Lung cancer is the leading cause of cancer deaths in men and women in the United States. Accurate staging is needed to determine prognosis and devise effective treatment plans. The International Association for the Study of Lung Cancer (IASLC) has made multiple revisions to the tumor, node, metastasis (TNM) staging system used by the Union for International Cancer Control and the American Joint Committee on Cancer to stage lung cancer. The eighth edition of this staging system includes modifications to the T classification with cut points of 1 cm increments in tumor size, grouping of lung cancers associated with partial or complete lung atelectasis or pneumonitis, grouping of tumors with involvement of a main bronchus regardless of distance from the carina, and upstaging of diaphragmatic invasion to T4.
1. Introduction
In 2020, lung cancer accounted for 1.8 million deaths worldwide
[1][2][1,2]. Initial staging of the disease is typically performed with computed tomography (CT) and positron emission tomography/computed tomography (PET/CT). TNM-8 used a database of 94,708 patients from 1999 to 2010 collected from 35 centers in 16 countries
[3]. This staging system is used for clinical and pathologic lung cancer staging for all histologic subtypes of the disease
[3]. Since 2016, the TNM staging system has been established as the standard system of lung cancer staging by the Union for International Cancer Control (UICC) and the American Joint Committee on Cancer (AJCC). Histologic subtypes of lung cancer, such as non-small cell lung cancer (NSCLC), small cell lung cancer (SCLC), and bronchopulmonary carcinoid tumor, can all be clinically and pathologically staged using the TNM classification
[4]. This staging system stratifies patient survival by using three factors to determine the anatomical extent of the malignancy: primary tumor (T), nodal metastasis (N), and metastasis to intra- and extrathoracic sites (M) (
Table 1 and
Table 2). For patients with small cell lung cancer, TNM-8 has been validated by an analysis of more than 5000 patients in the IASLC database
[5]. For patients with bronchopulmonary carcinoid tumors, which account for 1–2% of all lung cancers with approximately 2000–4500 newly diagnosed cases each year in the United States, the combined stage categories provide useful information on outcomes for typical and atypical carcinoids
[6]. However, due to persistent overlap in combined stage and subcategories of the staging system, the usefulness of the TNM staging system, particularly in the intermediate stages, is limited for carcinoid tumors
[7].
Table 1. IASLC Lung Cancer Staging Project T, N, and M Descriptors for the TNM-8 Classification of Lung Cancer.
| T—Primary Tumor |
| Category |
Subcategory |
Descriptors |
Table 2. Stage groupings for NSCLC.
| T or M Stage |
|
N0 |
N1 |
N2 |
N3 |
| TX |
|
Primary tumor cannot be assessed, or tumor is proven by the presence of malignant cells in sputum or bronchial washings but not visualized by imaging or bronchoscopy |
| T0 |
|
No evidence of primary tumor |
| IIB |
IIIA |
IIIB |
Tis |
|
Carcinoma in situ: Tis(AIS): adenocarcinoma
Tis(SCIS): squamous cell carcinoma |
| T1 |
| T1c |
IA3 |
IIB |
IIIA |
IIIB |
|
Tumor 3 cm or less in greatest dimension, surrounded by lung or visceral pleura, without bronchoscopic evidence of invasion more proximal than the lobar bronchus (i.e., not in the main bronchus). The uncommon superficial spreading tumor of any size with its invasive component limited to the bronchial wall, which may extend proximal to the main bronchus, is also classified as T1a. |
| |
| T2 |
T2a |
IB |
IIB |
IIIA |
IIIB |
T1mi |
Minimally invasive adenocarcinoma |
| T2b |
IIA |
IIB |
IIIA |
IIIB |
|
T1a |
Tumor 1 cm or less in greatest dimension |
| T3 |
T3 |
IIB |
IIIA |
IIIB |
|
T1b |
Tumor more than 1 cm but not more than 2 cm in greatest dimension |
| IIIC |
| T4 |
T4 |
IIIA |
IIIA |
IIIB |
IIIC |
|
T1c |
Tumor more than 2 cm but not more than 3 cm in greatest dimension |
| M1 |
M1a |
IVA |
IVA |
IVA |
IVA |
T2 |
|
Tumor more than 3 cm but not more than 5 cm; or tumor with any of the following features. T2 tumors with these features are classified T2a if 4 cm or less, or if size cannot be determined; and T2b if greater than 4 cm but not larger than 5 cm.
|
| |
T2b |
Tumor more than 4 cm but not more than 5 cm in greatest dimension |
| T3 |
|
Tumor more than 5 cm but not more than 7 cm in greatest dimension or one that directly invades any of the following: parietal pleura (PL3), chest wall (including superior sulcus tumors), phrenic nerve, parietal pericardium; or associated separate tumor nodule(s) in the same lobe as the primary |
| T4 |
| T1 |
T1a |
IA1 |
IIB |
IIIA |
IIIB |
| |
| Tumors more than 7 cm or one that invades any of the following: diaphragm, mediastinum, heart, great vessels, trachea, recurrent laryngeal nerve, esophagus, vertebral body, carina; separate tumor nodule(s) in a different ipsilateral lobe to that of the primary |
| T1b |
IA2 |
|
| |
|
| M1b |
IVA |
IVA |
IVA |
IVA |
|
T2a |
Tumor more than 3 cm but not more than 4 cm in greatest dimension |
| M1c |
IVB |
IVB |
IVB |
IVB |
| N—Regional Lymph Nodes |
| NX |
|
Regional lymph nodes cannot be assessed |
| N0 |
|
No regional lymph node metastasis |
| N1 |
|
Metastasis in ipsilateral peribronchial and/or ipsilateral hilar lymph nodes and intrapulmonary nodes, including involvement by direct extension |
| N2 |
|
Metastasis in ipsilateral mediastinal and/or subcarinal lymph node(s) |
| N3 |
|
Metastasis in contralateral mediastinal, contralateral hilar, ipsilateral or contralateral scalene, or supraclavicular lymph node(s) |
| M—Distant Metastasis |
| M0 |
|
No distant metastasis |
| M1 |
|
Distant metastasis |
| |
M1a |
Separate tumor nodule(s) in a contralateral lobe; tumor with pleural nodules or malignant pleural or pericardial effusion. Most pleural (pericardial) effusions with lung cancer are due to tumor. In a few patients, however, multiple microscopic examinations of pleural (pericardial) fluid are negative for tumor, and the fluid is non-bloody and is not an exudate.
Where these elements and clinical judgment dictate that the effusion is not related to the tumor, the effusion should be excluded as a staging descriptor. |
| |
M1b |
Single extrathoracic metastasis in a single organ and involvement of a single distant (non-regional) node |
| |
M1c |
Multiple extrathoracic metastases in one or several organs |
Clinical staging is based on information obtained from physical examination, laboratory tests, imaging studies, and procedures (e.g., endobronchial ultrasound-guided nodal biopsy and mediastinoscopy but not from thoracotomy) performed to evaluate the scope of disease. Pathologic staging builds on clinical staging by adding information obtained upon surgical resection of the tumor, lymph nodes or metastases
[8]. Accurate imaging interpretation is crucial for evaluating the extent of disease during clinical staging as it determines prognosis and allows for the development of a treatment plan tailored to the patient’s disease. Therefore, optimal patient care requires an understanding of the TNM staging system and the strengths and limitations of current imaging modalities used in lung cancer staging.
2. T Classification
The T classification describes tumor size, degree of local invasion, and the presence and location of separate tumor lung nodules. IASLC recommends measuring the primary tumor to the nearest millimeter on contiguous 1 mm sections with lung window setting on any plane that exhibits the largest diameter. For solid and pure ground glass lung cancers, the longest diameter of the tumor is used for staging purposes
[9][10][11][9,10,11]. For part-solid lung malignancies, the long axis diameter of the solid component should be recorded, as this is thought to represent the invasive component on pathology
[9][12][9,12]. In practice, over three-quarters of radiologists in one investigation performed tumor length measurements on only the axial plane
[11]. Except for a perfect sphere, axial plane only measurement is nearly always shorter than the longest diameter
[11][13][14][11,13,14]. Numerous studies have demonstrated that by using only the axial plane to measure the longest dimension, the T category is underestimated by at least one level in 18–27% of cases
[11][13][14][11,13,14].
Statistical analysis of the TNM-8 database showed significant differences in survival for each tumor size cut point. The size thresholds included the 3 cm cut point to separate T1 from T2 tumors, with a decline in survival associated with each 1 cm increment increase
[15]. T1 tumors were categorized into three subgroups: T1a measuring 1 cm or less, T1b measuring more than 1 cm but equal to or less than 2 cm, and T1c measuring more than 2 cm but equal to or less than 3 cm
[3]. Similarly, T2 malignancies were categorized into two subgroups with T2a tumors measuring more than 3 cm and less than or equal to 4 cm, and T2b lesions measuring more than 4 cm and less than or equal to 5 cm
[3]. T3 lesions measure more than 5 cm and less than or equal to 7 cm, and T4 lesions account for malignancies greater than 7 cm.
In addition to size, tumor location and the degree of local invasion are assessed in TNM staging and have the potential to increase the T classification. T1 tumors show no invasion into the lobar or more proximal bronchi. T2 tumors include lesions that show evidence of invasion of a main bronchus regardless of the distance from the carina
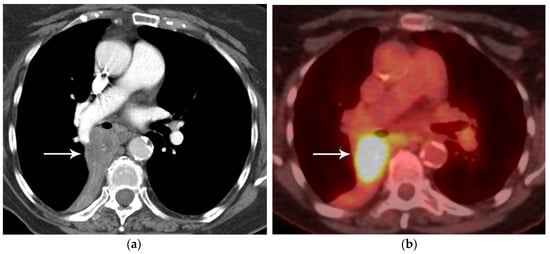
[3]. Additionally, lesions with invasion of the visceral pleura, partial or complete lung atelectasis, or pneumonitis, are classified as T2
[3] (
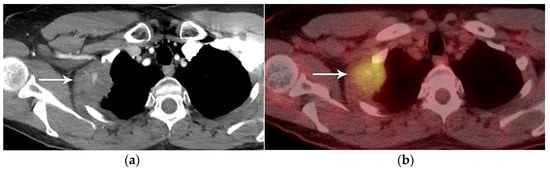
Figure 1). T3 tumors include lesions that show direct invasion of the parietal pleura, chest wall, phrenic nerve, or parietal pericardium (
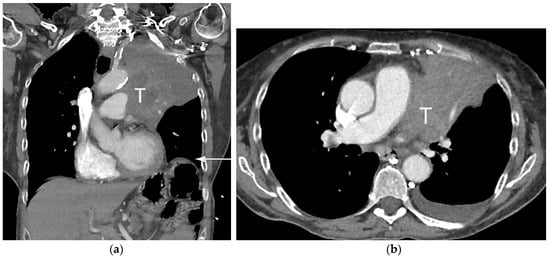
Figure 2). Lesions of any size that invade the mediastinum, diaphragm, heart, great vessels, recurrent laryngeal nerve, vertebrae, or carina are classified as T4
[3] (
Figure 3). For patients with separate tumor nodules, location is important. A separate lung nodule(s) in the same lobe as the primary tumor is considered T3. A separate lung nodule(s) in the same lung but different lobe from the primary tumor is considered T4
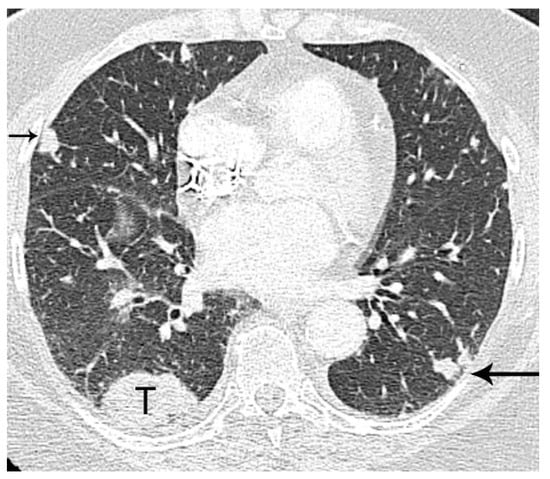
[3]. A separate nodule(s) in the contralateral lung to the primary tumor is considered intrathoracic metastatic disease M1a (
Figure 4).
Figure 1. T2 disease. (a) Contrast-enhanced CT shows right lower lobe collapse due to central obstructing tumor (arrow). (b) Axial PET/CT shows FDG avidity of the primary tumor, differentiating it from adjacent atelectatic lung. Tumor size of 3.5 cm is T2a; lobar/lung atelectasis is also T2 disease. As there is no nodal and no distant metastasis, the final stage is stage IB.
Figure 2. T3 disease. (a) Contrast-enhanced CT, and (b) axial PET/CT show the FDG-avid right upper lobe 4 cm primary tumor invading the chest wall (arrow). The size of 4 cm is T2a disease while chest wall invasion is T3 disease. With no nodal or distant metastases, the stage is IIB.
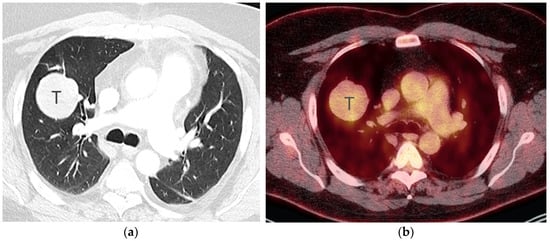
Figure 3. T4 disease. (a) Axial contrast-enhanced CT, and (b) coronal CT show 10 cm left upper lobe primary tumor (T) invading the mediastinum. Involvement of the left phrenic nerve resulted in elevation of the left hemidiaphragm (arrow). Involvement of the phrenic nerve is T3 disease. However, both size of greater than 7 cm and mediastinal invasion are T4 descriptors, dictating the T classification in this case.
Figure 4. M1a disease, intrathoracic metastasis. Contrast-enhanced CT shows a 4 cm primary tumor (T) in the right lower lobe. Separate nodule in the right middle lobe (short arrow) as the primary tumor is T4 disease. Separate nodule (long arrow) in the left lower lobe (contralateral lung) as the primary tumor is M1a disease.
FDG PET/CT, a combination of anatomical and functional imaging, is widely used in the staging of lung cancer. One benefit is the detection of recurrent laryngeal nerve involvement (T4), which manifests as ipsilateral vocal cord paralysis. In patients with recurrent laryngeal nerve involvement who are talking either before or during the PET/CT scan, there is FDG uptake in the normal vocal cord and lack of FDG uptake in the paralyzed cord. Another benefit of the functional data provided by FDG PET/CT is the ability to distinguish central obstructing primary tumors from adjacent atelectasis and post-obstructive consolidation, an imaging feature that is helpful to target the tumor for radiation therapy planning
[16] (
Figure 1).
FDG PET/CT is subject to both false negative and false positive results. False negative results can be observed with carcinoid tumors and some cases of early-stage disease (pre-invasive and minimally invasive lung adenocarcinoma)
[17] (
Figure 5 and
Figure 6). In a study of 550 patients with stage I lung adenocarcinoma, using maximal standardized uptake value (SUVmax) cutoff of 2.5 to discriminate a positive from a negative result on FGD PET/CT, 17.6% of patients had a false negative FDG PET result where the primary tumor had SUVmax of less than 2.5
[17]. Lung adenocarcinoma with a lepidic pattern on pathology have a tendency toward false negative FDG PET findings
[17]. There is evidence that focal FDG uptake correlates with tumor invasion in both pure ground-glass and part-solid malignancies, although many pre-invasive and minimally invasive adenocarcinomas may be below the resolution of PET due to their small size
[18][19][18,19]. False positive FDG PET results can be seen with nonneoplastic processes such as infections, hamartomas, granulomatous disease, sarcoidosis, amyloidosis, lung parenchymal or pleural fibrosis, and round atelectasis
[20].
Figure 5. Bronchopulmonary carcinoid. (a) CT shows a 5 cm well-circumscribed solid mass (T) in the right middle lobe. (b) Axial PET/CT shows the right middle lobe lesion (T) has low-grade FDG uptake, similar to that of the mediastinum. Biopsy showed low-grade neuroendocrine tumor.
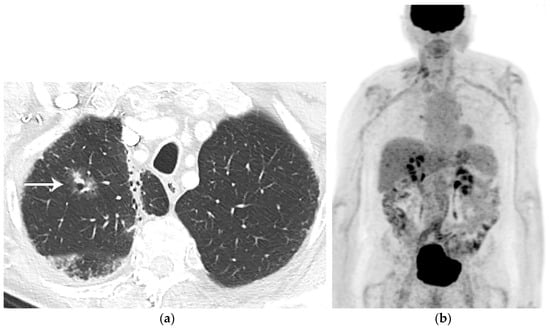
Figure 6. Lung adenocarcinoma. (a) CT shows a right upper lobe 2 cm part-solid nodule with focal “bubbly” internal lucencies and a solid component along the anterolateral aspect. Radiation fibrosis is noted in the right apex medially. (b) Whole-body PET shows the nodule is not FDG-avid. Biopsy revealed well-differentiated adenocarcinoma. Part-solid lung adenocarcinomas may not be FDG avid due to slow cell proliferation or poor cellularity.