Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 2 by Conner Chen and Version 1 by Juan Sahuquillo.
Chiari malformations are a group of craniovertebral junction anomalies characterized by the herniation of cerebellar tonsils below the foramen magnum, often accompanied by brainstem descent. The existing classification systems for Chiari malformations have expanded from the original four categories to nine, leading to debates about the need for a more descriptive and etiopathogenic terminology.
- Arnold-Chiari Malformation
- Rare diseases
- Syringomyelia
1. Introduction
Chiari malformations (CMs) are a heterogeneous group of anomalies of the posterior fossa (PF) and/or the craniovertebral junction (CVJ) characterized by herniation of the cerebellar tonsils below the level of the foramen magnum (FM), often in conjunction with varying degrees of brainstem descent (Figure 1 and Figure 2). These malformations—some authors consider the term ‘deformation’ more appropriate [1,2][1][2]—were described in the late 18th century by the Austrian pathologist Hans Chiari from the autopsy of children [3,4][3][4]. Since then, this topic has generated controversy and continues to do so. The correct eponym, the phenotypic variations that should be included under the term CMs including new subtypes, the best terminology to define Chiari-like cerebellar tonsillar herniations (TH) found in syndromic and non-syndromic patients, and even the pathophysiology, have been a matter of considerable debate. A review of the literature of the last two decades shows that there are still several problems to be resolved in CM and that each one generates important controversies. Among the most relevant are whether a slight tonsillar ectopia should be considered a ‘normal’ anatomical variant, if incidental patients with CM1 require clinical follow-up, indications for surgery, and, if needed, the most suitable surgical treatment. Professionals, patients, and their families are confused by the variety of opinions and lack of agreement on each topic [5].

Figure 1. Posterior view (Left) and inferior view (Right) of the cerebellum and brainstem. BLm: Bivental lobe, medial part; CeT: Cerebellar tonsils; Fl: Flocculus; PV: Pyramid of vermis; TV: Tuber of vermis. From: Véronique Schotte, https://sites.uclouvain.be/braininteratlas/en/chapter/cerebellum. Images licensed under Creative Commons License 4.0 (https://creativecommons.org/licenses/by-nc/4.0/ (accessed on 7 June 2023) ).
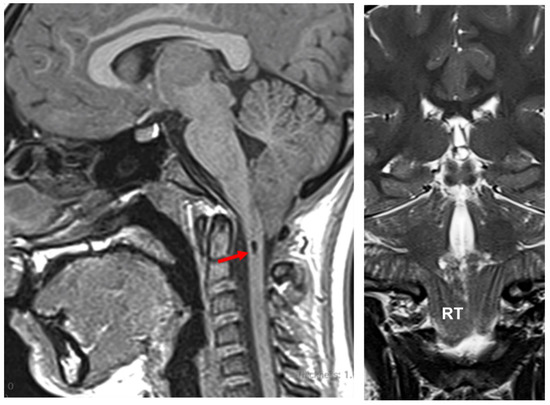
Figure 2. Chiari type 1 malformation. Sagittal T1-weighted MRI (left) and T2-weighted coronal (right) of a 13-year-old girl referred to neurosurgery with clinical symptoms of dizziness and unstable gait for the last 18 months. Her symptoms progressed in the last three months when she started to report paresthesia in the lower right foot. She did not report headaches. Neurological examination was normal. MRI disclosed a widened foramen magnum, a short subocciput, and asymmetrical herniation of the cerebellar tonsils 19 mm below McRae’s line. The (right) tonsil (RT) was slightly more herniated than the (left). A small syrinx is observed in the midsagittal T1-weighted slice, just below the lowest tip of the tonsils (red arrow).
2. A Brief Historical Review of the Chiari Malformation and the ‘Arnold-Chiari’ Eponym
Hans Chiari originally classified CMs into three types (CM1, CM2, and CM3) [4], and later, in 1895, he added a new category (CM4) [3]. Over the last two decades, several subtypes have been added by others (CM0, CM0.5, CM1.5, CM3.5, and CM5), with a total of nine variants described today and summarized in Table 1 [11,12,13,14][6][7][8][9].
Table 1. A summary of the different types of Chiari malformations (CMs) described in the indexed peer-reviewed literature under the eponym CMs. Due to the exceptionally rare anomalies and the absence of precise embryological investigations, CM3, CM3.5, CM4, and CM5 may be malformations unrelated to the more common CM0, CM1, CM1.5, and CM2. The versions that are kept in the ICC-CM classification are noted in bold and yellow background.

Despite various claims to the contrary and many historical studies [11[6][10][11][12][13],15,16,17,18], the eponym ‘Arnold-Chiari malformation’ is still used to describe this diverse set of malformations [18][13]. The main reason for the persistence of this eponym is that any biomedical literature search strategy using PubMed must include the Medical Subject Headings (MeSH) term ‘Arnold-Chiari Malformation’, which was added to MEDLINE in 1966 and remains unchanged since then [19][14]. The MeSH thesaurus is a hierarchically ordered medical vocabulary maintained by the National Library of Medicine and used for indexing, cataloging, and searching health-related papers on a particular subject, regardless of the terminology used by authors. For the purpose of promoting historical justice [15,16][10][11].
In the last two decades, the pathogenesis, screening, genetic inheritance, and surgical treatment of CMs, specifically the Chiari type 1 malformation (CM1) and the frequently associated syringomyelia (Syr), have received increased attention in the medical literature. CM1 is included in the Orphanet database (ORPHAcode: 268882), the reference information source on rare disease research that uses nomenclature (ORPHAcode) that provides a common language in the field of rare diseases [21][15].
The most common Chiari phenotype, regardless of the TH cutoff used to define it, is CM1. The concept that CM1 was a sporadic condition has persisted for a very long time but has proved to be incorrect. Recent evidence obtained from genetic studies—twin studies, familial clustering, etc.—clearly shows that, although most primary CM1 cases are sporadic, 5–30% of them have a non-Mendelian inheritance [23,24,25][16][17][18]. Non-sporadic CM1 is multigenic and involves several chromosomes—1, 8, 9, 12, 15, and 22—diverse chromosome regions, and many genes [24,25,26][17][18][19]. Urbizu et al., in the study of a Spanish family with multiple affected individuals, discovered the contribution of rare genetic variants in collagen genes to CM1 [27][20]. Recently, it has been suggested that CMs could be the result of an altered epigenetic regulation of genes involved in the proliferation of brain cells [28][21].
To understand the modern reclassification of CMs, it is essential to briefly summarize its history and how the eponyms used to describe the different variants have progressed. This framework is necessary to understand how Chiari’s categorization has evolved from its initial description in the late 19th century to the most recent revision incorporated in the documents resulting from the International Consensus Conference held in Milan, Italy, in 2019 (ICC-CM) [8,9,10][22][23][24]. Reading the ‘primary sources’ is the best course of action for updating the history of a certain subject because they include first-hand accounts and research information. The use of secondary sources—translations, evaluations, and interpretations of primary sources—is sometimes misleading and might lead to contradictory and sometimes wrong conclusions. From the 1850s to the early 1900s, when CMs were first described [29][25], German was the dominant scientific language for the production of scientific knowledge, and with a few exceptions, most early papers dealing with CMs were published in German or French [3,4,30,31][3][4][26][27].
To our knowledge, the first description of cerebellar tissue herniating below the FM was reported by Cruveilhier (1791–1874), a French military surgeon and anatomist who, in his atlas of general pathology published in 1829, presented the findings of many cases of spina bifida [30][26]. In one of the reported cases, the patient had an associated diastematomyelia, and he reported that “…the upper part of the considerably dilated cervical region, contained both the medulla oblongata and the corresponding part of the cerebellum, which was elongated and covered the fourth ventricle, itself enlarged and elongated.” [15,30][10][26]. Cruveilhier’s work was cited by Chiari and was analog with his description of Chiari type 2 (CM2), where not only the cerebellum but also the brainstem and IV ventricle were displaced into the cervical canal [3,4][3][4].
In 1883, the Scottish anatomist John Cleland (1835–1925) published a brief description of an infant with spina bifida and hydrocephalus [32][28]; some have argued that Cleland was the “first to publish observations on the morphology of what is termed Arnold-Chiari Malformation (cerebellar ectopy)…” [33][29], but after reading the primary sources, we do not believe this to be the case. In his 1883 paper, Cleland reported nine autopsy cases of spina bifida, encephalocele, and anencephaly [32][28]. In one of the cases with hydrocephalus (Specimen #1, Figure 6), he described that the elongated part of the inferior vermis was misplaced within an elongated IV ventricle [32][28]. In his paper, Cleland described the cerebellum as having “…its two lateral lobes completely separated by the vallecula”, yet he did not mention the ectopia of the cerebellum into the cervical canal [32][28]. Chiari cited Cleland’s findings, and, regarding his work, he wrote that the cerebellum was described (by Cleland) as “…two completely separated hemispheres and the nodulus was highly elongated within the elongated 4th ventricle. Unfortunately, this finding is treated only very briefly and the illustration is only macroscopic.” [3]. Fries et al. reported that Otto Mennicke, a German physician, reported the first case of CM1 in his PhD dissertation [34][30]. However, Mennicke’s thesis was written in 1891, the same year Chiari published his first report [4]. In addition, Mennicke reported two cases of syringomyelia [35][31], a disorder that had already been described in 1827 by Ollivier d’Angers [36][32]. Mennicke gave credit to Chiari for his previous and comprehensive work on syringomyelia [35][31].
In 1894—four years after the first Chiari report—the German pathologist Julius Arnold (1835–1915), working in Heidelberg, Germany, published the case of an infant with spina bifida but without hydrocephalus and described a cone-shaped extension of the cerebellum into the cervical canal. In his own words, “the cerebellum continues downwards in a ribbon-like mass, broader above, narrower below, and completely covering the 4th ventricle, descending almost to the middle of the cervical cord” [31][27]. Arnold did not cite Chiari’s findings [31][27]. Hans Chiari (1851–1916) was an Austrian pathologist who, while working in Prague, wrote two seminal papers in 1891 and 1895 describing the spectrum of the four malformations included today under the modern eponym ‘Chiari or Arnold-Chiari malformations’ [3,4,37,38][3][4][33][34] (Figure 43). In his first paper, Chiari presented a preliminary report of the abnormalities found in necropsies of the cerebellum and brainstem induced by congenital hydrocephalus [4,37][4][33]. In this 1891 report, Chiari described three different phenotypes and presented the pathological findings in three specific patients [4,37][4][33]. The first type was characterized by “the extension of the tonsils and the medial parts of the inferior lobes of the cerebellum into cone-shaped projections which accompany the medulla oblongata into the spinal canal” [4,37][4][33]. He reported a second type in a six-month-old girl with “a lumbar myelomeningocele with diastematomyelia, and hydromyelia in the thoracic cord”, who presented “…displacement of portions of the cerebellum within the elongated fourth ventricle into the widened spinal canal” [4,37][4][33]. Chiari also described a third type in a five-month-old girl with a cerebellar-cervical hydroencephalocele in whom he found an “…almost complete displacement of the cerebellum, itself hydrocephalic, into a cervical spina bifida as a result of cerebral hydrocephalus” [4,37][4][33]. Chiari considered that all the anomalies described were a direct consequence of congenital hydrocephalus [4,37][4][33] and he expanded his preliminary findings in a second paper published in 1895 [3] in which he added 63 cases of congenital hydrocephalus, of which 14 had CM1 and 7 CM2 [3,37][3][33]. In this 1895 paper, Chiari added a fourth phenotype to the first three reported in 1891. Chiari type 4 (CM4) was described in two cases with cerebellar hypoplasia that Chiari believed was also caused by congenital hydrocephalus [3]. In his own words, type 4 cases “…were distinguished by the fact that they involved developmental disturbances of the cerebellum to be included in the area of hypoplasia, without any displacement of parts of the cerebellum into the vertebral canal” [3].
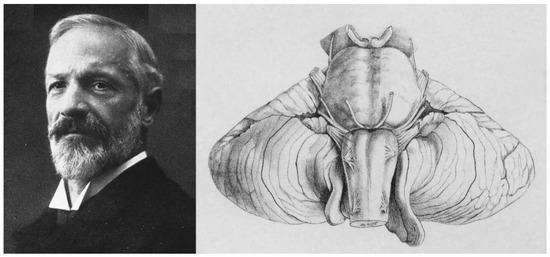
Figure 43. (Left): Hans Chiari (1851–1916), an Austrian pathologist who, while working at the University of Prague, described the malformations now known as Chiari malformations. (Right): Figure 1 of Chiari’s paper published in 1895 [3] corresponding to the cerebellum of a six-year-old boy with a prior diagnosis of “Hemiplegia spastica”, who died of diphtheria and pneumonia. In his detailed report, Chiari described that the lateral and III ventricles were dilated but the IV ventricle was of normal size. The cerebellum, normally configured, presented a bilateral asymmetrical herniation of the cerebellar tonsils surrounding the medulla oblongata laterally and especially dorsally. The left tonsil ended at the level of the lower edge of the atlas and the right one above the upper edge of the atlas.
The widespread eponym ‘Arnold-Chiari’ was introduced in the literature in 1907 by two of Arnold’s students (Schwalbe and Gredig) in a review published in under the title “On developmental disorders of the cerebellum, brainstem, and cervical cord in spina bifida (Arnold’s and Chiari’s malformation)” [38,39][34][35]. As remarked quite bluntly by Sarnat, “both authors were former students (i.e., residents) who wanted ‘to honor their professor,’ knowing well that their assertion was fraudulent.”[40][36]. For some inexplicable reason, the incorrect eponym is still in use as a legacy of a historical mistake.
References
- Poretti, A.; Ashmawy, R.; Garzon-Muvdi, T.; Jallo, G.I.; Huisman, T.A.; Raybaud, C. Chiari Type 1 Deformity in Children: Pathogenetic, Clinical, Neuroimaging, and Management Aspects. Neuropediatrics 2016, 47, 293–307.
- Thompson, D.N.P. Chiari I—A ‘not so’ congenital malformation? Childs Nerv. Syst. 2019, 35, 1653–1664.
- Chiari, H. Über Veränderungen des Kleinhirns, des Pons und der Medulla Oblongata in Folge von Congenitaler Hydrocephalie; K.K. Hof- und Staatsdruckerei: Wien, Austria, 1895; Volume 63, pp. 71–116.
- Chiari, H. Über Veränderungen des Kleinhirns Infolge von Hydrocephalie des Grosshirns. Denkschr. Der Kais. Akad. Der Wiss. /Math.-Naturwissenschaftliche Cl. 1891, 17, 1172–1175.
- van Dellen, J.R. Chiari Malformation: An Unhelpful Eponym. World Neurosurg. 2021, 156, 1–3.
- Tubbs, R.S.; Turgut, M. Defining the Chiari Malformations: Past and Newer Classifications. In The Chiari Malformations, 2nd ed.; Tubbs, R.S., Turgut, M., Oakes, W.J., Tubbs, R.S., Turgut, M., Oakes, W.J., Eds.; Springer: New York, NY, USA, 2020; pp. 21–39.
- Fisahn, C.; Shoja, M.M.; Turgut, M.; Oskouian, R.J.; Oakes, W.J.; Tubbs, R.S. The Chiari 3.5 malformation: A review of the only reported case. Childs Nerv. Syst. 2016, 32, 2317–2319.
- Tubbs, R.S.; Muhleman, M.; Loukas, M.; Oakes, W.J. A new form of herniation: The Chiari V malformation. Childs Nerv. Syst. 2012, 28, 305–307.
- Cools, M.J.; Wellons, J.C., 3rd; Iskandar, B.J. The Nomenclature of Chiari Malformations. Neurosurg. Clin. N. Am. 2023, 34, 1–7.
- Pearce, J.M.S. Historical note. Arnold Chiari, or “Cruveilhier Cleland Chiari” malformation. J. Neurol. Neurosurg. Psychiat. 2000, 68, 13.
- Solt, I. Chiari malformation eponym- time for historical justice (letter). Ultrasound Obstet. Gynecol. Off. J. Int. Soc. Ultrasound Obstet. Gynecol. 2011, 37, 250–251.
- Azahraa Haddad, F.; Qaisi, I.; Joudeh, N.; Dajani, H.; Jumah, F.; Elmashala, A.; Adeeb, N.; Chern, J.J.; Tubbs, R.S. The newer classifications of the chiari malformations with clarifications: An anatomical review. Clin. Anat. 2018, 31, 314–322.
- Tubbs, R.S.; Turgut, M.; Oakes, W.J. A History of the Chiari Malformations. In Chiari Malformations, 2nd ed.; Tubbs, R.S., Turgut, M., Oakes, W.J., Eds.; Springer: New York, NY, USA, 2020; pp. 3–20.
- PubMed. Arnold-Chiari Malformation MeSH Descriptor Data 2022. Available online: https://meshb.nlm.nih.gov/record/ui?ui=D001139 (accessed on 3 July 2023).
- Orphanet. The Portal for Rare Diseases and Orphan Drugs; Orphanet: Paris, France, 2023.
- Loukas, M.; Shayota, B.J.; Oelhafen, K.; Miller, J.H.; Chern, J.J.; Tubbs, R.S.; Oakes, W.J. Associated disorders of Chiari Type I malformations: A review. Neurosurg. Focus 2011, 31, E3.
- Capra, V.; Iacomino, M.; Accogli, A.; Pavanello, M.; Zara, F.; Cama, A.; De Marco, P. Chiari malformation type I: What information from the genetics? Childs Nerv. Syst. 2019, 35, 1665–1671.
- Markunas, C.A.; Enterline, D.S.; Dunlap, K.; Soldano, K.; Cope, H.; Stajich, J.; Grant, G.; Fuchs, H.; Gregory, S.G.; Ashley-Koch, A.E. Genetic Evaluation and Application of Posterior Cranial Fossa Traits as Endophenotypes for Chiari Type I Malformation. Ann. Hum. Genet. 2014, 78, 1–12.
- Urbizu, A.; Khan, T.N.; Ashley-Koch, A.E. Genetic dissection of Chiari malformation type 1 using endophenotypes and stratification. J. Rare Dis. Res. Treat. 2017, 2, 35–42.
- Urbizu, A.; Garrett, M.E.; Soldano, K.; Drechsel, O.; Loth, D.; Marcé-Grau, A.; Mestres, I.S.O.; Poca, M.A.; Ossowski, S.; Macaya, A.; et al. Rare functional genetic variants in COL7A1, COL6A5, COL1A2 and COL5A2 frequently occur in Chiari Malformation Type 1. PLoS ONE 2021, 16, e0251289.
- Miro, X.; Zhou, X.; Boretius, S.; Michaelis, T.; Kubisch, C.; Alvarez-Bolado, G.; Gruss, P. Haploinsufficiency of the murine polycomb gene Suz12 results in diverse malformations of the brain and neural tube. Dis. Model Mech. 2009, 2, 412–418.
- Ciaramitaro, P.; Massimi, L.; Bertuccio, A.; Solari, A.; Farinotti, M.; Peretta, P.; Saletti, V.; Chiapparini, L.; Barbanera, A.; Garbossa, D.; et al. Diagnosis and treatment of Chiari malformation and syringomyelia in adults: International consensus document. Neurol. Sci. 2022, 43, 1327–1342.
- Massimi, L.; Peretta, P.; Erbetta, A.; Solari, A.; Farinotti, M.; Ciaramitaro, P.; Saletti, V.; Caldarelli, M.; Canheu, A.C.; Celada, C.; et al. Diagnosis and treatment of Chiari malformation type 1 in children: The International Consensus Document. Neurol. Sci. 2021, 43, 1311–1326.
- Ciaramitaro, P.; Garbossa, D.; Peretta, P.; Piatelli, G.; Massimi, L.; Valentini, L.; Migliaretti, G.; Baldovino, S.; Roccatello, D.; Kodra, Y.; et al. Syringomyelia and Chiari Syndrome Registry: Advances in epidemiology, clinical phenotypes and natural history based on a North Western Italy cohort. Ann. Ist. Super. Sanita 2020, 56, 48–58.
- Gordin, M.D. Scientific Babel: How Science Was Done Before and After Global English; The University of Chicago Press: Chicago, IL, USA; London, UK, 2015; 415p.
- Cruveilhier, J. Anatomie Pathologique du Corps Humain ou Descriptions avec Figures Litographiées et Coloriées des Diverses Altération Morbides dont le Corps Humain est Susceptible; J.B. Bailliere: Paris, France, 1829; pp. 1829–1842.
- Arnold, J. Myelocytes, Transposition von Gewebskeimen und Sympodie. Beitr. Pathol. Anat. 1894, 16, 1–28.
- Cleland, J. Contribution to the Study of Spina Bifida, Encephalocele, and Anencephalus. J. Anat. Physiol. 1883, 17, 257–292.
- Black, A. John Cleland 1835–1925. Scott. Med. J. 2002, 47, 140–142.
- Fries, F.N.; Hendrix, P.; Brinker, T.J.; Loukas, M.; Tubbs, R.S. Otto Mennicke (1876-) and the first description of skull base anomalies causing cerebellar tonsillar ectopia: One of the first mentions of the Chiari I malformation. Childs Nerv. Syst. 2017, 33, 825–827.
- Mennicke, O. Ueber Syringomyelie Syringomyelie Mit Anatomischer Untersuchung Zweier Fälle; University of Marburg, Universitäts- Buchdruckerei (R. Friedrich): Maburg, Germany, 1891.
- Ollivier, C.P. Traité de la Moelle Épinière et de ses Maladies: Contenant L’histoire Anatomique, Physiologique et Pathologique de ce Centre Nerveux chez L’homme; Crevot: Paris, France, 1827; Volume 1.
- Radkowski, M.A. Hans Chiari. Concerning alterations in the cerebellum resulting from cerebral hydrocephalus (English translation). Pediatr. Neurosci. 1987, 13, 3–8.
- Bejjani, G.K. Definition of the adult Chiari malformation: A brief historical overview. Neurosurg. Focus 2001, 11, 1–8.
- Schwalbe, E.; Gredig, M. Ueber Entwicklungsstorungen des Kleinhirns, Hirnstamms und Halsmarks bei Spina Bifida (Arnold’sche und Chiari’sche Missbildung). Beitr. Path. Anat. 1907, 40, 132–194.
- Sarnat, H.B. Semantics do matter! Precision in scientific communication in pediatric neurology. J. Child Neurol. 2007, 22, 1245–1251.
More