Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 2 by Conner Chen and Version 1 by Radu MIFTODE.
Acute heart failure (AHF) is a life-threatening condition with high morbidity and mortality. Even though this pathology has been extensively researched, there are still challenges in establishing an accurate and early diagnosis, determining the long- and short-term prognosis and choosing a targeted therapeutic strategy. The use of reliable biomarkers to support clinical judgment has been shown to improve the management of AHF patients. Despite a large pool of interesting candidate biomarkers, endothelin-1 (ET-1) appears to be involved in multiple aspects of AHF pathogenesis that include neurohormonal activation, cardiac remodeling, endothelial dysfunction, inflammation, atherosclerosis and alteration of the renal function.
- endothelin-1
- acute heart failure
- biomarkers
1. Introduction
Heart failure (HF) is currently a major public health concern, affecting more than 25 million people worldwide, with a growing prevalence and extensive socio-economic burden [1,2][1][2]. Remarkable advances in the past three decades in optimizing the prevention, diagnosis and treatment of HF have contributed to the increase in life expectancy in these patients. However, acute heart failure (AHF) is the most common cause of hospitalization, and the prognosis of patients after discharge continues to be poor [1,3][1][3]. AHF is a life-threatening condition with dramatic burdens in terms of symptomatology, morbidity, and mortality [4]. The length of hospitalization of these patients is on average 5 days, and the readmission rate in the first 3 months after discharge can reach 30% [5,6][5][6]. In addition, in-hospital mortality is estimated at 10% of cases, and up to 20% of survivors die within 30 days [3].
AHF is a complex syndrome which requires emergency evaluation and treatment, being defined either as a rapid “de novo” onset or worsening of symptoms and signs of a previously stable chronic HF (CHF). Most patients are admitted for an acute decompensation of a CHF caused by precipitating factors, such as myocardial ischemia, uncontrolled arterial hypertension, arrhythmias, pulmonary embolism, acute kidney injury, infections, or low therapeutic adherence, while the “de novo” onset of AHF is mainly associated with acute coronary syndromes [6,7,8][6][7][8].
The relatively modest improvement concerning the therapeutic management of patients with AHF could be mainly due to the inability to recognize the various pathophysiological processes that occur during decompensation [9]. The diagnostic challenges arise from the fact that these patients exhibit a complex yet not specific clinical picture and usually have multiple comorbidities requiring a holistic approach [4,6,7,10][4][6][7][10].
Biomarkers can play an important role in addressing these deficiencies, and their routine incorporation into clinical practice can improve the outcomes. Many biomarkers are well established for their use in cardiovascular disease and in the management of CHF. In addition, several new biomarkers have recently shown promising results, especially in AHF, which could further improve patient management [9,11][9][11].
Current paradigm is shifting towards the study of various biomarkers which are associated with myocardial injury processes, neurohormonal activation, oxidative stress, and cardiac remodeling, with promising results in terms of clinical utility [5,11,12][5][11][12].
Endothelin-1 (ET-1) is a vasoconstrictive peptide that is primarily produced by endothelial cells and cardiomyocytes. It plays a role in the pathophysiology of various diseases, including heart failure, by causing cardiac hypertrophy and having profibrotic and proinflammatory effects [13,14,15,16][13][14][15][16]. Numerous literature data confirm that patients with these pathologies have higher levels of ET-1, which is linked to higher mortality as well as hospitalization rates. Based on previous observations, ET-1 may provide additional prognostic information beyond clinical variables [17].
2. The Endothelin System: Morphofunctional Considerations
The endothelium has an essential role in protecting the arterial wall by releasing nitric oxide (NO) and prostacyclin. One year after discovering that endothelium has the ability to constrict and relax, one proposed the hypothesis of an endothelium-derived constricting factor [17]. The discovery of ET-1 by Yahagisawa et al. in 1988 represented a fundamental landmark in the field of cardiovascular research. In 1990, two receptors of ET-1 were identified, type A (ETA) and type B (ETB), respectively, offering the foundation for designing Bosentan (an antagonist of the ET-1 receptor), which can be currently used in the treatment of patients with pulmonary arterial hypertension. Multiple molecular and pharmacological approaches have outlined ET-1 as the most potent vasoconstrictor identified in biological systems to date. Since its discovery, remarkable efforts have been made to thoroughly understand the pathophysiological implications of this peptide in the cardiovascular system [18,19,20][18][19][20]. The ET system consists of three interconnected peptides: ET-1, ET-2 and ET-3. The 21-amino-acid peptide ET-1 is the main isoform produced at cardiovascular level and it has been the most intensively studied [19]. ETs have multiple pathophysiological functions involved not only in cardiovascular disorders (HF, arterial hypertension, cardiac hypertrophy, atherosclerosis), but also in pulmonary and kidney pathologies. Moreover, the ET system is implicated in tumoral processes, wound healing, and neurohormonal activation [21]. ET-1 is a 21-amino-acid cyclic peptide with two disulfide bonds consisting of four cysteines. The N-terminal end of the peptide defines its binding affinity to the receptor, whereas at the C-terminal end is located in the amino acids that bind to the receptor [21] (Figure 1).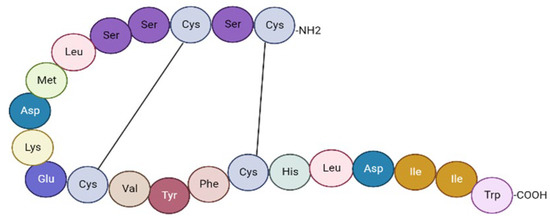
Figure 1. Endothelin-1 structure (adapted from Khimji et al. [21]) This image was created with BioRender (https://biorender.com/ accessed on 14 May 2023).
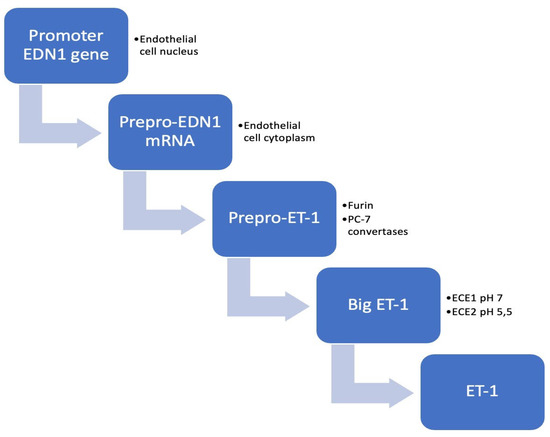
Figure 2. Endothelin-1 cycle. Abbreviations: EDN1—encoding endothelin-1; ECE—endothelin-converting enzyme; ET-1—endothelin-1.
Table 1.
Subtypes of ET and their tissue sites of synthesis.
| ET-1 | ET-2 | ET-3 |
|---|---|---|
| Vascular smooth muscle cells | Gastrointestinal stromal cells | Gastrointestinal stromal cells |
| Endothelial cells | Kidney epithelial cells | Kidney epithelial cells |
| Cardiac myocytes | Neurons | |
| Kidney epithelial cells | Glia | |
| Inflammatory cells | ||
| Hepatocytes | ||
| Neurons |
References
- Mentz, R.J.; O’Connor, C.M. Pathophysiology and clinical evaluation of acute heart failure. Nat. Rev. Cardiol. 2016, 13, 28–35.
- Miftode, R.-S.; Costache, I.-I.; Cianga, P.; Petris, A.O.; Cianga, C.-M.; Maranduca, M.-A.; Miftode, I.-L.; Constantinescu, D.; Timpau, A.-S.; Crisan, A.; et al. The Influence of Socioeconomic Status on the Prognosis and Profile of Patients Admitted for Acute Heart Failure during COVID-19 Pandemic: Overestimated Aspects or a Multifaceted Hydra of Cardiovascular Risk Factors? Healthcare 2021, 9, 1700.
- Teerlink, J.R.; McMurray, J.J.; Bourge, R.C.; Cleland, J.G.; Cotter, G.; Jondeau, G.; Krum, H.; Metra, M.; O’Connor, C.M.; Parker, J.D.; et al. Tezosentan in patients with acute heart failure: Design of the Value of Endothelin Receptor Inhibition with Tezosentan in Acute heart failure Study (VERITAS). Am. Heart J. 2005, 150, 46–53.
- Tomasoni, D.; Lombardi, C.M.; Sbolli, M.; Cotter, G.; Metra, M. Acute heart failure: More questions than answers. Prog. Cardiovasc. Dis. 2020, 63, 599–606.
- Pourafkari, L.; Tajlil, A.; Nader, N.D. Biomarkers in diagnosing and treatment of acute heart failure. Biomark. Med. 2019, 13, 1235–1249.
- Arrigo, M.; Jessup, M.; Mullens, W.; Reza, N.; Shah, A.M.; Sliwa, K.; Mebazaa, A. Acute heart failure. Nat. Rev. Dis. Primers 2020, 6, 16.
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200.
- Sinnenberg, L.; Givertz, M.M. Acute heart failure. Trends Cardiovasc. Med. 2020, 30, 104–112.
- Wettersten, N. Biomarkers in Acute Heart Failure: Diagnosis, Prognosis, and Treatment. Int. J. Heart Fail. 2021, 3, 81–105.
- Maisel, A.S.; Choudhary, R. Biomarkers in acute heart failure-state of the art. Nat. Rev. Cardiol. 2012, 9, 478–490.
- Mallick, A.; Januzzi, J.L. Biomarkers in acute heart failure. Rev. Esp. Cardiol. 2015, 68, 514–525.
- Miftode, R.-S.; Constantinescu, D.; Cianga, C.-M.; Petris, A.-O.; Costache, I.-I.; Mitu, O.; Miftode, I.-L.; Mitu, I.; Timpau, A.-S.; Duca, S.-T.; et al. A Rising Star of the Multimarker Panel: Growth Differentiation Factor-15 Levels Are an Independent Predictor of Mortality in Acute Heart Failure Patients Admitted to an Emergency Clinical Hospital from Eastern Europe. Life 2022, 12, 1948.
- Yanagisawa, M.; Kurihara, H.; Kimura, S.; Tomobe, Y.; Kobayashi, M.; Mitsui, Y.; Yazaki, Y.; Goto, K.; Masaki, T. A novel potent vasoconstrictor peptide produced by vascular endothelial cells. Nature 1988, 332, 411–415.
- Jankowich, M.; Choudhary, G. Endothelin-1 levels and cardiovascular events. Trends Cardiovasc. Med. 2020, 30, 1–8.
- Matsubara, T.J.; Fujiu, K. Endothelin-1 and Atrial Cardiomyopathy. Int. Heart J. 2019, 60, 238–240.
- Omland, T. Targeting the endothelin system: A step towards a precision medicine approach in heart failure with preserved ejection fraction. Eur. Heart J. 2019, 40, 3718–3720.
- Ern Yeoh, S.; Docherty, K.F.; Campbell, R.T.; Jhund, P.S.; Hammarstedt, A.; Heerspink, H.J.L.; Jarolim, P.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; et al. Endothelin-1, Outcomes in Patients with Heart Failure and Reduced Ejection Fraction, and Effects of Dapagliflozin: Findings From DAPA-HF. Circulation 2023, 147, 1670–1683.
- Thorin, E.; Clozel, M. The cardiovascular physiology and pharmacology of endothelin-1. Adv. Pharmacol. 2010, 60, 1–26.
- Attinà, T.; Camidge, R.; Newby, D.E.; Webb, D.J. Endothelin antagonism in pulmonary hypertension, heart failure, and beyond. Heart 2005, 91, 825–831.
- Kostov, K. The Causal Relationship between Endothelin-1 and Hypertension: Focusing on Endothelial Dysfunction, Arterial Stiffness, Vascular Remodeling, and Blood Pressure Regulation. Life 2021, 11, 986.
- Khimji, A.K.; Rockey, D.C. Endothelin—Biology and disease. Cell. Signal. 2010, 22, 1615–1625.
- Böhm, F.; Pernow, J. The importance of endothelin-1 for vascular dysfunction in cardiovascular disease. Cardiovasc. Res. 2007, 76, 8–18.
- Boerrigter, G.; Burnett, J.C. Endothelin in neurohormonal activation in heart failure. Coron. Artery Dis. 2003, 14, 495–500.
More