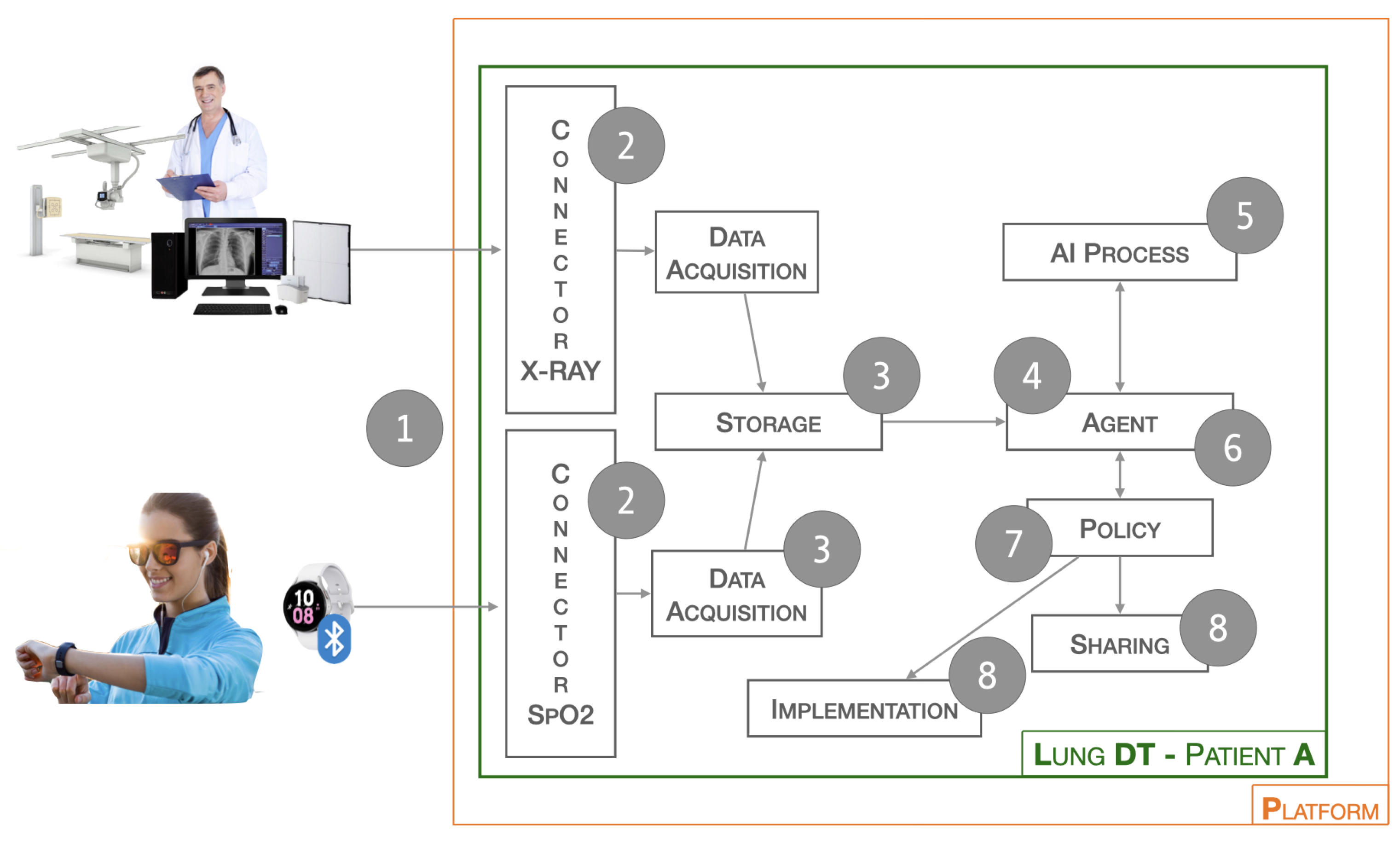
Figure 2. Workflow of Lung-DT.
The next phase (2) involves reading the data and performing cleaning and normalization operations. In this process, operations such as the removal of non-useful metadata, uniformity of format, and file type are carried out. The Storage block (3) is responsible for storing the raw and cleaned data for future use.
The Agent block (4), through cyclical checks or external interactions, initiates the validation and inference process for previously acquired data. In particular, if a new image has been received, it will contact the AI Process block (5) to start the validation process. In the case of an X-ray image, the AI Process block will contact the AI Long Instance X-ray block to check for the presence of a new updated model, which will be used for inference.
Once completed, the result is returned to the Agent block (6) to assess future actions. Specifically, based on the thresholds set in the Policy block (7), certain actions will or will not be taken. These actions may include physical world actions through the Implementation block or sharing with other DTs through the Sharing block (8).
The Implementation block (8) is utilized in the context of this research to implement and establish alert and notification systems for medical specialists. This enables them to promptly consider the possibility of activating remote administration systems, scheduling specific medical exams, or triggering immediate emergency services. The objective is to develop a modular and dynamic architecture capable of adapting to various application scenarios and, above all, facilitating seamless integration of new functionalities without compromising the integrity of the entire system, as previously proposed by the authors in [3].
4. Healthcare Digital Twin Platform
The platform introduced by the authors [3] has been characterized for a specific application related to the lung, as illustrated in Figure 3. In the patient-dedicated section, there are DTs related to both heart and lung, while two generic DTs for pathologies are exemplified. The AI Services section includes three instances, one focused on the cardiac context (AI Heart Instance), while the other two are dedicated to the pulmonary domain. Specifically, there is the AI Lung SpO2 Instance, related to blood saturation data, and the AI Lung X-ray Instance, which handles the processing of lung images. All instances are independent of each other, allowing updates and changes without affecting the behavior of the entire platform. This flexibility enables adapting the platform to specific needs, facilitating the seamless integration of new elements to enhance the overall capabilities of the system. The modular structure of the platform provides the opportunity to customize and expand functionalities based on the evolving requirements of the application.
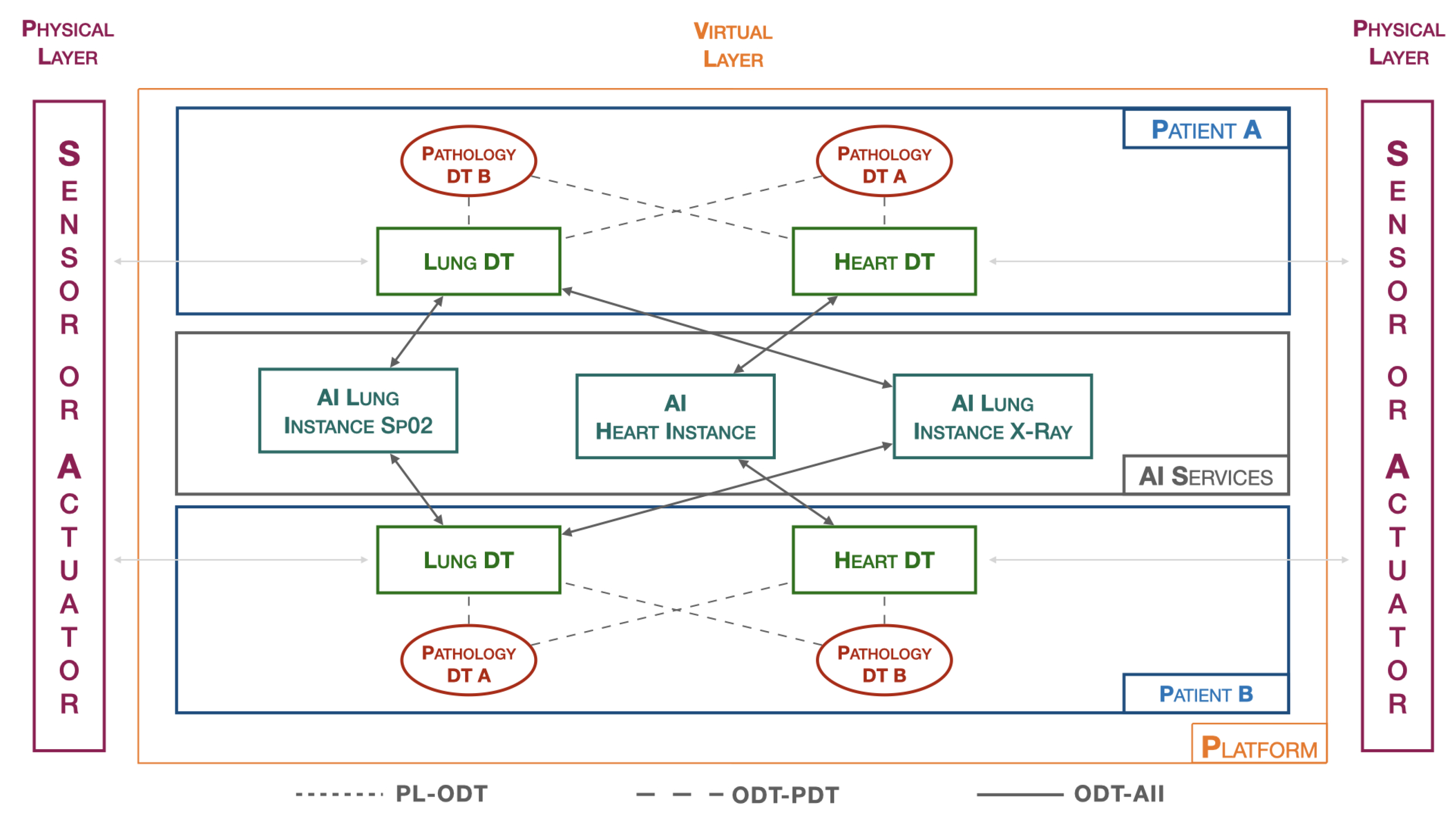
Figure 3. Platform architecture.
References
- Wang, X.; Peng, Y.; Lu, L.; Lu, Z.; Bagheri, M.; Summers, R.M. ChestX-ray8: Hospital-Scale Chest X-ray Database and Benchmarks on Weakly-Supervised Classification and Localization of Common Thorax Diseases. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017.
- Kermany, D.S.; Goldbaum, M.; Cai, W.; Valentim, C.C.; Liang, H.; Baxter, S.L.; McKeown, A.; Yang, G.; Wu, X.; Yan, F.; et al. Identifying Medical Diagnoses and Treatable Diseases by Image-Based Deep Learning. Cell 2018, 172, 1122–1131.
- Avanzato, R.; Beritelli, F.; Lombardo, A.; Ricci, C. Heart DT: Monitoring and Preventing Cardiac Pathologies Using AI and IoT Sensors. Future Internet 2023, 15, 223.
More