Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Monica Macrì and Version 2 by Jessie Wu.
The term “functional appliance” refers to a lot of orthodontic appliances initially designed primarily to correct Class II malocclusion; their use received much acclaim in Europe in the 20th century but not in the USA, where Angle’s philosophy, which put in the foreground the need to achieve an ideal dental occlusion with a fixed multibrackets device, was preferred. Elastodontics, therefore, aims to solve skeletal and functional problems in the growth period. Still, at the same time, it represents an extraordinary instrument to readjust the vertical dimension in the adult patient for prosthetic purposes. Elastodontics is a new therapeutic approach that uses removable appliances made with an elastomeric material to produce light and elastic forces to correct malocclusion, aligning them and reducing potential risk factors that can affect growth. This therapy simplifies or eliminates a possible and subsequent orthodontic intervention because it facilitates balanced growth, reduces the number of extractions, and increases stability during treatment. If you change the function through the re-education of behaviour, you will also change the shape. The main purpose of the functional treatment is to “guide” the proper growth of the bone bases by stimulating the perioral muscles and neuromuscular system.
- elastodontics
- elastodontic therapy
- elastodontic appliances
- oral health
1. Description of the Device
Bioactivators (cranio-occlusion-postural multifunctional harmonisers) are appliances made of heat-activated elastic materials. The material used is a polymer/elastomer blend, which is very soft, comfortable, and hardly deformable. The material is heat-activated; it is possible to modify the devices using hot water at about 70 degrees for 30 s and then immersing them in cold water to fix them in the new shape [1]. It is also possible to make changes and shortenings with rubber pads and brushes and restore shine with a flame tool. They are available in blends of different hardness (Shore 55 and 65), chosen according to clinical needs.
An in vitro study evaluated [2][17] the mechanical loads of bioactivators, their maximum compressive strength, and plastic deformation under load (percentage). The study’s results revealed that the strain rate for all orthodontic appliances tested could be considered clinically acceptable. The slight difference found between the devices refers to the recommended clinical use. This reflects that slightly different mechanical properties and characteristics of different elastomeric devices may explain their clinically recommended use. Nowadays, more studies are needed to test these properties after medium- and long-term use [3][18].
The structure of the bioactivators is presentedin Figure 1:
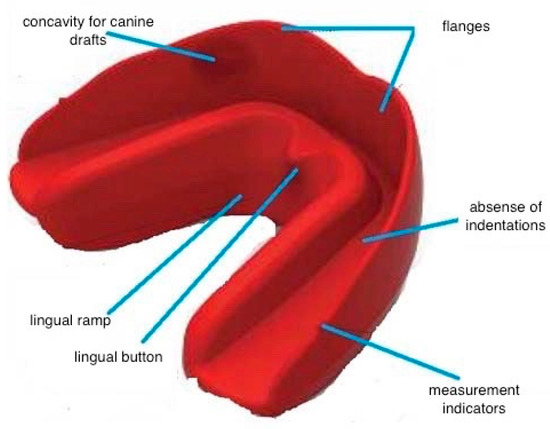
Figure 1.
The structure of bioactivators.
- -
-
Vestibular and lingual flanges form with a free area in the middle where the indentation is absent, and teeth are positioned by an occlusal plane in I-class normocclusion. The vestibular flanges extend up to the border, with the fornixes performing a lip-bumper type function and stimulating proprioceptively the matrix bone. The two arches are thus involved simultaneously, carrying out a multidimensional orthopaedic action in a vertical, transverse, sagittal, and torsional direction;
- -
-
Indicators: are located on the buccal flange and are helpful in detecting the size of the device;
- -
-
Concavity: used at the level of the canine drafts to avoid bone interference;
- -
-
Lingual ramp: used to guide the tongue on the palatal spot;
- -
-
Lingual button: used to correct the position of the tongue.
The device performs a gentle and continuous action on the teeth since it exercises a guiding function by promoting correct dental eruption in a correct bone–tooth–alveolus relationship [3][18].
2. Classification
The devices come in various abbreviations and colours, which indicate their skeletal classes and arch shapes. They are built for the mouths of children, young adults, and adults, and are suitable for all ages from 3 years upwards.
- -
-
Class I bioactivator: used in deciduous, mixed, and permanent dentition to correct arch deviations by correcting the midlines to correct bad habits; it determines a pre-alignment of the teeth and is also used as a restraint after multibracket therapy and basal skeletal disharmonies such as horizontal, transverse, and vertical deficits, such as open or deep bites, and is designed in two different occlusal planes: BASIC: equipped with a raised anterior plane suitable for deep bites and INTEGRAL: equipped with a uniform plane anteriorly and posteriorly used to treat alterations in occlusal curves. Four models can be distinguished based on the different arches and facial biotype forms: F for ogival arches in the dolicofacial arches, S for more rounded arches in the mesofacial, OS for square-shaped arches in the mesofacial, and C for wide dental arches in the brachifacial [4][5] (Figure 2 and Figure 3):
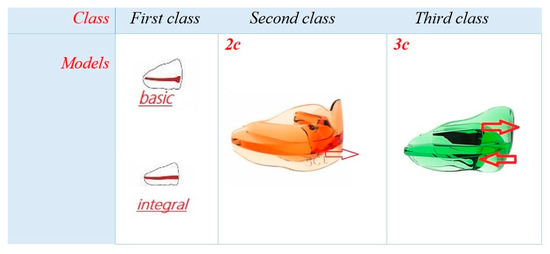 Figure 2.Type of bioactivators based on skeletal and dental class in mixed and permanent dentition.
Figure 2.Type of bioactivators based on skeletal and dental class in mixed and permanent dentition.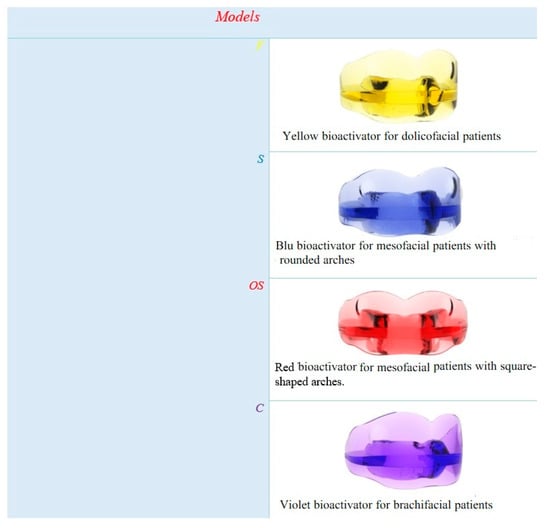 Figure 3.Type of first-class bioactivators based on facial biotype and form of arches.
Figure 3.Type of first-class bioactivators based on facial biotype and form of arches.
- -
- -
-
Class III TC bioactivator: Used for skeletal Class III and pseudo-Class III. It has an anterior sliding plane that guides the correct position of the upper incisors, and it exercises posterior pressure on the mandible to limit its excessive growth. It eliminates the centripetal force of the orbicular muscle and the tongue’s centrifugal force to restore normal muscular function. [4][5] (Figure 2);
- -
-
ElastoOsas bioactivator: Made to clear the respiratory tract by reducing snoring at night and also indicated in cases of bruxism, neuromuscular tension problems, and muscle tension headaches. It has a guide to the lower arch, which is more protruded, a raised occlusal plane, and a lingual ramp that acts as a lingual elevator (accompanies the tongue towards the button in the palatine area) [4][5] (Figure 4);
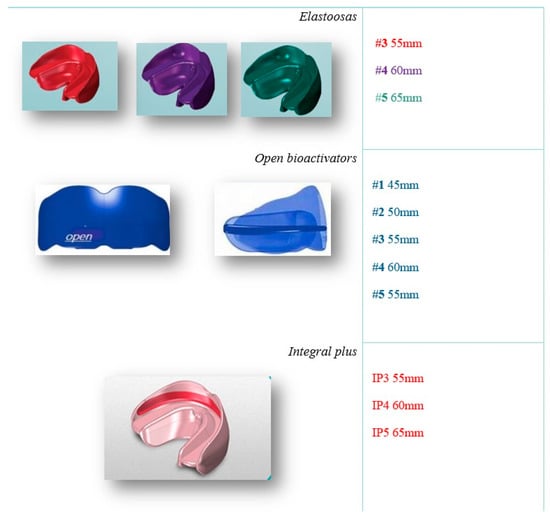 Figure 4. Special bioactivators: elastoosas: in cases of bruxism, neuromuscular tension problems, and muscle tension headaches. Open bioactivator: for open bite. Integral plus: improve the teeth’s alignment and functional, skeletal, joint, and neuromuscular problems with multibrackets therapy.
Figure 4. Special bioactivators: elastoosas: in cases of bruxism, neuromuscular tension problems, and muscle tension headaches. Open bioactivator: for open bite. Integral plus: improve the teeth’s alignment and functional, skeletal, joint, and neuromuscular problems with multibrackets therapy. - -
-
These elements allow the recovery of correct nasal breathing as they free the pharyngeal area;
- -
-
Open bioactivator: Indicated for the treatment of skeletal anterior open bites. The device has a raised rear surface as a specific thrust on the posterior molars. The plane has a “fulcrum” action causing an anteroflexion of the occlusal plane, restoring it horizontally. Contraindicated for ATM-specific problems [4][5] (Figure 4);
- -
-
Integral Plus bioactivator: It has a guide in the inner wall of the upper and lower flange for housing the brackets. It aims to improve the teeth’s alignment and functional, skeletal, joint, and neuromuscular problems. It cannot be used with steel arches, reverse arches, inter-arch elastics, or in the presence of occlusal rises [4][5] (Figure 4);
- -
-
Bioactivator for deciduous teeth: Used in deciduous dentition, indicated to correct deviations of the dental arches, mono and bilateral crossbites, anterior open bites, correct bad habits, improve swallowing and breathing, and night grinding. There are two models: DC (with a pacifier) and D (without a pacifier) [4][5] (Figure 5).
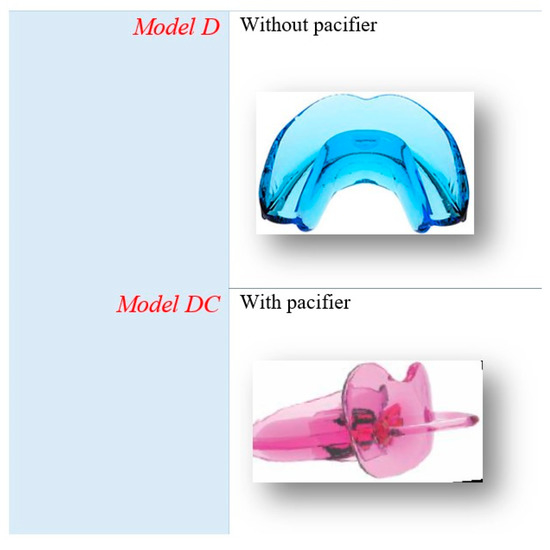 Figure 5.Type of bioactivators for deciduous teeth.
Figure 5.Type of bioactivators for deciduous teeth.
The transverse distance between the outermost point of the vestibular cusps of the first two upper molars is defined as the size of the bioactivator. The size of appliances can also be made through a wax bite (Figure 6 and Figure 7), which is advantageous for young children because it avoids impression taking [5][10]. It makes bioactivators more comfortable than classic functional appliances; they can be used in patients at the age of 2.5 years [1].

Figure 6.
Measures of bioactivators for mixed and permanent dentition.
Figure 7.
Measures of bioactivators for deciduous dentition.
3. Treatment protocol
Regardless of the type of malocclusion to be corrected, the currently available studies show a standard protocol regarding the type of device to be used and the duration of therapy in the active and passive phases of treatment [4][6][7][8][9][4,5,14,19,20].
Patients are treated with these functional devices for 16–18 months.
All patients must wear braces for one hour during the day and all night for 6–8 months and then only at night for the next 12–16 months [4][5].
Generally, when discrepancies to be corrected coexist in more than one plane, rwesearchers proceed in two phases: 6–8 months to correct the vertical and transversal discrepancy and, simultaneously, the sagittal discrepancy [10][21].
4. Exercises
For the optimisation of this device and to obtain the maximum benefit, it is recommended to perform simple exercises slowly and without haste.
The therapy consists of using the device during the day and at night.
Daytime: active exercises with functional exercises to teach correct swallowing and nasal breathing associated with biting the device. At night: keep the device in the mouth in a passive condition.
Swallowing should occur in a normal way. The tongue must be positioned immediately behind the upper incisors and precisely in the area with a button suitable for simulation for 10 s. Next, swallow your saliva and place your tongue against the roof of your mouth for 10 s, then exhale.
After the swallowing and breathing exercises, the active chewing phase of the device can be started. Exert pressure on the occlusal plane of the activator with your teeth and intermittently come out of the outlet (nibbling). The nibbling should take 20 to 30 min. After taking the day therapy for one week to 10 days, the treatment can be completed overnight. The goal is to keep the activator placed in the mouth all night.
5. Advantages and Limits
Bioactivators are an evolution of elastodontic therapy; they simultaneously harmonise, maxilla, and mandible, they work tridimensionally, and they normalise the inclination and rotation of occlusal planes to obtain a correct function and a good balance of the masticatory system [4][5].
Many bioactivators’ advantages derive from their structure and elastomeric material.
The material of the appliances is made of a polymer/elastomer mixture, which has these characteristics: very elastic, comfortable, thermoactivable, and adaptable to different arch shapes.
It is not predisposed to caries, it does not cause lesions to the periodontium, and it does not cause root resorption (still scarce literature on this subject).
Possible interference caused by the flanges can be modified with instruments suitable for heat. The device can also be expanded by immersing it in the water at about 70 °C for 30 s and, to fix it in the new shape, immersing it in cold water. The adjustments and shortenings are made with a rubber brush, and shine is restored with a flame tool [1].
This bioactivator material, together with the myofunctional exercises, restores the balance between the oral and lingual musculature. Normal muscular function is restored by proper relation and balance between skeletal and dentoalveolar components [1][11][12][1,12,22].
A study at the University of Aquila analysed two Class II bioactivators of two different marks on a group of adolescent patients. Both techniques studied improved the degree of OJ and OB between T0 and T1, even 1 year after the start of therapy [13][23].
Various bioactivator models and types suit several kinds of arches, vertical planes, and faces. No construction bite is needed, so it allows reusearchers to avoid the impression manoeuvre, which is not well-tolerated. They are cheap for the patient, and the therapy time is short.
Limitations: it does not rotate canines, molars, and premolars; it does not correct eighth disodontiasis and mesialised teeth; and it cannot be used in patients with mobile dental elements.