Polypoidal choroidal vasculopathy (PCV) was generally considered as a subtype of age-related macular degeneration. Currently, the gold standard for diagnosing PCV is indocyanine green angiography (ICGA). However, it has been concerned about its rare but deadly complications and inconvenience during clinical visits. ICGA cannot provide detailed anatomical information about the disease lesions, either. Swept-source optical coherence tomography angiography (SS-OCTA) is a new, noninvasive, fast, and high-quality imaging method for PCV, which is significantly improved in many aspects compared with the previous spectral domain OCTA (SD-OCTA). With SS-OCTA, the lesion characteristics of PCV have been extensively studied. SS-OCTA revealed a new morphological pattern of the polypoidal lesions (PLs) call “tangled vasculature”, suggesting the neovascular essence of PLs, instead of aneurysmal dilations. In addition, by assessing the changes of choroidal structure, such as the choriocapillaris flow voids, the hypothetical developing model of PCV has been proposed. Due to the improved detecting ability, SS-OCTA might also play a more important role in differential diagnosis, disease reactivation monitoring in the future. This article reviewed recently published papers that focused on imaging PCV with SS-OCTA, summarized advances in the presentation and relevant new pathogenic findings of PCV, and assessed its value in the clinical management of PCV as described above, hoping to update current understandings of PCV and suggest directions for future studies.
- polypoidal choroidal vasculopathy
- swept-source optical coherence tomography angiography
- tangled vasculature
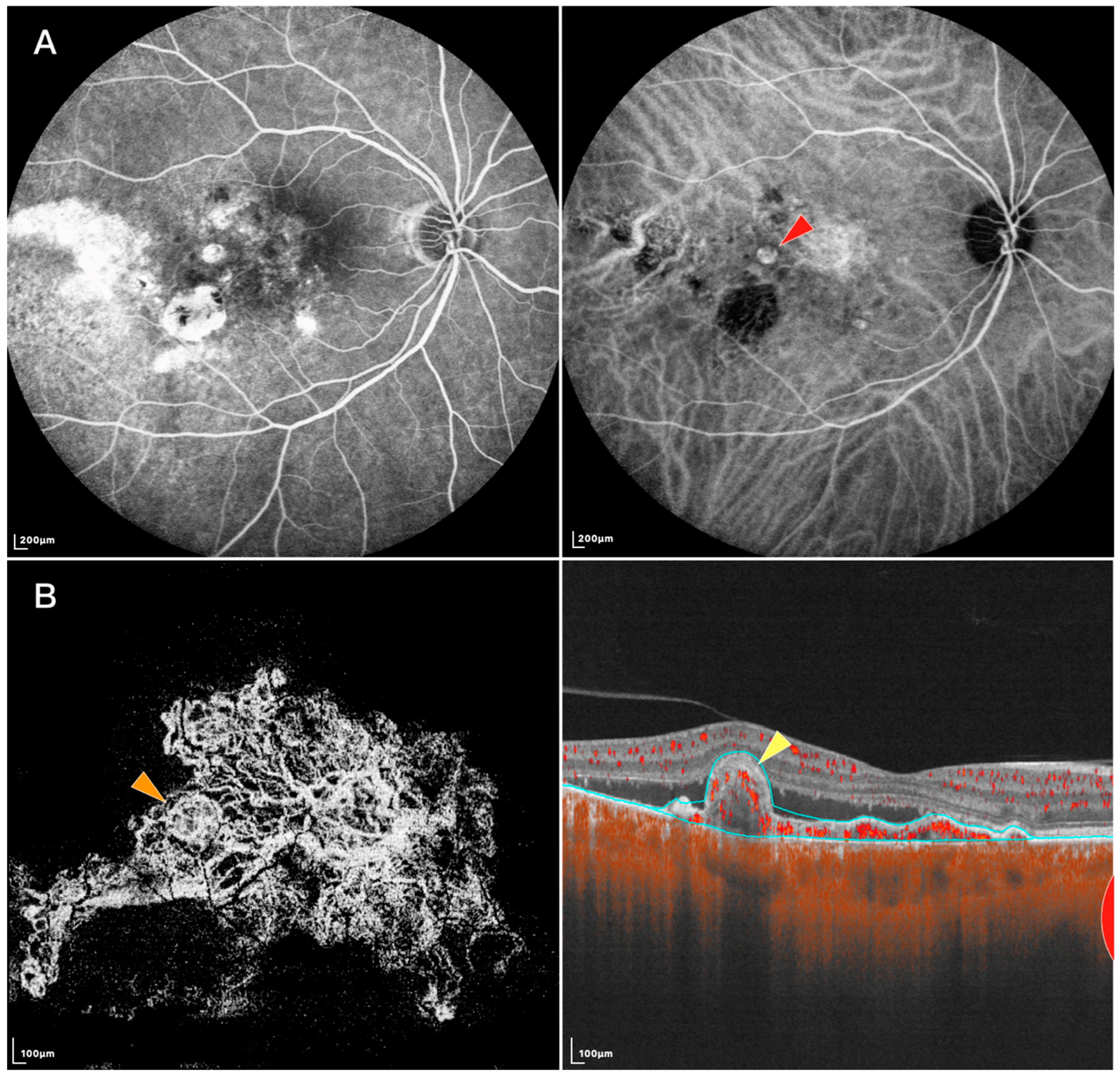
1. Presentation of Polypoidal Lesions on SS-OCTA
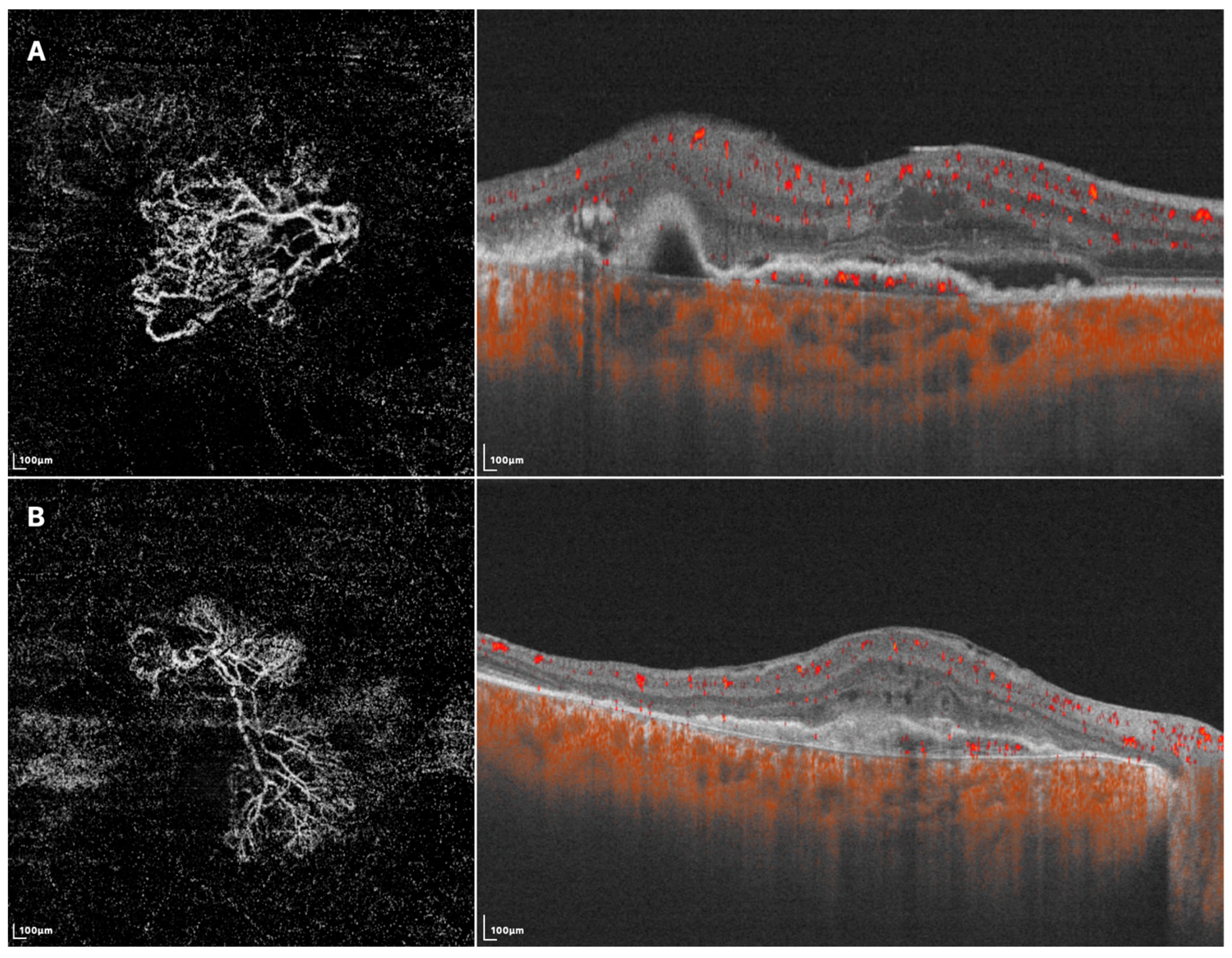
2. Presentation of Branching Vascular Networks on SS-OCTA
3. Choroidal Changes of PCV on SS-OCTA
References
- Cheung, C.M.G.; Yanagi, Y.; Mohla, A.; Lee, S.Y.; Mathur, R.; Chan, C.M.; Yeo, I.; Wong, T.Y. Characterization and differentiation of polypoidal choroidal vasculopathy using swept source optical coherence tomography angiography. Retina 2017, 37, 1464–1474.
- Singh, S.R.; Goyal, P.; Parameswarappa, D.C.; Goud, A.; Chhablani, J. Angiographic features of polypoidal choroidal vasculopathy using indocyanine green angiography and optical coherence tomography angiography: A comparative study. Eur. J. Ophthalmol. 2020, 30, 1076–1081.
- Azar, G.; Vasseur, V.; Lahoud, C.; Favard, C.; De Bats, F.; Cochereau, I.; Yachvitz, A.; Mauget-Faÿsse, M. Polypoidal Choroidal Vasculopathy Diagnosis and Neovascular Activity Evaluation Using Optical Coherence Tomography Angiography. Biomed. Res. Int. 2021, 2021, 1637377.
- Bo, Q.; Yan, Q.; Shen, M.; Song, M.; Sun, M.; Yu, Y.; Rosenfeld, P.J.; Wang, F.; Sun, X. Appearance of Polypoidal Lesions in Patients with Polypoidal Choroidal Vasculopathy Using Swept-Source Optical Coherence Tomographic Angiography. JAMA Ophthalmol. 2019, 137, 642–650.
- Fujita, A.; Kataoka, K.; Takeuchi, J.; Nakano, Y.; Horiguchi, E.; Kaneko, H.M.; Ito, Y.M.; Terasaki, H.M. Diagnostic characteristics of polypoidal choroidal vasculopathy based on b-scan swept-source optical coherence tomography angiography and its interrater agreement compared with indocyanine green angiography. Retina 2020, 40, 2296–2303.
- Kim, K.; Yang, J.; Feuer, W.; Gregori, G.; Kim, E.S.; Rosenfeld, P.J.; Yu, S.-Y. A Comparison Study of Polypoidal Choroidal Vasculopathy Imaged with Indocyanine Green Angiography and Swept-Source Optical Coherence Tomography Angiography. Am. J. Ophthalmol. 2020, 217, 240–251.
- Shen, M.; Bo, Q.; Song, M.; Jiang, X.; Yehoshua, Z.; Gregori, G.; Sun, X.; Wang, F.; Rosenfeld, P.J. Replacement of polyps with type 1 macular neovascularization in polypoidal choroidal vasculopathy imaged with swept source OCT angiography. Am. J. Ophthalmol. Case Rep. 2021, 22, 101057.
- Yuzawa, M.; Mori, R.; Kawamura, A. The origins of polypoidal choroidal vasculopathy. Br. J. Ophthalmol. 2005, 89, 602–607.
- Akaza, E.; Matsumoto, Y.; Yuzawa, M. Pulsation in polypoidal choroidal vasculopathy. Nippon Ganka Gakkai Zasshi 2006, 110, 288–292.
- Chen, Y.; Yang, Z.; Xia, F.; Ning, H.; Hua, R. The blood flow characteristics of polypoidal choroidal vasculopathy and the choroidal remodelling process after photodynamic therapy. Lasers Surg. Med. 2018, 50, 427–432.
- Rebhun, C.B.; Moult, E.M.; Novais, E.A.; Moreira-Neto, C.; Ploner, S.B.; Louzada, R.N.; Lee, B.; Baumal, C.R.; Fujimoto, J.G.; Duker, J.S.; et al. Polypoidal Choroidal Vasculopathy on Swept-Source Optical Coherence Tomography Angiography with Variable Interscan Time Analysis. Transl. Vis. Sci. Technol. 2017, 6, 4.
- Nakashizuka, H.; Mitsumata, M.; Okisaka, S.; Shimada, H.; Kawamura, A.; Mori, R.; Yuzawa, M. Clinicopathologic findings in polypoidal choroidal vasculopathy. Investig. Ophthalmol. Vis. Sci. 2008, 49, 4729–4737.
- Okubo, A.; Sameshima, M.; Uemura, A.; Kanda, S.; Ohba, N. Clinicopathological correlation of polypoidal choroidal vasculopathy revealed by ultrastructural study. Br. J. Ophthalmol. 2002, 86, 1093–1098.
- Li, M.; Dolz-Marco, R.; Messinger, J.D.; Sloan, K.R.; Ferrara, D.; Curcio, C.A.; Freund, K.B. Clinicopathologic Correlation of Aneurysmal Type 1 Neovascularization in Age-Related Macular Degeneration. Ophthalmol. Retin. 2019, 3, 99–111.
- Oishi, A.; Kojima, H.; Mandai, M.; Honda, S.; Matsuoka, T.; Oh, H.; Kita, M.; Nagai, T.; Fujihara, M.; Bessho, N.; et al. Comparison of the effect of ranibizumab and verteporfin for polypoidal choroidal vasculopathy: 12-month LAPTOP study results. Am. J. Ophthalmol. 2013, 156, 644–651.
- Arias, J.D.; Margarita Parra, M.; Hoyos, A.T.; Arango, F.; Viteri, E.J.; Arevalo, J.F. En face swept-source optical coherence tomography angiography choroidal vasculography (CVG) a tool to discriminate choroidal abnormalities in polypoidal choroidal vasculopathy. Expert Rev. Med. Devices 2021, 18, 903–908.
- Liu, G.; Han, L.; Lu, Y.; Wang, C.; Ma, L.; Zhang, P.; Liu, C.; Lu, X.; Ma, Z. Clinicopathological study of the polypoidal lesions of polypoidal choroidal vasculopathy. Graefe’s Arch. Clin. Exp. Ophthalmol. 2022, 260, 2369–2377.
- Wang, Y.; Bo, Q.; Jia, H.; Sun, M.; Yu, Y.; Huang, P.; Wang, J.; Xu, N.; Wang, F.; Wang, H.; et al. Small dome-shaped pigment epithelium detachment in polypoidal choroidal vasculopathy: An under-recognized sign of polypoidal lesions on optical coherence tomography? Eye 2021, 36, 733–741.
- Tsujikawa, A.; Sasahara, M.; Otani, A.; Gotoh, N.; Kameda, T.; Iwama, D.; Yodoi, Y.; Tamura, H.; Mandai, M.; Yoshimura, N. Pigment epithelial detachment in polypoidal choroidal vasculopathy. Am. J. Ophthalmol. 2007, 143, 102–111.
- Huang, C.-H.; Yeh, P.-T.; Hsieh, Y.-T.; Ho, T.-C.; Yang, C.-M.; Yang, C.-H. Characterizing Branching Vascular Network Morphology in Polypoidal Choroidal Vasculopathy by Optical Coherence Tomography Angiography. Sci. Rep. 2019, 9, 595.
- Ma, S.-T.; Huang, C.-H.; Chang, Y.-C.; Lai, T.-T.; Hsieh, Y.-T.; Ho, T.-C.; Yang, C.-M.; Cheng, C.-G.; Yang, C.-H. Clinical features and prognosis of polypoidal choroidal vasculopathy with different morphologies of branching vascular network on optical coherence tomography angiography. Sci. Rep. 2021, 11, 17848.
- Coscas, G.J.; Lupidi, M.; Coscas, F.; Cagini, C.; Souied, E.H. Optical coherence tomography angiography versus traditional multimodal imaging in assessing the activity of exudative age-related macular degeneration: A New Diagnostic Challenge. Retina 2015, 35, 2219–2228.
- Chen, L.; Yuan, M.; Sun, L.; Chen, Y. Different Morphology of Branching Neovascular Network in Polypoidal Choroidal Vasculopathy: A Swept-Source Optical Coherence Tomography Angiography Study. J. Clin. Med. 2023, 12, 742.
- Alasil, T.; Ferrara, D.; Adhi, M.; Brewer, E.; Kraus, M.F.; Baumal, C.R.; Hornegger, J.; Fujimoto, J.G.; Witkin, A.J.; Reichel, E.; et al. En Face Imaging of the Choroid in Polypoidal Choroidal Vasculopathy Using Swept-Source Optical Coherence Tomography. Am. J. Ophthalmol. 2015, 159, 634–643.e632.
- Chung, H.; Byeon, S.H.; Freund, K.B. Focal choroidal excavation and its association with pachychoroid spectrum disorders: A Review of the Literature and Multimodal Imaging Findings. Retina 2017, 37, 199–221.
- Lee, W.K.; Baek, J.; Dansingani, K.K.; Lee, J.H.; Freund, K.B. Choroidal morphology in eyes with polypoidal choroidal vasculopathy and normal or subnormal subfoveal choroidal thickness. Retina 2016, 36 (Suppl. 1), S73–S82.
- Bakthavatsalam, M.; Ng, D.S.; Lai, F.H.; Tang, F.Y.; Brelén, M.E.; Tsang, C.W.; Lai, T.; Cheung, C. Choroidal structures in polypoidal choroidal vasculopathy, neovascular age-related maculopathy, and healthy eyes determined by binarization of swept source optical coherence tomographic images. Graefe’s Arch. Clin. Exp. Ophthalmol. 2017, 255, 935–943.
- Liu, B.; Zhang, X.; Mi, L.; Peng, Y.; Wen, F. Choroidal structure in subtypes of polypoidal choroidal vasculopathy determined by binarization of optical coherence tomographic images. Clin. Exp. Ophthalmol. 2019, 47, 631–637.
- Wei, X.; Ting, D.S.W.; Ng, W.Y.; Khandelwal, N.; Agrawal, R.; Cheung, C.M.G. Choroidal vascularity index a Novel Optical Coherence Tomography Based Parameter in Patients with Exudative Age-Related Macular Degeneration. Retin. J. Retin. Vitr. Dis. 2017, 37, 1120–1125.
- Cho, H.J.; Kim, H.S.; Jang, Y.S.; Han, J.I.; Lew, Y.J.; Lee, T.G.; Kim, C.G.; Kim, J.W. Effects of choroidal vascular hyperpermeability on anti-vascular endothelial growth factor treatment for polypoidal choroidal vasculopathy. Am. J. Ophthalmol. 2013, 156, 1192–1200.e1191.
- Shen, M.; Zhou, H.; Kim, K.; Bo, Q.; Lu, J.; Laiginhas, R.; Jiang, X.; Yan, Q.; Iyer, P.; Trivizki, O.; et al. Choroidal Changes in Eyes with Polypoidal Choroidal Vasculopathy After Anti-VEGF Therapy Imaged With Swept-Source OCT Angiography. Investig. Ophthalmol. Vis. Sci. 2021, 62, 5.
- Wu, H.; Sugano, Y.; Itagaki, K.; Kasai, A.; Shintake, H.; Sekiryu, T. The characteristics of choriocapillaris flow void in the unilateral polypoidal choroidal vasculopathy fellow eyes. Sci. Rep. 2021, 11, 23059.
- Lee, K.; Park, J.H.; Park, Y.G. Analysis of choroidal thickness and vascularity in patients with unilateral polypoidal choroidal vasculopathy. Graefe’s Arch. Clin. Exp. Ophthalmol. 2020, 258, 1157–1164.
- Luo, M.; Zhao, X.; Zhao, N.; Yuan, M.; Yang, J.; Dai, R.; Chen, Y. Comparison of choriocapillary flow density between fellow eyes of polypoidal choroidal vasculopathy and neovascular age-related macular degeneration. BMC Ophthalmol. 2020, 20, 162.
- Kamei, T.; Ooto, S.; Uji, A.; Ichioka, A.; Tsujikawa, A. Choriocapillaris structure in the fellow eye of neovascular age-related macular degeneration patients: An OCT angiography image averaging study. Investig. Ophthalmol. Vis. Sci. 2018, 59, 2808.
- Wu, H.; Sekiryu, T.; Sugano, Y.; Itagaki, K.; Kasai, A.; Shintake, H. A modified measuring method to investigate the choriocapillaris flow void of polypoidal choroidal vasculopathy with swept source optical coherence tomography angiography. Quant. Imaging Med. Surg. 2021, 11, 3146–3156.
- Mahalingam, M.; Sachidanandam, R.; Verma, A.; Alagorie, A.; Sen, P. Choriocapillaris flow deficits in polypoidal choroidal vasculopathy using swept source optical coherence tomography angiography. Indian J. Ophthalmol. 2022, 70, 3002–3007.
- Baek, J.; Kook, L.; Lee, W.K. Choriocapillaris Flow Impairments in Association with Pachyvessel in Early Stages of Pachychoroid. Sci. Rep. 2019, 9, 5565.