Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Laquanda Knowlin and Version 2 by Catherine Yang.
Pediatric surgery is the diagnostic, operative, and postoperative surgical care of children with congenital and acquired anomalies and diseases. The early history of the specialty followed the classic “see one, do one, teach one” philosophy of training but has since evolved to modern methods including simulation-based training (SBT). Current trainees in pediatric surgery face numerous challenges, such as the decreasing incidence of congenital disease and reduced work hours.
- pediatric surgery
- simulation training
- education
- neonatal
1. Introduction
Pediatric surgery involves the diagnostic, operative, and postoperative surgical care of children with congenital and acquired anomalies and diseases [1]. There is no universal definition of a pediatric surgeon, as some are recognized through specific board certification while others have developed a niche based on clinical experience alone [2]. The journey to become a surgeon that operates on this special population is tedious but rich in history.
2. The Future Direction of the Simulation-Based Training of Pediatric Surgeons
As pediatric surgical simulation training continues to evolve, the future needs of the field should include the creation of more models tailored to pediatric surgery, the expansion of video gaming technology to clinical areas of limited training exposure, and more implementation of simulation-based curricula. Previous reviews have noted that very few pediatric surgical simulators are readily available for purchase, but some literature examples enable departments and hospitals to develop their own [3][35]. Now that 3D printers have become more commercialized, some hospitals have 3D printing programs or institutes for clinical and research purposes. It is possible to print anatomic structures—like bones to internal organs—that can be handled during surgical procedures. Engineers and trained technicians can therefore develop products to meet the haptic and tactile needs of surgeons (Figure 1). A hybrid of 3D printing and cadaver tissue has even been used [4][30].
Figure 1. Neonatal Abdominal wall defect models created for the Pediatric Surgery Fellow Workshop at Las Madrinas Simulation Center (Los Angeles, CA, USA).
2.1. Technology Expansion
The expansion of video gaming technology also enables training in areas of limited exposure for pediatric surgery trainees. These are low-frequency, high-stakes events. One such area is pediatric trauma education. Pediatric trauma is the leading cause of mortality in children [5][51]. It is essential to prepare providers, surgeons, and non-surgeons to take care of this special population to improve outcomes. However, specific simulators for trauma are very limited, especially for pediatric and infant patients. Moulage, special makeup, is often used to simulate critical injuries on non-trauma-designated manikins (Figure 2a,b). Trauma simulators can range from USD 14,000 to USD 200,000 depending on the size of the manikin and the level of desired fidelity [6][7][8][52,53,54]. A lower-cost simulation solution is digital. Several companies are creating simulation training through VR to train providers with minimal exposure to pediatric trauma [9][55]. Specialized topics include mass casualty situations in both the military and civilian populations. It provides a psychologically safe environment to practice making life-saving decisions in preparation for actual events. Taking it a step further, augmented reality (AR) decision-making systems with algorithms for trauma activations have been designed in New Zealand, with expanded use in Asia and the Middle East [10][56]. Collaboration among adult and pediatric surgeons can expand this further and help reduce morbidity and mortality outcomes in children around the world. The surgical field is shifting to implementing artificial intelligence (AI) which encompasses machine learning, to offer feedback on trainee surgical performance after video review [11][57]. As surgical fields such as neurosurgery, urology, and some general surgery subspecialties look to artificial intelligence, the question remains if pediatric surgery will follow suit [12][13][14][58,59,60]. Similar to 3D VR, AI has been proposed for pre-operative planning with a focus on visualization [15][61]. However, there is still work that needs to be done as far as reducing implementation and production costs, providing clear evidence that this technology is superior to the current standard, and addressing intrinsic technology limitations (i.e., cybersickness, head-mounted devices, and power for graphic processors) [10][56]. Future technologies are likely to improve haptic sensations in VR and digital simulations, building on hybrid models that combine tactile sensations with digital solutions to achieve learning objectives. Haptics are not optimized for current digital simulations, despite the importance of haptic feedback in pediatric surgical procedures. The researchers predict that haptic technology will enhance future training, which will fully enable digital and distance-based simulations for pediatric surgeons [16][62]. In addition, as the future becomes even more technology-driven, we must not forget the importance of pediatric surgery training in countries with limited resources or technological access (Figure 3).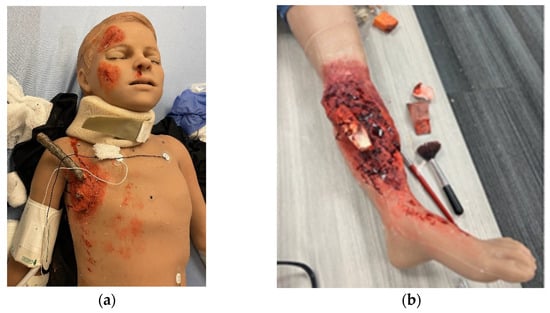
Figure 2. Trauma moulage to simulate critical injuries on a pediatric medical simulator (Pediatric HAL, Gaumard Scientific) at Las Madrinas Simulation Center (Los Angeles): (a) penetrating chest trauma and (b) open orthopedic fracture.
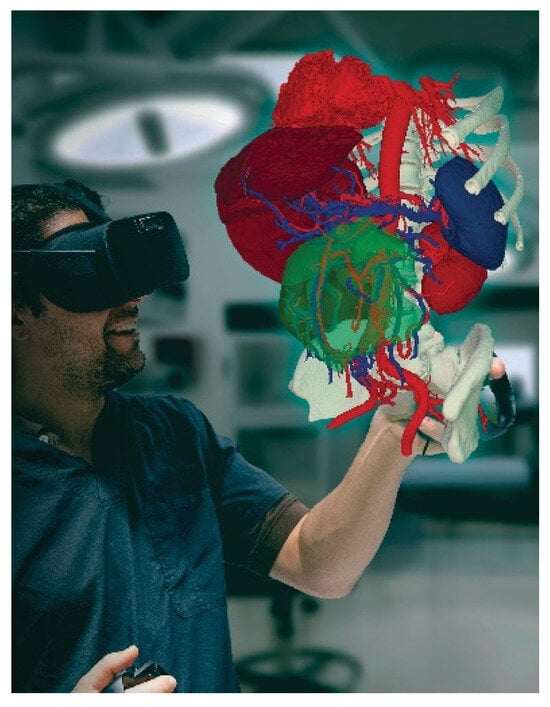
Figure 3.
Preoperative planning using 3D virtuality reality software ImmersiveView 5.0 by ImmersiveTouch (Chicago, IL, USA).