Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 2 by Rita Xu and Version 1 by Hussam Jouhara.
Breast cancer is the most prevalent cancer and the second leading cause of death among women, primarily due to the development of deadly metastases in 25–50% of patients, resulting in an unfavorable prognosis. Consequently, there is growing interest in exploring innovative therapeutic approaches to improve clinical outcomes and enhance the quality of life for breast cancer patients.
- breast cancer
- cryogenic media
- cryosurgery
1. Introduction
Cryogenic Media and Biomedical Applications
Since its inception in 1877, cryogenics has made remarkable progress in both theory and experimentation, leading to significant advancements in the production and behavior of materials at extremely low temperatures. These advances have paved the way for various applications of cryogenic heat transfer, revolutionizing modern technology. Cryogenic media, also referred to as cryogens, now play a critical role in aerospace, healthcare, advanced manufacturing, machining methods, superconductivity, and advanced scientific research [1]. Notably, cryogenic media, such as nitrogen (N2), helium-3 (3He), argon (Ar), and oxygen (O2), have found extensive use in the biomedical sector due to their distinctive properties and material characteristics. These cryogens have boiling points of −195.79 °C, −269.96 °C, −185.85 °C, and −182.96 °C, respectively. N2 and He are particularly favored due to their inert behavior, favorable thermal properties, widespread availability, and the cost effectiveness of liquid nitrogen. Furthermore, helium-3’s ability to exist in its liquid phase at temperatures close to absolute zero makes it valuable, albeit challenging to process and store efficiently. Argon serves as an inert component in cryogenic separation units during the fractional distillation of liquid air, while oxygen, despite its reactivity, instability, and strong oxidizing features, is commercially viable and readily accessible as a cryogen [2,3][2][3]. Ongoing research efforts are focused on developing new numerical models to investigate the mechanisms of heat transfer and material behavior related to cryogens. These studies are crucial for enhancing the performance of cryogenic technologies and for exploring innovative and efficient methods of energy storage in processing and storage systems.
2. Cryobiology
The use of low temperatures in healthcare has a rich history dating back to 2500 BC in ancient Egypt, where the concept of using cold to treat injuries and inflammation originated [4]. Centuries of research and remarkable discoveries have led to the development of cryosurgery, a cutting-edge medical technique. Cryosurgery involves the use of a cryoprobe, a small vacuum-insulated tube-like tool that serves as a conduit for a cryogenic liquid, causing complete tissue destruction. It is important to note that cryosurgery, or cryoablation, should not be confused with cryotherapy, which refers to non-invasive treatments involving the application of N2 vapor or air refrigeration at temperatures around −160 °C. Cryotherapy can be applied locally or as whole-body cryotherapy (WBC), which involves briefly exposing the entire body to temperatures ranging from −110 °C to −160 °C in a chamber environment. Significant advancements in cryogenic technologies have given rise to third-generation cryosurgery systems, which operate based on the principle of temperature change accompanying gas expansion without heat exchange with the environment. These modern systems utilize intra-operative imaging in real-time to monitor the precise placement of ultra-small cryoprobes and the extent of the freezing process. This enables easier and less traumatic probe placement, greater control over treatment margins, and ensures a more uniform temperature distribution, resulting in more efficient heat transfer. By rapidly expanding argon (Ar) or nitrogen (N2) gas through the cryoprobe’s tip, these systems can achieve extreme temperature drops, freezing adjacent tissues to approximately −140 °C within seconds. This leads to the formation of an ice ball and causes cell death within approximately 3 mm beyond the margins of the ball, as illustrated in Figure 1 [5].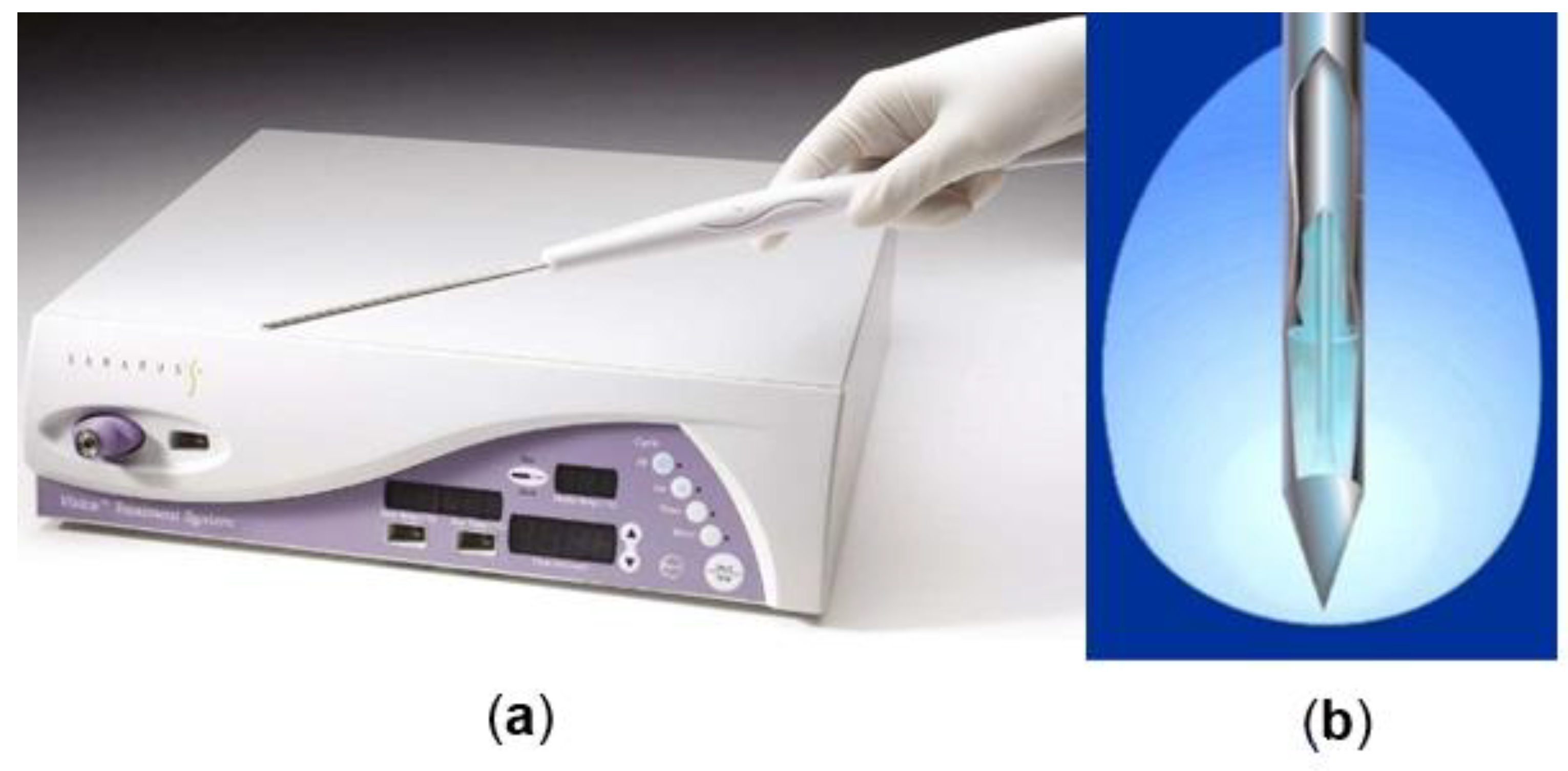
Figure 1.
(
a
) Percutaneous cryoablation probes. (
b
) Schematic representation of the active tip of a cryoablation probe and the ice ball formed.
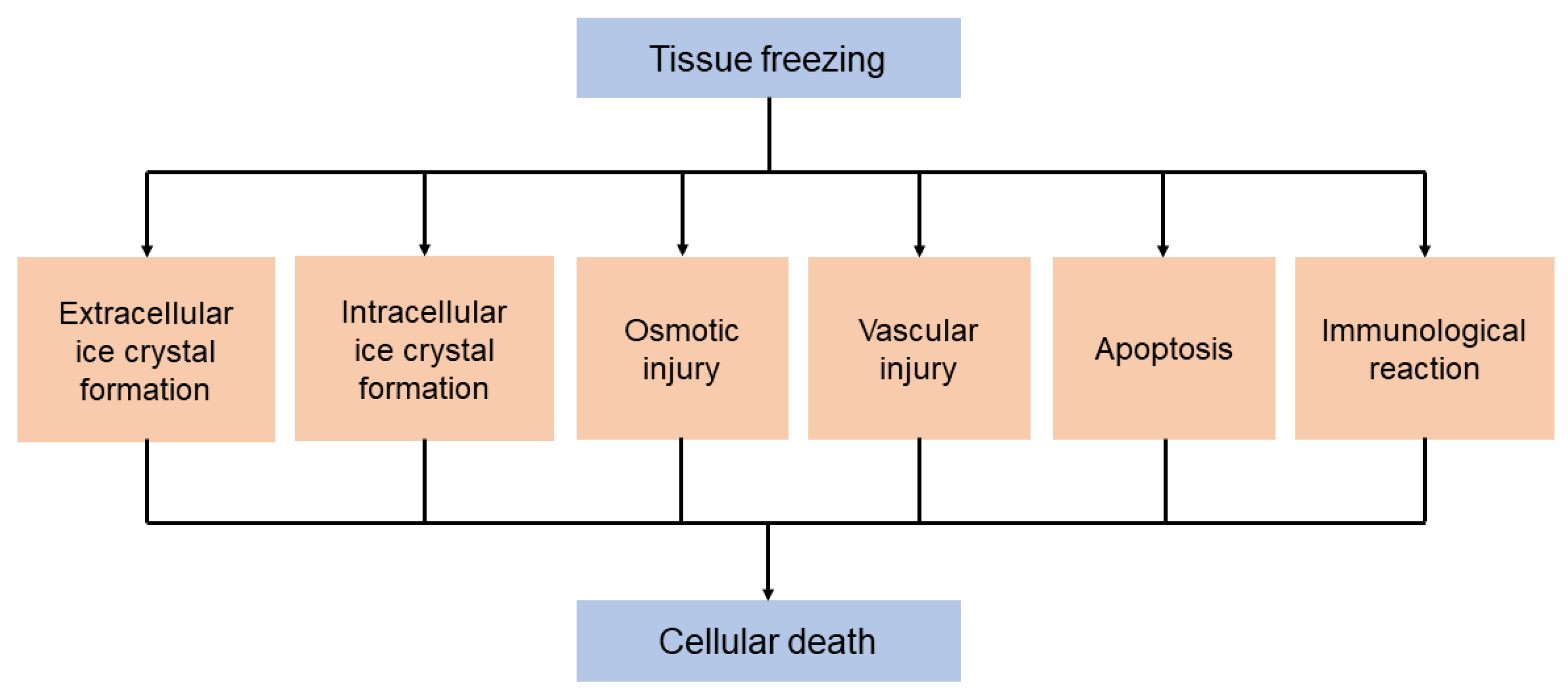
Figure 2.
Underlying pathophysiological mechanisms of the destructive effects of cryosurgery on biological tissues and the associated tissue damage.
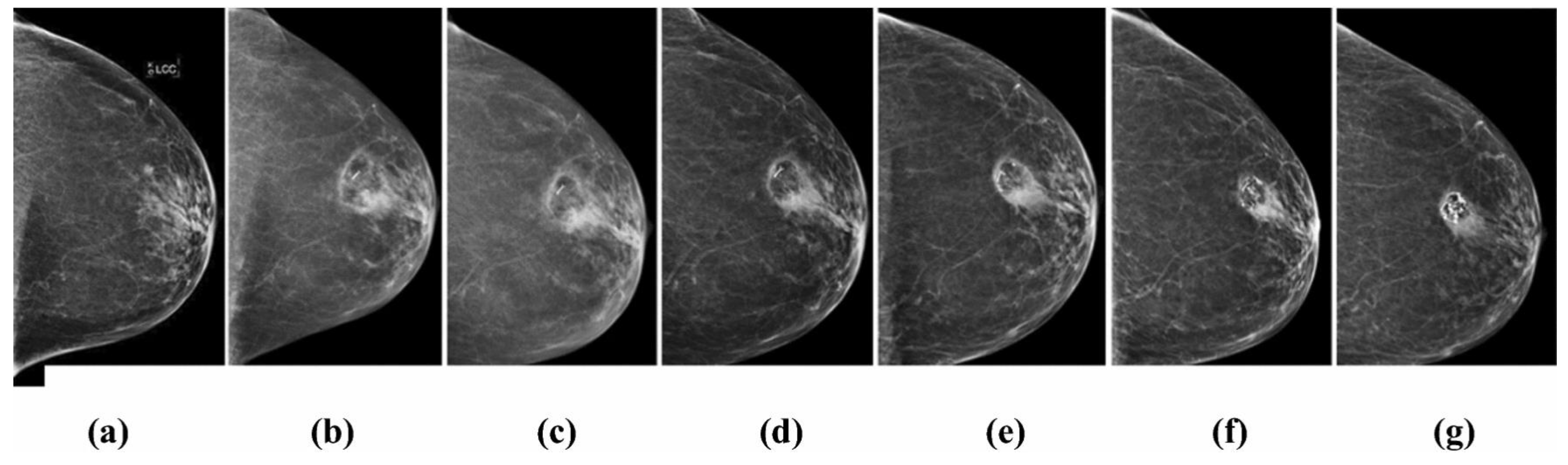
Figure 3. Mammography imaging of a left breast with a 0.5 cm invasive ductal carcinoma with tubular features demonstrating the resolving zone of fat necrosis around the area treated by cryoablation: (a) Before cryoablation; and (b) 6 months; (c) 12 months; (d) 24 months; (e) 36 months; (f) 48 months; (g) 60 months after cryoablation.
2.1. Cryosurgery and Breast Cancer
Breast cancer is currently the most common malignancy and the second leading cause of death among women, mainly due to the development of deadly metastases in 25–50% of patients, resulting in an unfavorable prognosis. Only 25% of patients have a 5-year survival rate [10][8]. Traditional surgical methods for removing the primary tumor, such as breast-conserving surgery or total mastectomy, often require general anesthesia and hospitalization, and are associated with postoperative pain and potential adverse cosmetic effects. To address these issues, minimally invasive modalities have gained significant interest. These modalities allow for the ablation of benign (e.g., fibroadenoma) or malignant breast lesions under local anesthesia in an outpatient setting. They cause minimal pain, promote quicker recovery, and result in better cosmetic outcomes with minimal tissue loss, smaller wounds, and less breast deformity. The availability of commercial liquefied gases has revolutionized modern cryosurgery, offering novel and state-of-the-art treatment options for patients with breast cancer [11,12][9][10]. Furthermore, advancements in screening and imaging technologies have led to the detection of breast cancers at earlier stages, resulting in a better prognosis with 5-year survival rates ranging from 98% to 99%. However, current treatment protocols have been associated with overtreatment and unnecessary surgical interventions, emphasizing the need to de-escalate breast cancer surgery toward less invasive approaches. The American College of Surgeons has outlined three essential criteria for any novel treatment modality: proven safety and efficacy, cost effectiveness, and at least the same effectiveness with lower morbidity compared to existing therapeutic options. Cryosurgery meets these criteria and has demonstrated feasibility, tolerance, and effectiveness in destroying breast tumors. It offers a simple procedure with low morbidity, reduced or absent pain, and cost effectiveness [11,12][9][10]. Cryosurgery not only destroys cancer cells but also induces the release of intact tumor-specific antigens into the circulation, which is vital for immune system recognition and response [13][11]. Studies have shown that cryosurgery can stimulate a tumor-specific immune response, which is reflected in the regression of metastatic lesions. The presence of higher levels of tumor-infiltrating lymphocytes (TILs) has been associated with better response rates to neoadjuvant chemotherapy and improved survival rates. Animal studies have demonstrated that cryosurgery increases immune effector cell numbers while decreasing immunosuppressive regulatory T cell (Tregs) numbers associated with tumor growth promotion. Cryosurgery is typically performed in an outpatient setting under local anesthesia, resulting in reduced sedation requirements, operating room needs, surgical complications, recovery times, and healthcare costs. Importantly, it offers an attractive alternative to surgery with better cosmetic outcomes. Unlike surgery, cryosurgery does not require excision within the breast parenchyma, which can cause breast asymmetry and compromised cosmetic results. When analyzing potential cryosurgery-associated complications, major complications are classified as Common Terminology Criteria for Adverse Events (CTCAE) grade 3 or more and minor complications as CTCAE grade 1–2. Major complications include major arterial bleeding after cryoprobe removal and skin necrosis or pectoralis muscle necrosis, and minor complications include minor bleeding, pain, minor skin freeze burns, localized edema, swelling, ecchymosis, skin induration, pruritis, mild hematoma, seroma, and nodular thickening at the cryoablation site. Meta-analyses comparing various ablation modalities, including cryoablation, radiofrequency ablation (RFA), microwave ablation (MWA), high-intensity focused ultrasound (HIFU), and laser ablation, have shown that cryoablation achieves satisfactory to excellent cosmesis in over 95% of treated patients, with lower complication rates compared with other modalities (5% vs. 18%) [14][12]. Minor adverse events associated with cryoablation, such as minor bleeding, pain during anesthetic injection, and bruising, are similar to those associated with breast needle biopsy. Large randomized controlled trials are still needed to evaluate cryoablation’s long-term benefits, considering factors such as breast density category or the biological subtype of the tumor in terms of treatment response. Alternatively, cryoablation can be utilized as a salvage method for treating local recurrence following conservation therapy. However, to ascertain the comparable efficacy of cryoablation to breast conservation treatment, it is crucial to conduct large-scale, multi-center randomized control studies that evaluate its long-term benefits. Interestingly, a study comparing cryosurgery with other modalities, such as radiofrequency ablation (RFA), microwave ablation (MWA), and radiation therapy, discovered that ultra-low temperatures induced a stronger immune response. This heightened response could be attributed to the ability of heat-based techniques to cause protein denaturation and antigen damage [16,17][13][14]. Figure 4 provides a schematic representation of the cryosurgery procedure for breast cancer, illustrating the various stages from preparation to peri-operative monitoring.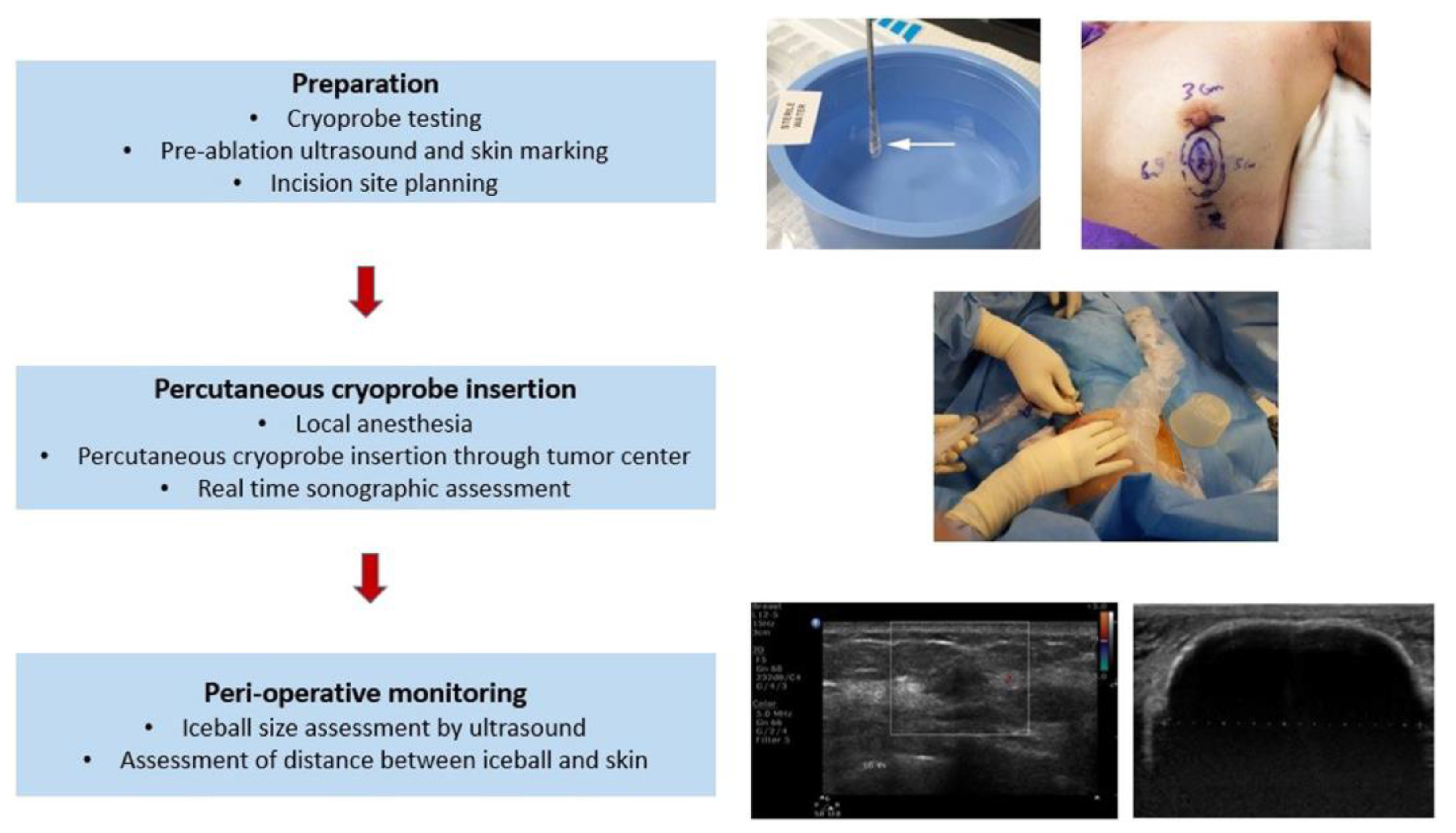
Figure 4.
Schematic representation of the cryosurgery procedure in breast cancer from preparation to peri-operative monitoring.
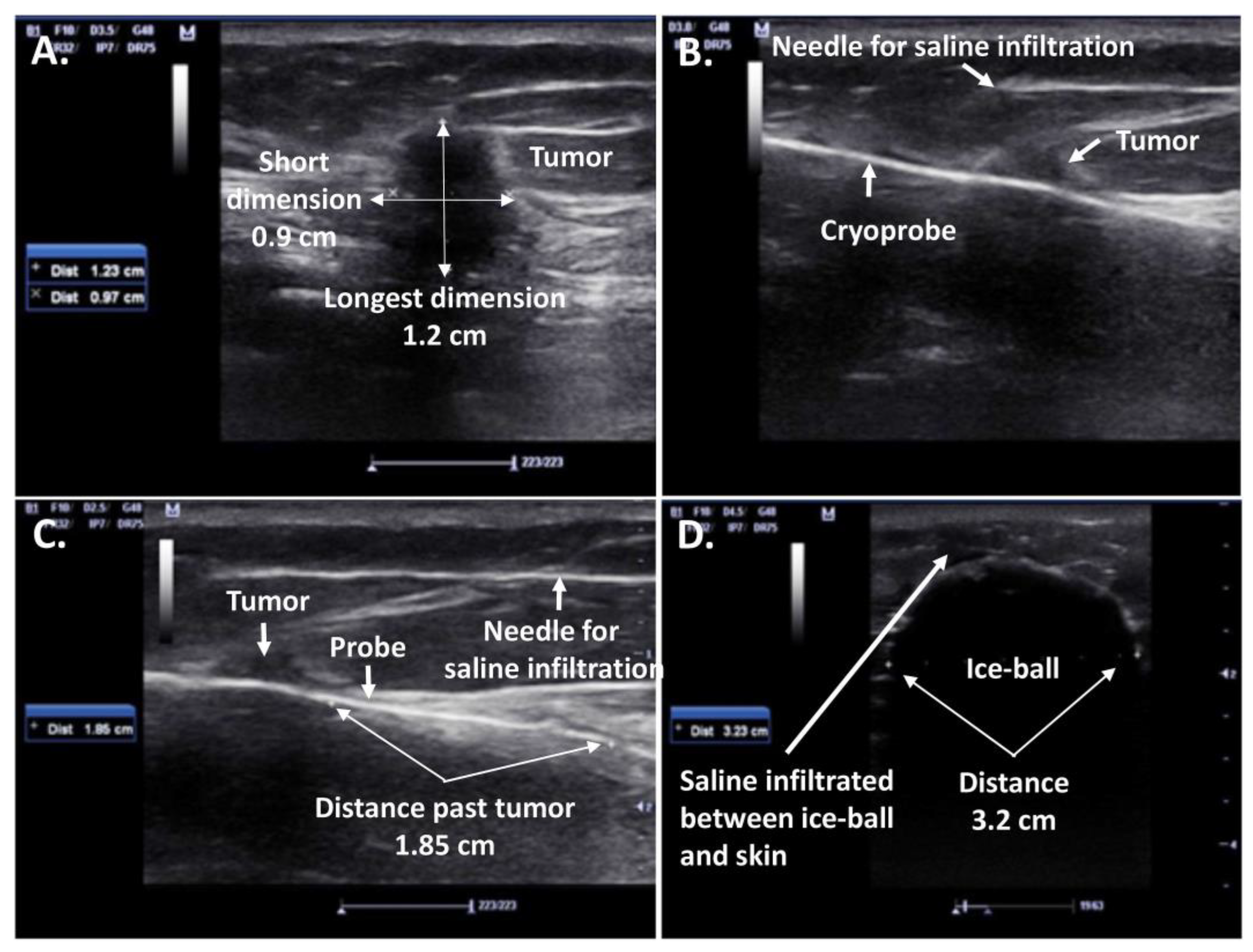
Figure 5. Ultrasound (US)-guided cryosurgery for a 1.2 cm diameter right breast IDC: (A) Size of tumor visualized by ultrasound; (B) Visualization of cryoprobe penetration hydro-dissection with saline; (C) Visualization of distance of probe projection past the tumor; (D) Transverse dimension of the ice-ball (3.2 cm) completely engulfing the transverse dimension of the tumor (0.9 cm), generating at least a 1 cm safety freeze margin on either side of the tumor.
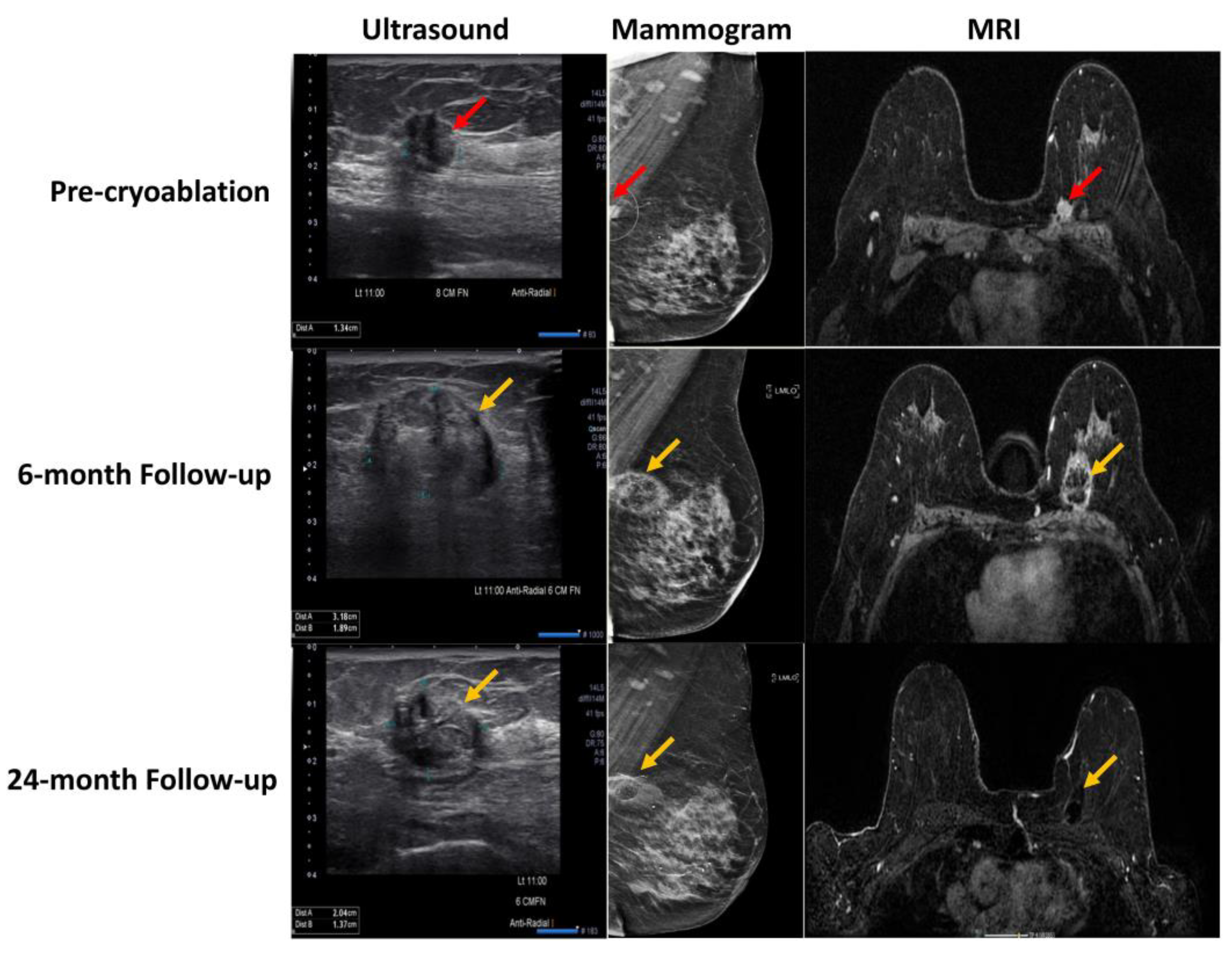
Figure 6. Pre-cryoablation and post-cryoablation imaging at the 6- and 24-month timepoint by US, mammogram, and MRI of a patient with invasive ductal carcinoma (red arrow) in the left breast and an identified area of fat necrosis (yellow arrow).
2.2. Cryosurgery Potential in Metastatic Breast Cancer
To date, the majority of cryosurgery research has focused on patients with early-stage small breast cancers, while its application in patients with metastatic breast cancer remains limited. The therapeutic options for metastatic breast cancer, also known as stage IV breast cancer that has spread to other organs such as the bones, liver, brain, and lungs, depend on various factors, including the patient’s estrogen receptor (ER) or human epidermal growth factor receptor 2 (Her2) status, gene mutations, metastatic locations, previous treatments, and involve systemic drugs and local and regional treatments, including surgery, chemotherapy, targeted biological therapy, immunotherapy, and/or radiation therapy. Recent evidence suggests that locoregional treatment of primary breast cancer after primary systemic therapy in patients with stage IV disease improves overall survival [33][21]. While lumpectomy has shown survival benefits for selected patients, resection of the primary tumor could remove potential tumor stem-cell sources that support distant metastases by different neoplastic cell lines. However, surgery may also expose the patient to surgical complications and delay systemic treatment [34][22]. Locoregional therapy of the primary tumor in de novo stage IV breast cancer has been reported to improve overall survival (OS) and reduce mortality risk [33,35,36,37][21][23][24][25]. Nevertheless, due to the limited research and conflicting studies, cryosurgery, as a minimally invasive modality with potential antitumoral immune effects, has gained relevance for patients with stage IV metastatic disease. Cryosurgery may play a role in controlling the development of metastases. A retrospective study by Niu et al. [10][8] analyzed the therapeutic effects of cryosurgery in combination with other therapies such as immunotherapy and chemotherapy in metastatic patients after failed radical surgery and reported the highest median OS of 83 months in the cryo-immunotherapy group, highlighting the overall beneficial effect of cryosurgery when used in conjunction with other treatment modalities. Furthermore, a retrospective study by Pusceddu et al. [38][26] demonstrated that cryoablation of primary advanced breast cancers in patients with bone metastatic ductal invasive breast lesions, who had previously received systemic therapy, is an effective, feasible, and well-tolerated treatment option. Complete regression was achieved in 88% of patients, but further large-scale studies are warranted. Supporting this perspective, Pusceddu et al. [39][27] also demonstrated the safety and efficacy of cryoablation when ablating primary tumors in stage IV breast cancer patients, achieving complete tumor necrosis in 85.7% of patients at the 2-month follow-up and 100% at the 6-month follow-up. However, given that the study, like almost all breast ablation studies, was retrospective in nature, prospective well-designed studies comparing cryoablation with other treatment options in metastatic breast disease are essential for a deeper understanding of the role of cryosurgery in this subgroup of patients and its potential survival benefits.References
- Jouhara, H.; Chauhan, A.; Guichet, V.; Delpech, B.; Abdelkarem, M.A.; Olabi, A.G.; Trembley, J. Low-Temperature Heat Transfer Mediums for Cryogenic Applications. J. Taiwan Inst. Chem. Eng. 2023, 2023, 104709.
- Ershov, B.G. Radiation-Chemical Decomposition of Seawater: The Appearance and Accumulation of Oxygen in the Earth’s Atmosphere. Radiat. Phys. Chem. 2020, 168, 108530.
- Park, D.H.; Park, J.J.; Olawuyi, I.F.; Lee, W.Y. Quality of White Mushroom (Agaricus Bisporus) under Argon- and Nitrogen-Based Controlled Atmosphere Storage. Sci. Hortic. 2020, 265, 109229.
- Bouganim, N.; Freiman, A. History of Cryotherapy. Dermatol. Online J. 2005, 11.
- Ullrick, S.R.; Hebert, J.J.; Davis, K.W. Cryoablation in the Musculoskeletal System. Curr. Probl. Diagn. Radiol. 2008, 37, 39–48.
- Mohammed, A.; Miller, S.; Douglas-Moore, J.; Miller, M. Cryotherapy and Its Applications in the Management of Urologic Malignancies: A Review of Its Use in Prostate and Renal Cancers; Elsevier: Amsterdam, The Netherlands, 2014; Volume 31.
- Yiu, W.K.; Basco, M.T.; Aruny, J.E.; Cheng, S.W.K.; Sumpio, B.E. Cryosurgery: A Review. Int. J. Angiol. 2007, 16, 1–6.
- Niu, L.; Mu, F.; Zhang, C.; Li, Y.; Liu, W.; Jiang, F.; Li, L.; Liu, C.; Zeng, J.; Yao, F.; et al. Cryotherapy Protocols for Metastatic Breast Cancer after Failure of Radical Surgery. Cryobiology 2013, 67, 17–22.
- Kaufman, C.S.; Rewcastle, J.C. Cryosurgery for Breast Cancer. Technol. Cancer Res. Treat. 2004, 3, 165–175.
- Tarkowski, R.; Rzaca, M. Cryosurgery in the Treatment of Women with Breast Cancer-a Review. Gland Surg. 2014, 3, 88–93.
- Olagunju, A.; Forsman, T.; Ward, R.C. An Update on the Use of Cryoablation and Immunotherapy for Breast Cancer. Front. Immunol. 2022, 13, 1026475.
- van de Voort, E.M.F.; Struik, G.M.; Birnie, E.; Moelker, A.; Verhoef, C.; Klem, T.M.A.L. Thermal Ablation as an Alternative for Surgical Resection of Small (≤2 Cm) Breast Cancers: A Meta-Analysis. Clin. Breast Cancer 2021, 21, e715–e730.
- Abdo, J.; Cornell, D.L.; Mittal, S.K.; Agrawal, D.K. Immunotherapy Plus Cryotherapy: Potential Augmented Abscopal Effect for Advanced Cancers. Front. Oncol. 2018, 8, 1.
- Mehta, A.; Oklu, R.; Sheth, R.A. Thermal Ablative Therapies and Immune Checkpoint Modulation: Can Locoregional Approaches Effect a Systemic Response? Gastroenterol. Res. Pract. 2016, 2016, 9251375.
- Roubidoux, M.A.; Sabel, M.S.; Bailey, J.E.; Kleer, C.G.; Klein, K.A.; Helvie, M.A. Small (<2.0-Cm) Breast Cancers: Mammographic and US Findings at US-Guided Cryoablation—Initial Experience1. Radiology 2004, 233, 857–867.
- Rabin, Y.; Julian, T.B.; Olson, P.; Taylor, M.J.; Wolmark, N. Long-Term Follow-Up Post-Cryosurgery in a Sheep Breast Model. Cryobiology 1999, 39, 29–46.
- Ward, R.C.; Lourenco, A.P.; Mainiero, M.B. Ultrasound-Guided Breast Cancer Cryoablation. Am. J. Roentgenol. 2019, 213, 716–722.
- Sabel, M.S.; Kaufman, C.S.; Whitworth, P.; Chang, H.; Stocks, L.H.; Simmons, R.; Schultz, M. Cryoablation of Early-Stage Breast Cancer: Work-in-Progress Report of a Multi-Institutional Trial. Ann. Surg. Oncol. 2004, 11, 542–549.
- Simmons, R.M.; Ballman, K.V.; Cox, C.; Carp, N.; Sabol, J.; Hwang, R.F.; Attai, D.; Sabel, M.; Nathanson, D.; Kenler, A.; et al. A Phase II Trial Exploring the Success of Cryoablation Therapy in the Treatment of Invasive Breast Carcinoma: Results from ACOSOG (Alliance) Z1072. Ann. Surg. Oncol. 2016, 23, 2438.
- Kwong, A.; Co, M.; Fukuma, E. Prospective Clinical Trial on Expanding Indications for Cryosurgery for Early Breast Cancers. Clin. Breast Cancer 2023, 23, 363–368.
- Gera, R.; Chehade, H.E.L.H.; Wazir, U.; Tayeh, S.; Kasem, A.; Mokbel, K. Locoregional therapy of the primary tumour in de novo stage IV breast cancer in 216,066 patients: A meta-analysis. Sci. Rep. 2020, 10, 2952.
- Patrick, J.; Khan, S.A. Surgical Management of de Novo Stage IV Breast Cancer. JNCCN J. Natl. Compr. Cancer Netw. 2015, 13, 487–493.
- Kolben, T.; Kolben, T.M.; Himsl, I.; Degenhardt, T.; Engel, J.; Wuerstlein, R.; Mahner, S.; Harbeck, N.; Kahlert, S. Local Resection of Primary Tumor in Upfront Stage IV Breast Cancer. Breast Care 2016, 11, 411–417.
- Lang, J.E.; Tereffe, W.; Mitchell, M.P.; Rao, R.; Feng, L.; Meric-Bernstam, F.; Bedrosian, I.; Kuerer, H.M.; Hunt, K.K.; Hortobagyi, G.N.; et al. Primary Tumor Extirpation in Breast Cancer Patients Who Present with Stage IV Disease Is Associated with Improved Survival. Ann. Surg. Oncol. 2013, 20, 1893–1899.
- Ruiterkamp, J.; Ernst, M.F.; van de Poll-Franse, L.V.; Bosscha, K.; Tjan-Heijnen, V.C.G.; Voogd, A.C. Surgical Resection of the Primary Tumour Is Associated with Improved Survival in Patients with Distant Metastatic Breast Cancer at Diagnosis. Eur. J. Surg. Oncol. 2009, 35, 1146–1151.
- Pusceddu, C.; Sotgia, B.; Amucano, G.; Fele, R.M.; Pilleri, S.; Meloni, G.B.; Melis, L. Breast Cryoablation in Patients with Bone Metastatic Breast Cancer. J. Vasc. Interv. Radiol. 2014, 25, 1225–1232.
- Pusceddu, C.; Melis, L.; Ballicu, N.; Meloni, P.; Sanna, V.; Porcu, A.; Fancellu, A. Cryoablation of Primary Breast Cancer in Patients with Metastatic Disease: Considerations Arising from a Single-Centre Data Analysis. BioMed Res. Int. 2017, 2017, 3839012.
More