The mobile apps can be categorized into autism support apps, educational apps, teacher training apps, parental support apps, and data collection apps. The individuals with autism spectrum disorder (ASD) are the primary users of the first two categories of apps. Teachers of children with ASD are the primary users of the teacher training apps. Parents are the primary users of the parental support apps, while individuals with ASD are usually the primary users of the data collection apps and clinicians and autism researchers are the beneficiaries. Gamification, virtual reality, and autism-specific mechanisms have been used to improve the usability of the apps. User-centered design is the most popular approach for mobile app development. Augmentative and alternative communication, video modeling, and various behavior change practices have been used as the theoretical foundation for intervention efficacy.
- autism
- mobile apps
- smartphones
- user-centered design
- augmentative and alternative communication
- video modeling
- virtual reality
1. Introduction
2. The Primary Beneficiaries of the Mobile Apps
The taxonomy of the mobile apps and their beneficiaries are shown in Figure 21. Scholars categorize the mobiles apps into five types: (1) autism support apps; (2) educational apps; (3) parental support apps; (4) teacher training apps; and (5) data collection apps. The individuals with autism spectrum disorder (ASD) are further divided into children, adolescents (i.e., young adults), college students, and adults. Individuals with ASD are the primary users and beneficiaries of autism support apps and educational apps. Parents and teachers may be the secondary users of the autism support apps to provide content and customize the apps. Educational apps may also allow the teachers to configure and customize the apps as the secondary users. Educational apps are typically used in a classroom setting under the guidance of teachers.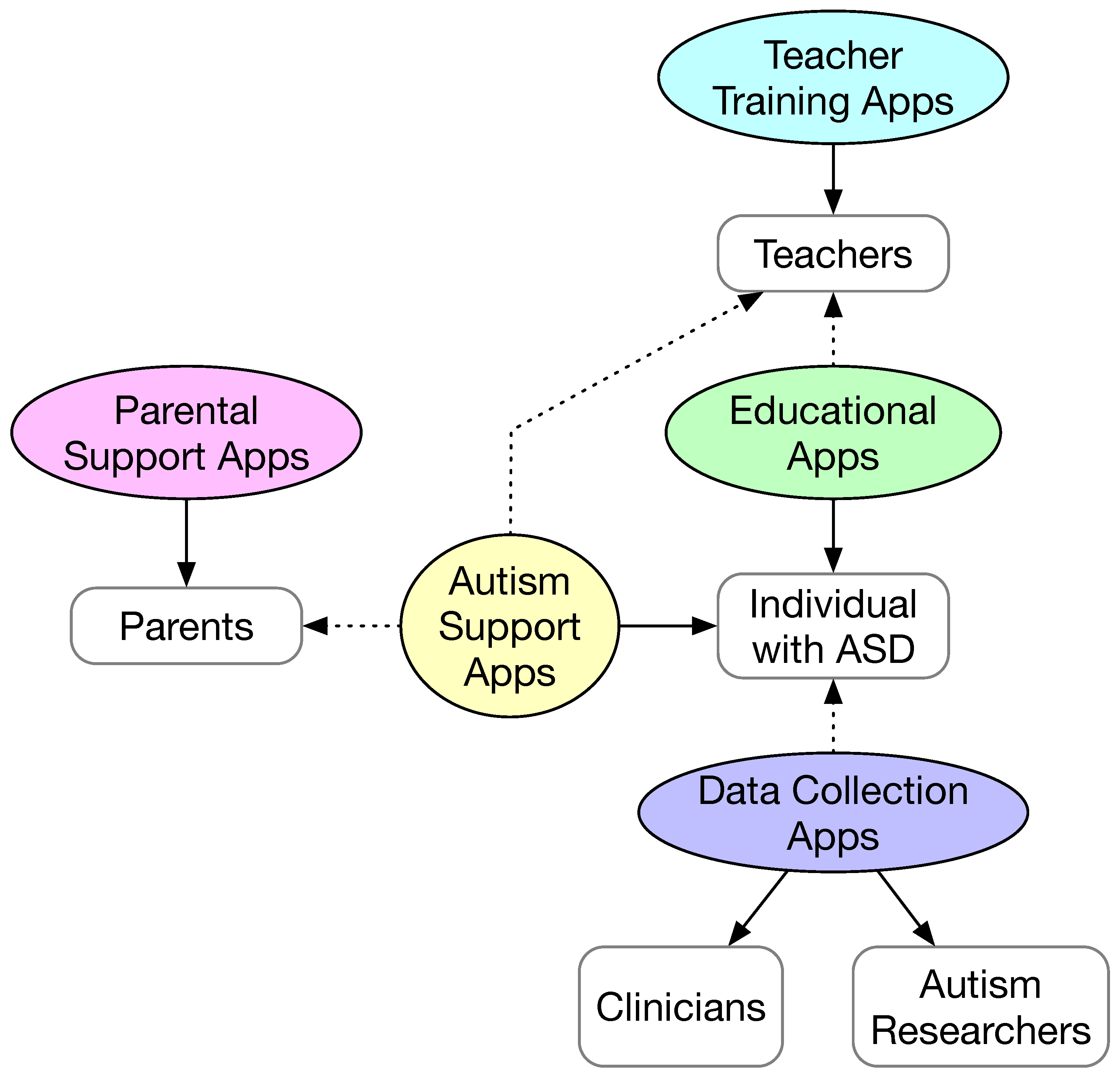
3. The Primary Purposes of the Mobile Apps
3.1. Parental Support Apps
3.2. Teacher Training Apps
In [5], the Map4speech mobile app was used to train teachers in a very similar fashion to the authors’ earlier study [6], where the app was used to train parents to improve the functional communication of their children with ASD. In [7], the usability and efficacy of a mobile app called IEP-Connect were reported. IEP in the app name stands for individualized education program. The study was conducted in the context of classroom education. The app was designed to select the most optimal motivator for teachers and therapists to use based on the recorded problematic behaviors of their students. The motivator selection is based on an applied behavior analysis and incorporates reinforcement learning. The decision making is based on Markov decision processes. The effectiveness of the motivator selected is measured by the student motivation after the selected motivator has been applied.3.3. Autism Support Apps
3.3.1. Communication and Social Interaction
In [8], a mobile app called MyCalendar was used to help children with ASD who have limited verbal skills to communicate with their teachers in schools and with their families at home. The app presents a calendar view to the users, where the children, teachers, and family members may add photos and videos to the calendar each day. The mobile app encourages the children with ASD to communicate with the teachers at school and the family members at home. The app also allows the users to annotate the photos and videos, which make the app a visual diary of the children with ASD. That said, the main goal of the app is to encourage children with ASD to communicate with their teachers and family members, and reinforce the value of social interaction and emotional bonds via replaying and modeling positive social interactions.3.3.2. Independent Living
Several mobile apps have been developed to help individuals with ASD to achieve independent living. These not only include the training of children with ASD to perform daily routines such as brushing teeth and putting on clothes, but also include the training of more demanding skills such as planning for trips and medical appointments, self-management skills, vocational skills, and adaptive skills. In [9], the design of a mobile app called AutiAct was reported. The app helps a child with ASD to learn some basic daily routines at three different difficulty levels: easy, medium, and hard. The easy level consists of the daily routines of washing their hands and face. The medium level consists of the daily routines of brushing their teeth and flushing the toilet. The difficult level consists of one daily routine of putting on shoes. For each daily routine, a training video is provided in the app. The underlying mechanisms adopted in the app are augmentative and alternative communication [10] and video modeling [11].3.4. Educational Apps
In [12], a set of criteria was developed to assess the mobile apps (limited to the Android platform) for teaching children and adolescents basic instrumental skills (oral language, reading, writing, and mathematics). The study found 88 apps (English and Spanish) from the Google Play Store. The criteria include three dimensions: design and form (availability of the app, ergonomics, usability, popularity, and accessibility), content (coverage of key elements in pronunciation, reading, writing, and math, guide on using the app, audio quality, and safety), and pedagogical aspects (interactivity, suitability of pace and learning, and assessment). Some of the criteria could provide guidance on the development of new mobile apps that target instrumental skills. However, the criteria appear to have ignored the specific needs from children and adolescents with ASD. In a similar study [13], the same research group evaluated 155 Android apps using the same set of criteria.
3.5. Data Collection Apps
Traditionally, diagnosis and assessment of symptom changes are largely based on retrospective reports from caregivers of individuals with ASD. Such an approach may introduce errors in reporting because of the necessity of recalling past behaviors of the individuals with ASD. It is much more desirable to collect data in real time or nearly real time. In [14], an observational study on caregivers’ daily reporting of autism symptoms using a web and mobile app called My JAKE (short for Janssen Autism Knowledge Engine) was reported. The caregiver is expected to first complete the medical and developmental history of the child with ASD in the app. Then, on a daily basis, the caregiver is required to complete the autism behavior inventory, which consists of 73 items that cover the symptoms and behaviors of the child with ASD. The app also allows the caregiver to log additional items using the journal and event tracker. Furthermore, the app can be connected to the Microsoft health vault. The usability of the app was evaluated using a human subject trial with 144 caregivers.4. The Mechanisms of Mobile Apps to Improve User Engagement
4.1. General Purpose Mechanisms
Gamification
Gamification refers to adding game design elements in the mobile app. Games by definition are voluntary and enjoyable. Games are a special form of play in that games are intrinsically goal-oriented and they are bound by predefined rules [15]. Another element of games is feedback. Feedback informs the player whether or not the rules are followed and whether or not the goal has been reached. The mechanics, dynamics, and aesthetics (MDA) framework has been widely adopted in game development [16]. According to the MDA framework, game design is experience driven instead of feature driven. The game itself resembles more of an artifact instead of media. The content of the game is its behavior exhibited via the interaction with a player. The relationship between game mechanics, game dynamics, and game aesthetics is illustrated in Figure 3.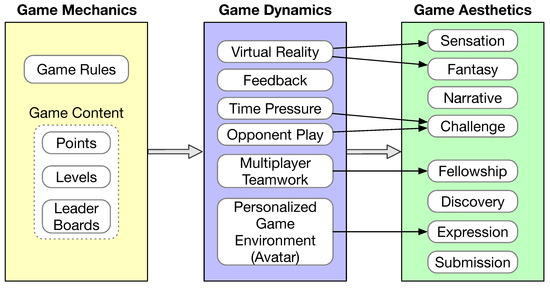
4.2. Virtual Reality
Virtual reality refers to the immersive and interactive environment of a synthetic world [17]. The synthetic world might incorporate elements of the real environment to different extents. In [17], this is referred to as a virtuality continuum. For example, the virtual reality environment may use smartphone cameras and sensors to incorporate the user’s face or movement into the virtual reality scene. That is why some publications use the term “augmented” reality. Traditionally, virtual reality is achieved via expensive 3D immersive systems such as CAVE and head-mounted goggles. Recently, devices have been made to use a smartphone in a way similar to head-mounted goggles. The Virtuoso mobile app is used in this way [18], and it was used to train adults with ASD adaptive skills. However, a virtual reality user interface does not have to be fully immersive to be effective, which has been confirmed in many autism studies [19].4.3. Autism-Specific Mechanisms
Several studies incorporated autism-specific mechanisms to improve the engagement level of the mobile apps. In [20], the app design allows the user to choose an avatar that matches their own restricted interest. As a result of the alignment with the child’s restricted interest, the mobile app (called Sidekick!) was able to maintain the motivation of the child with ASD and improve the treatment adherence in therapy sessions, schools, and at home.5. Guidelines Followed in the Mobile App Development
Three studies provided detailed processes in the design and development of the mobile app [21][22][23]. All of them followed a user-centered design (UCD) process [24]. UCD refers to a loosely defined process that has the following elements: (1) understand the users; (2) actively involve the users when defining the requirements; and (3) iterative design and evaluation. To understand the users and to discover the requirements, various instruments have been used, including questionnaires, interviews, focus groups, and observations. Ideally, the targeted individuals with ASD should be the subjects of these instruments. However, it might not be practical to directly involve children with ASD in the design process due to their disorders. Some of them might be non-verbal. As such, studies often involve parents, teachers, and therapists of the children with ASD. Experienced software developers for this type of app have also been involved [21][22]. Each of the three studies developed or followed a set of guidelines to make the app a good fit for the target autism population and for the specific application objective, as illustrated in Figure 4. The development of the PuzzleWalk app [23], which is an app promoting physical activities for adults with ASD, included ten guidelines as shown in the left column of Figure 4. The development of the SimpleTEA app [21], which is a serious mobile game for improving communication in children with ASD, considered four major perspectives: user sensitivity, user safety, user engagement, and game playability, as shown in the middle column of Figure 4. The development of the PlanTEA app [22], which is an app supporting children with ASD to attend medical appointments, was guided by the AutismGuideline proposed in [25], as illustrated in the right column of Figure 4.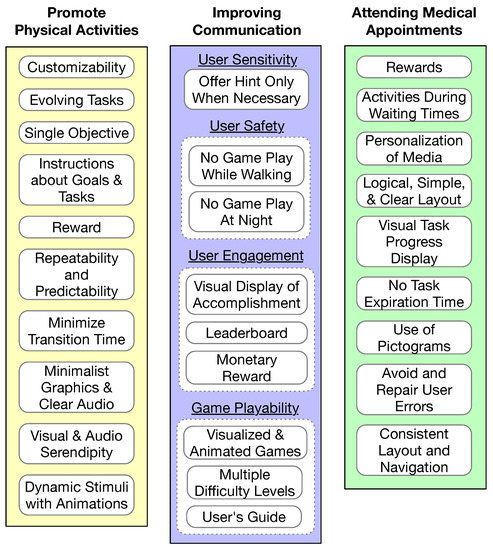
6. The Theoretical Foundations in the Mobile App Design to Ensure Intervention Effectiveness
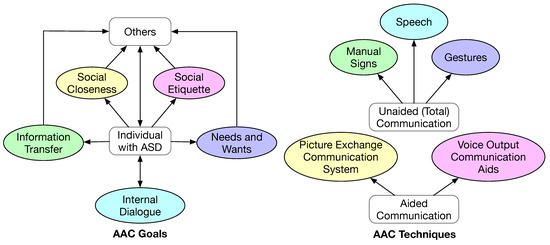
6.1. Augmentative and Alternative Communication
-
Communication of needs and wants. This is the most basic form of communication. It often involves the individual making a request to the caregiver and expecting an action-oriented response.
-
Information transfer. This form of communication entails the formulation of a coherent message. Hence, it is more complex and demanding for the individual. The ability of making this form of communication is essential for an individual to receive education, stay employed, and receive healthcare.
-
Social closeness. To establish friendship and other inter-personal relationships, sustained conversational communication is required. This is an even more demanding form of communication. In addition to coherent information, this form of communication requires the individual to express one’s emotions and to have a correct understanding of the feelings of the conversation partner.
-
Social etiquette. This form of communication is necessary for an individual to conform to social conventions of politeness, for example, the individual is supposed to express appreciation when being helped.
-
Internal dialogue. This form of communication is to communicate with oneself, which is necessary to accept oneself, to be productive daily, to perform self-reflection, and to improve oneself.
6.2. Video Modeling
Video modeling is considered a form of evidence-based practice in autism intervention [28]. Video modeling refers to using video clips to demonstrate how to complete a task or the desirable behavior in a social interaction. Video self-modeling has been used in many studies, where the learner could be video-recorded while performing a task and simulating a scenario [28]. Typically, a therapist would view the recording and provide feedback. Smartphones and tablets constitute an excellent platform for an individual to acquire various skills and to gain knowledge on proper ways of social interaction via video modeling and video self-modeling. The concept of learning via modeling is attributed to Bandura, who elaborated the role of modeling in social learning [29]. As a method for autism intervention, video modeling has been used to improve social communication skills, functional skills (for daily living), and behavioral functioning [28].6.3. Behavior Changes
6.3.1. Behavior Change Techniques

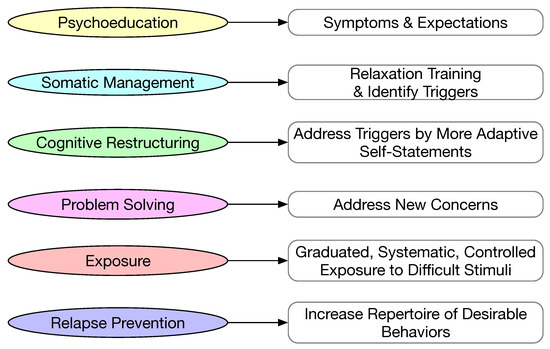
6.3.2. Cognitive Behavioral Training
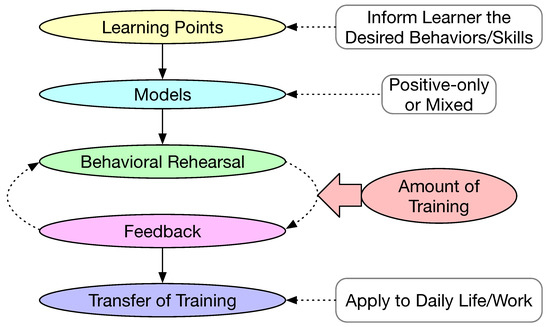
7.3.3. Behavior Modeling Training
References
- Silva, B.M.; Rodrigues, J.J.; de la Torre Díez, I.; López-Coronado, M.; Saleem, K. Mobile-health: A review of current state in 2015. J. Biomed. Inform. 2015, 56, 265–272.
- Zhao, W.; Luo, X.; Qiu, T. Smart healthcare. Appl. Sci. 2017, 7, 1176.
- Bonnot, O.; Adrien, V.; Venelle, V.; Bonneau, D.; Gollier-Briant, F.; Mouchabac, S. Mobile App for Parental Empowerment for Caregivers of Children with Autism Spectrum Disorders: Prospective Open Trial. JMIR Ment. Health 2021, 8, e27803.
- Fuller-Tyszkiewicz, M.; Richardson, B.; Little, K.; Teague, S.; Hartley-Clark, L.; Capic, T.; Khor, S.; Cummins, R.A.; Olsson, C.A.; Hutchinson, D.; et al. Efficacy of a smartphone app intervention for reducing caregiver stress: Randomized controlled trial. JMIR Ment. Health 2020, 7, e17541.
- Law, G.C.; Dutt, A.; Neihart, M. Increasing intervention fidelity among special education teachers for autism intervention: A pilot study of utilizing a mobile-app-enabled training program. Res. Autism Spectr. Disord. 2019, 67, 101411.
- Law, G.C.; Neihart, M.; Dutt, A. The use of behavior modeling training in a mobile app parent training program to improve functional communication of young children with autism spectrum disorder. Autism 2018, 22, 424–439.
- Siyam, N.; Abdallah, S. Toward automatic motivator selection for autism behavior intervention therapy. Univers. Access Inf. Soc. 2022, 1–23.
- Abdullah, M.H.L.; Wilson, C.; Brereton, M. Mycalendar: Supporting families to communicate with their child on the autism spectrum. In Proceedings of the 28th Australian Conference on Computer-Human Interaction, Launceston, Australia, 29 November–2 December 2016; pp. 613–617.
- Ahmad, W.F.W.; Zulkharnain, N.A.B. Development of a Mobile Application Using Augmentative and Alternative Communication and Video Modelling for Autistic Children. Glob. Bus. Manag. Res. 2020, 12, 1–11.
- Schlosser, R.W.; Wendt, O. Effects of augmentative and alternative communication intervention on speech production in children with autism: A systematic review. Am. J. Speech-Lang. Pathol. 2008, 17, 212–230.
- Charlop-Christy, M.H.; Le, L.; Freeman, K.A. A comparison of video modeling with in vivo modeling for teaching children with autism. J. Autism Dev. Disord. 2000, 30, 537–553.
- Gallardo-Montes, C.d.P.; Caurcel Cara, M.J.; Crisol Moya, E.; Jarque Fernández, S. Assessment of apps aimed at developing basic instrumental skills in autistic children and teenagers. Mathematics 2021, 9, 1032.
- Gallardo-Montes, C.d.P.; Caurcel Cara, M.J.; Rodríguez Fuentes, A. Technologies in the education of children and teenagers with autism: Evaluation and classification of apps by work areas. Educ. Inf. Technol. 2022, 27, 4087–4115.
- Bangerter, A.; Manyakov, N.V.; Lewin, D.; Boice, M.; Skalkin, A.; Jagannatha, S.; Chatterjee, M.; Dawson, G.; Goodwin, M.S.; Hendren, R.; et al. Caregiver daily reporting of symptoms in autism spectrum disorder: Observational study using web and mobile apps. JMIR Ment. Health 2019, 6, e11365.
- Matallaoui, A.; Hanner, N.; Zarnekow, R. Introduction to Gamification: Foundation and Underlying Theories. In Gamification: Using Game Elements in Serious Contexts; Stieglitz, S., Lattemann, C., Robra-Bissantz, S., Zarnekow, R., Brockmann, T., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 3–18.
- Hunicke, R.; LeBlanc, M.; Zubek, R. MDA: A formal approach to game design and game research. In Proceedings of the AAAI Workshop on Challenges in Game AI, San Jose, CA, USA, 25–29 July 2004; Volume 4, p. 1722.
- Milgram, P.; Kishino, F. A taxonomy of mixed reality visual displays. IEICE Trans. Inf. Syst. 1994, 77, 1321–1329.
- Schmidt, M.; Schmidt, C.; Glaser, N.; Beck, D.; Lim, M.; Palmer, H. Evaluation of a spherical video-based virtual reality intervention designed to teach adaptive skills for adults with autism: A preliminary report. Interact. Learn. Environ. 2021, 29, 345–364.
- Liu, X.; Wu, Q.; Zhao, W.; Luo, X. Technology-facilitated diagnosis and treatment of individuals with autism spectrum disorder: An engineering perspective. Appl. Sci. 2017, 7, 1051.
- Birtwell, K.B.; Platner, A.K.; Nowinski, L.A. Exploring the use of Sidekicks! For children with autism spectrum disorder (ASD). Psychol. Serv. 2019, 16, 266.
- Jaramillo-Alcázar, A.; Arias, J.; Albornoz, I.; Alvarado, A.; Luján-Mora, S. Method for the Development of Accessible Mobile Serious Games for Children with Autism Spectrum Disorder. Int. J. Environ. Res. Public Health 2022, 19, 3844.
- Hernández, P.; Molina, A.I.; Lacave, C.; Rusu, C.; Toledano-González, A. PlanTEA: Supporting Planning and Anticipation for Children with ASD Attending Medical Appointments. Appl. Sci. 2022, 12, 5237.
- Kim, B.; Lee, D.; Min, A.; Paik, S.; Frey, G.; Bellini, S.; Han, K.; Shih, P.C. PuzzleWalk: A theory-driven iterative design inquiry of a mobile game for promoting physical activity in adults with autism spectrum disorder. PLoS ONE 2020, 15, e0237966.
- Vredenburg, K.; Mao, J.Y.; Smith, P.W.; Carey, T. A survey of user-centered design practice. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Minneapolis, MI, USA, 20–25 April 2002; pp. 471–478.
- Aguiar, Y.P.C.; Galy, E.; Godde, A.; Trémaud, M.; Tardif, C. AutismGuide: A usability guidelines to design software solutions for users with autism spectrum disorder. Behav. Inf. Technol. 2022, 41, 1132–1150.
- Beukelman, D.R.; Mirenda, P. Augmentative and Alternative Communication; Paul, H., Ed.; Brookes: Baltimore, MD, USA, 1998.
- Mirenda, P. Toward functional augmentative and alternative communication for students with autism. Lang. Speecch Hear. Serv. Sch. 2003, 34, 203–216.
- Bellini, S.; Akullian, J. A meta-analysis of video modeling and video self-modeling interventions for children and adolescents with autism spectrum disorders. Except. Child. 2007, 73, 264–287.
- Bandura, A.; Walters, R.H. Social Learning Theory; Prentice Hall: Englewood Cliffs, NJ, USA, 1977; Volume 1.
- Davis, R.; Campbell, R.; Hildon, Z.; Hobbs, L.; Michie, S. Theories of behaviour and behaviour change across the social and behavioural sciences: A scoping review. Health Psychol. Rev. 2015, 9, 323–344.
- Michie, S.; Johnston, M.; Carey, R. Behavior change techniques. In Encyclopedia of Behavioral Medicine; Springer: Berlin/Heidelberg, Germany, 2020; pp. 206–213.
- Lee, D.; Frey, G.C.; Cothran, D.J.; Harezlak, J.; Shih, P.C. Effects of a Gamified, Behavior Change Technique–Based Mobile App on Increasing Physical Activity and Reducing Anxiety in Adults With Autism Spectrum Disorder: Feasibility Randomized Controlled Trial. JMIR Form. Res. 2022, 6, e35701.
- Rotheram-Fuller, E.; MacMullen, L. Cognitive-behavioral therapy for children with autism spectrum disorders. Psychol. Sch. 2011, 48, 263–271.
- Taylor, P.J.; Russ-Eft, D.F.; Chan, D.W. A meta-analytic review of behavior modeling training. J. Appl. Psychol. 2005, 90, 692.
- Decker, P.J.; Nathan, B.R. Behavior Modeling Training: Principles and Applications; Greenwood: Westport, CT, USA, 1985.