Eleven歯科矯正用アンカースクリュー original articles with orthodontic anchoring screws (OASs) placement in humans including insertion torque (IT) and success rate were selected and were used to evaluate the relationships among IT, success rates, screw design, and placement methods at different sites. The ITs and success rates ranged from (OAS) の最適な挿入トルク (IT) は、OAS の特徴と挿入方法によって異なるという仮説が立てられました。IT と成功率は、上部頬側歯槽領域と下部頬側歯槽領域でそれぞれ 6.0 ± 3.2 to~ 15.7 ± 2.3 Ncm and from 62.5 to、62.5 ~ 100.0% in the upper and lower buccal alveolar areas, respectively. For the mid-palatal area, the range was の範囲でした。口蓋中央部の範囲は、それぞれ 14.5 ± 1.6 to~ 25.6 ± 5.5 Ncm andおよび 83.0 to~ 100.0%, respectively. ITs of 5–12 and 6–14 Ncm were found to be optimal for the commonly used φ1.5– でした。一般的に使用される φ1.5 ~ 1.7 mm OASs in the upper and lower interproximal areas, respectively. In the mid-palatal suture area, ITs of 11–16 and 20–25 Ncm were considered suitable for tapered の OAS では、上部歯間領域と下部歯間領域でそれぞれ 5 ~ 12 および 6 ~ 14 Ncm の IT が最適であることがわかりました。口蓋中央縫合領域では、テーパー付き φ1.5 mm andおよび φ2.0 mm OASs, respectively. Although identified optimal IT ranges deserve the recommendations, care must be taken to monitor the IT during placement constantly. には、それぞれ 11 ~ 16 Ncm および 20 ~ 25 Ncm の IT が適していると考えられました。特定された最適な IT 範囲は推奨に値しますが、配置中は常に IT を監視するように注意する必要があります。
- orthodontic anchoring screw
- orthodontic mini-implant
- temporary anchorage device (TAD)
- placement torque
- insertion torque
- success rate
1. Introductionはじめに
2. Maternal Trait Mindfulness and Social Competence of Preschoolers歯科矯正用アンカースクリューの配置に最適な挿入トルク
2.1. Placement Methods (Self-Drilling or Self-Tapping)
2.2. Shapes and Dimensions of OASs
2.2.1. Tapered and Cylindrical OASs
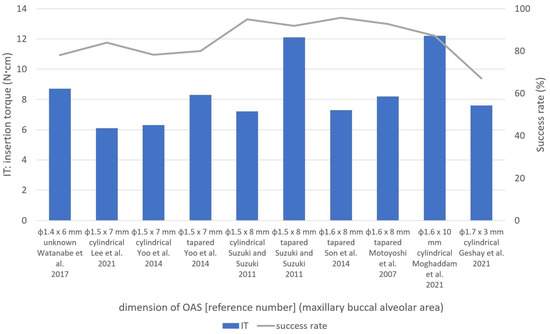
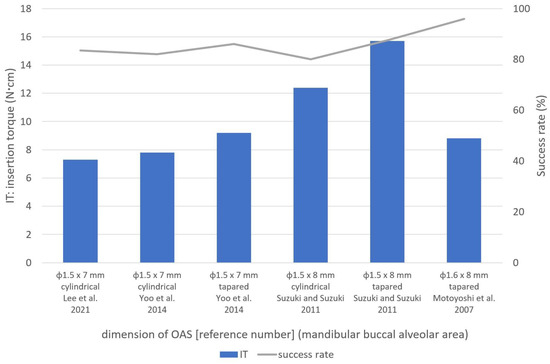
Yooユら。[ et13 al.] [13] compared taperedは、テーパー型と円筒型のセルフドリリング and cylindrical self-drilling φ1.5 × 7 mm OASs and reported significantly higher ITs in tapered OASs (8.3 ± 3.7 を比較し、上顎頬側歯槽領域において円筒型 OAS (6.3 ± 2.8 Ncm) than in cylindrical OASs (6.3 ± 2.8よりもテーパー型 OAS (8.3 ± 3.7 Ncm) in the maxillary buccal alveolar area. They reported noの方が有意に高い IT を報告しました。彼らは成功率に有意差はないと報告した [ significant13 differences in success rates [13].]。 Suzukiスズキとスズキ and[ Suzuki15 [15]] usedは、同じ寸法(頬側歯槽領域では tapered (self-drilling) and cylindrical (self-tapping) OASs of the same dimension (φ1.5 × 8 mm in the buccal alveolar area, and 、口蓋中央部では φ1.5 × 6 mm in the mid-palatal suture area), and found that tapered OASs had higher ITs (12.1 ± 3.1 Ncm, 15.7 ± 2.3 Ncm, and 21.1 ± 2.2 Ncm, respectively) than cylindrical OASs (7.2 ± 1.4 Ncm, 12.4 ± 1.2 Ncm, and 14.5 ± 1.6 Ncm) in all)のテーパー型(セルフドリリング)および円筒型(セルフタッピング)OAS を使用しました。縫合部)、テーパ状 OAS の IT が円筒形 OAS(7.2 ± 1.4 Ncm、12.4 ± 1.2 Ncm、14.5 ± 1.6 Ncm)よりも高いことがわかりました(それぞれ 12.1 ± 3.1 Ncm、15.7 ± 2.3 Ncm、21.1 ± 2.2 Ncm)。 ) すべてのサイトにあります [ sites15 [15].]。 In an in vitro study, 研究で、Assad-Loss etらは、[ al.16 [16]] evaluatedは、いくつかの the fracture torques for several OAS designsOAS 設計 (φ1.5– ~ 1.6 × 6– ~ 7 mm) andの破壊トルクを評価し、結果に最も影響を与える特性は内径と外径の比であると報告しました。クーニャら。[ reported17 that] the characteristic that most influenced the results was the ratio between the internal and external diameters. Cunha et al. [17] compared ITs in tapered and cylindrical は、低密度および高密度の牛骨を使用してテーパー型と円筒型の φ1.6 × 8 mm OASs using low- and high-density bovine bone and reported that tapered OASs had higher ITs than cylindrical OASs in the high-density bone,の IT を比較し、高密度骨ではテーパー型 OAS の方が円筒型 OAS より IT が高いと報告しましたが、低密度骨 [ but17 there were no significant differences in the low-density bone [17]. ]。2.2.2. OAS Dimensionsの寸法
AChen らによるin vitro研究。[ study21 by] Chen et al.は、密度 20、30、および 40 [18] examined the mepchanicalf properties of の人工骨を使用した φ1.3 × 7 mm OASs (self-drilling) using artificial bone with densities of 20, 30, and 40 pcf, and reported ITs of 3.9, 5.2, and (セルフドリリング) の機械的特性を調査し、それぞれ 3.9、5.2、および 10.0 Ncm, respectively. の IT を報告しました。
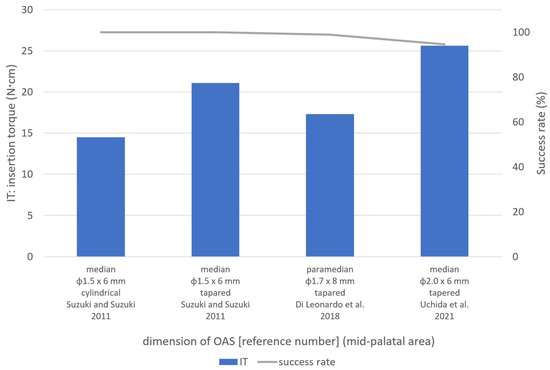
Large ある研究で口蓋中央縫合領域に使用された大型のφ2.0 × 6 mm OASs used in one study in the mid-palatal suture area had a success rate of は、94.5% and the highest ITsの成功率と最高の IT (25.6 ± 5.5 Ncm) [8].を示しました An[8] in(図4 vitro study by )。Nienkemper らによる et al.in vitro 研究。[ 23 [19]] evaluatedはブタの骨盤を使用して φ2.0 × 9 mm OASs using pig pelvic bone and reported that the ITs for insertion depths of 4 mm, 5 mm, and 6 mm were を評価し、挿入深さ 4 mm、5 mm、および 6 mm の IT が 15.4 ± 7.0 Ncm, 、26.2 ± 10.4 Ncm, and 、および 27.2 ± 14.1 Ncm, respectively. Considering であると報告しました。それぞれ。これらの結果 [ these23 results] [19], the high ITs of を考慮すると、φ2.0 × 6 mm OASs [8]の高い mayIT be[ appropriate8 for] regions with high-density bone, such as the mid-palatal suture area.は、口蓋中央縫合部などの高密度骨領域に適している可能性があります。
2.3. Placement Location
2.3. 設置場所
2.3.1. Buccal Alveolar Area頬歯槽領域
The頬側歯槽領域は、手順が簡単で固定が有利であるため、歯科矯正診療において buccal alveolarOAS が頻繁に設置される部位です。本吉ら。[ area7 is] a frequent site for OAS placement in orthodontic practice because of the simplicity of the procedureは、φ1.6 mm OAS の成功率を向上させるために 5 ~ 10 Ncm の IT を推奨しました。この領域[ 1、6、7、8、9、10、11、12、13、14、15 and]では直径 advantageous anchorage. Motoyoshi et al. [7]1.3 ~ 1.7 recommended が使用されているため、さまざまな条件に対する参照ITs範囲が望ましいと考えられます。 これらの研究に基づいて、この領域ではφ1.5〜1.7 ofmmのOASが一般的に使用され、上部および下部頬歯槽領域の円筒形OASにはそれぞれ5〜8 5–10 Ncm to improve the success rate of φ1.6 mmNcmおよび6〜12 NcmのITが最適でした。テーパー付き OAS の場合、IT は 6 ~ 12 Ncm および 8 ~ 15 Ncm が最適です。2.3.2. 口蓋中央部
口蓋中央領域への OASs. As diametersの配置は、前歯の後退や上顎弓における臼歯の侵入、遠位化、突出など、さまざまな目的に使用されます [28 of]。この領域への 1.3–1.7OAS mm wereの配置は、解剖学的にも隣接歯間領域よりも好ましいと考えられています [ used29 ]。ただし、Naya-Imainらによって報告されているように。[ 30 this]、成人でも縫合糸の閉鎖が不完全である可能性があるため、OAS area留置前にコーンビーム [1][6][7][8][9][10][11][12][13][14][15],CT aなどの適切な画像診断を使用して口蓋正中縫合糸の縫合深さを考慮する必要があります。この点に関して、彼らは、未縫合領域への挿入を防ぐために、口蓋中央縫合糸での reference OAS の留置は年齢に関係なく避けるべきであると結論付けました。 口蓋中央領域は、特に正中縫合糸に近い皮質が厚いため、IT range制御のために for variousOAS を配置する前に事前のドリリングが必要になることがよくあります[ conditions8、15 would]。スズキおよびスズキ be[ desirable. Based15 on] these studies, φ1.5–1.7 mm OASs were commonly used は、この領域で円筒形とテーパ状の OAS (φ1.5 mm) の両方を使用し、前者の方が IT が低いと報告しました。円筒形 OAS の IT と成功率は、それぞれ 14.5 ± 1.6 Ncm と 100.0% でした。 in vithis area, andro 研究では、Wilmes et al. [ ITs26 of] 5–は、φ1.5 mm およびφ2.0 mm OAS の破断時の最大トルクがそれぞれ 20.1 ± 3.8 Ncm and 6–12 Ncm were optimal for cylindricalおよび 49.2 ± 7.5 Ncm であると報告しています。Dalla Rosaらによるin vitro研究では、[ 27 ]、φ1.5 mm OASs in the upper and lower buccal alveolarの破壊までの降伏トルクは 16.3 ± 1.6 Ncm でした。これらの研究に基づいて、スズキおよびスズキ [ 15 areas, respectively]によって報告されたφ1. For tapered OASs, ITs of 6–15 mm OAS の IT 21.1 ± 2.2 Ncm and 8–1は降伏トルクを超えました。したがって、口蓋中央縫合部には、IT が 20 ~ 25 Ncm were most suitableの φ2.0 mm テーパー OAS の使用が適していると考えられます。2.3.2. Mid-Palatal Area
OAS placement in the mid-palatal area is used for various purposes, such as the retraction of anterior teeth and intrusion, distalization, and protraction of molars in the maxillary arch [20]. OAS placement in this area is also considered anatomically more favorable than the interproximal area [21]. However, as reported by Naya-Imai et al. [22], the sutured depth of mid-palatal suture should be considered using adequate imaging, such as cone-beam computed tomography, before OAS placement because there could be incomplete suture closure even in adults. Concerning this matter, they concluded that the OAS placement in mid-palatal sutures should be avoided regardless of age to prevent the insertion into unsutured areas.
The mid-palatal area has a thicker cortex, especially close to the median suture, which often requires pre-drilling before OAS placement for IT control [8][15]. Suzuki and Suzuki [15] used both cylindrical and tapered OASs (φ1.5 mm) in this area and reported lower ITs for the former. Cylindrical OASs had ITs and success rates of 14.5 ± 1.6 Ncm and 100.0%, respectively.
In an in vitro study, Wilmes et al. [23] reported that the maximum torques at the time of fracture for φ1.5 mm and φ2.0 mm OASs were 20.1 ± 3.8 Ncm and 49.2 ± 7.5 Ncm, respectively. In an in vitro study by Dalla Rosa et al. [24], the yield torque to fracture for φ1.5 mm OASs was 16.3 ± 1.6 Ncm. Based on these studies, the ITs of 21.1 ± 2.2 Ncm for φ1.5 mm OASs reported by Suzuki and Suzuki [15] exceeded the yield torque. Therefore, the use of φ2.0 mm tapered OASs with ITs of 20–25 Ncm is thought to be suitable in the mid-palatal suture area.
2.3.3. Infrazygomatic Crest and the Buccal Shelf Areas頬骨下縁と頬側棚領域
The infrazygomatic crest and the buccal shelf area have some clinical advantages over alveolar interproximal areas [25][26], but few studies have investigated OASs in these sites. Sreenivasagan et al. [3] investigated the ITs of OASs (φ2.0 × 12 mm) in these areas and found that the ITs and success rates at the infrazygomatic crest (12 screws) and buccal shelf (four screws) areas were 10.1 Ncm and 83.3%, and 10.3 Ncm and 100.0%, respectively. Approximately 10 Ncm IT is considered optimal in these areas, but further studies are required to investigate these placement sites.