Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Meng-Han Tsai and Version 2 by Wendy Huang.
Primary familial brain calcification (PFBC), also known as Fahr’s disease, is a rare inherited disorder characterized by bilateral calcification in the basal ganglia according to neuroimaging. Other brain regions, such as the thalamus, cerebellum, and subcortical white matter, can also be affected. Among the diverse clinical phenotypes, the most common manifestations are movement disorders, cognitive deficits, and psychiatric disturbances. Although patients with PFBC always exhibit brain calcification, nearly one-third of cases remain clinically asymptomatic.
- primary familial brain calcification
- SLC20A2
- PDGFRB
- PDGFB
- XPR1
- MYORG
- JAM2
- CMPK2
1. Introduction
To date, two inheritance patterns have been found in PFBC patients. Heterozygous variants in SLC20A2, PDGFRB, PDGFB, and XPR1 are responsible for autosomal dominant PFBC [1][2][3][4][6,7,8,9], while biallelic changes in MYORG, JAM2, and CMPK2 are associated with autosomal recessive forms of the disease [5][6][7][8][10,11,12,13]. At present, around 50% of patients with PFBC do not have a pathogenic variant in the seven currently known genes [9][2], which indicates a more diverse genetic heterogeneity.
PFBC is genetically heterogeneous. To date, seven genes have been associated with PFBC, including four dominant genes and three recessive genes (Table 1).
Table 1.
Summary of PFBC-causative genes.
| Gene | Locus | Mode of Inheritance | Protein | Expression | Function | Effect of Variant | Most Common Variant Type | References |
|---|---|---|---|---|---|---|---|---|
| SLC20A2 | Chr 8 | AD | Type III sodium-dependent inorganic phosphate transporter 2 (PiT2) | Ubiquitously, higher level in the brain | Uptake of inorganic phosphate (Pi) into cells | Loss of function | Missense | [1][10][11][12][3,6,41,42] |
| PDGFRB | Chr 5 | AD | Platelet-derived growth factor receptor-β (PDGFRB) | Neurons, vascular smooth muscle cells (SCMs), pericytes in the brain | Cell-surface tyrosine kinase receptors for the PDGF family, especially for homodimeric PDGF-B and PDGF-D; Essential for angiogenesis and formation of the blood–brain barrier (BBB) | Loss of function | Only missense | [2][9][10][13][2,3,7,43] |
| PDGFB | Chr 22 | AD | Platelet-derived growth factor subunit B (PDGFB) | Neurons and endothelial cells in the brain | Growth factors for mesenchymal cells; Crucial role in the proliferation and recruitment of pericytes and vascular SCMs | Loss of function | Missense | [3][10][14][15][3,8,44,45] |
| XPR1 | Chr 1 | AD | Xenotropic and polytropic retrovirus receptor 1 (XPR1) | Ubiquitously, higher level in the brain | Pi efflux from cells | Loss of function | Missense | [4][10][16][3,9,46] |
| MYORG | Chr 9 | AR | Myogenesis regulating glycosidase (MYORG) | Endoplasmic reticulum of the astrocytes in the brain | Member of the glycosyl hydrolase 31 family; Regulate protein glycosylation | Loss of function | Missense | [5][10][3,10] |
| JAM2 | Chr 21 | AR | Junctional-adhesion-molecule-2 (JAM2) | Endothelial cells and astrocytes in the brain | Member of the junctional adhesion molecules family; Crucial role in the regulation of cell polarity, endothelium permeability, leukocyte migration, and BBB function | Loss of function | Nonsense | [6][7][10][3,11,12] |
| CMPK2 | Chr 2 | AR | Uridine monophosphate-cytidine monophosphate kinase 2 (UMP-CMPK2) | Neurons and endothelial cells in the brain | Takes part in the salvage pathway for phosphorylation of dCMP, dUMP, CMP, and UMP in the mitochondria | Loss of function | Missense and start-codon loss | [8][17][13,47] |
Abbreviations: Chr: chromosome; AD: autosomal dominant; AR: autosomal recessive.
2. SLC20A2
The first PFBC-causative gene, SLC20A2, was identified in 2012 [1][6]. It is located on chromosome 8 and encodes for type III sodium-dependent inorganic phosphate (Pi) transporter 2 (PiT2). PiT2 has 12 transmembrane domains, and this protein is responsible for the uptake of Pi into cells [1][9][18][2,6,16]. SLC20A2 is expressed ubiquitously, but at a higher level in the brain, especially in the globus pallidus, thalamus, and cerebellum [11][41]. SLC20A2 is the most common PFBC gene; heterozygous variants have been identified in more than 60% of genetically confirmed PFBC patients [10][3]. A missense change is the most common variant type, followed by frameshift, nonsense, and splice site variations, without obvious hotspots for pathogenic variants (Figure 1a) [1][2][10][19][20][21][22][23][24][25][26][27][28][29][30][31][32][33][34][35][36][37][38][39][40][41][42][43][44][45][46][47][48][49][50][51][52][53][54][55][56][57][58][59][60][61][3,6,7,17,18,21,23,37,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85]. Functionally, both haploinsufficiency and dominant negative effects have been described; the loss of normal PiT2 function results in extracellular Pi accumulation and subsequent calcium phosphate formation [1][12][6,42]. Calcification around the blood vessels or within the vessel walls of involved brain regions has been demonstrated in Slc20a2 homozygous knockout mice (Slc20a2−/− mice) and in an autopsied SLC20A2-PFBC patient [62][63][64][86,87,88]. Calcification in Slc20a2−/− mice was also found inside cells, mainly in the pericytes and astrocytes, which suggested the intracellular cytosolic initiation of calcification [63][87]. Moreover, increasing T-cell infiltration in the brain parenchyma was found in Slc20a2−/− mice, which is positively associated with brain calcification and aging. Impaired blood–brain barrier (BBB) permeability with the enhancement of endocytosis and transcytosis was also demonstrated, which may be explained by the dysfunction of pericytes and astrocytes due to intracellular calcification [65][89]. In addition, PiT2 is known to be expressed in the apical membrane of choroid plexus epithelial cells in spiny dogfish and rats, suggesting that PiT2 plays an important role in actively transporting Pi from the cerebrospinal fluid (CSF) to the blood to maintain phosphate homeostasis in the CSF [66][90]. The level of Pi in CSF is significantly elevated in both Slc20a2 homozygous knockout mice and PFBC patients with SLC20A2 pathogenic variants [63][67][68][87,91,92]. In summary, PiT2 dysfunction can leads to a local increase in the extracellular and CSF Pi concentrations, which then trigger cell-mediated mineralization progression, ensuing calcification [62][63][86,87].
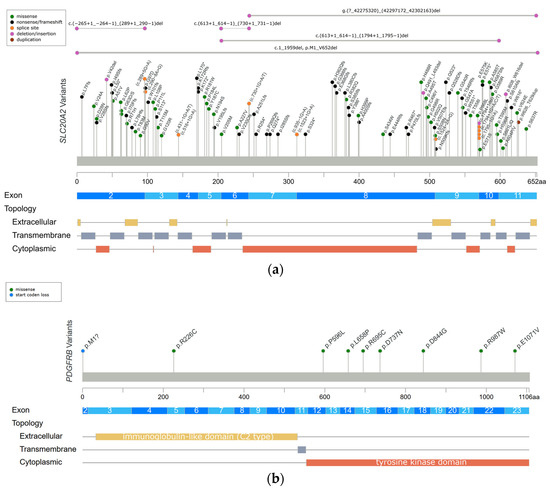
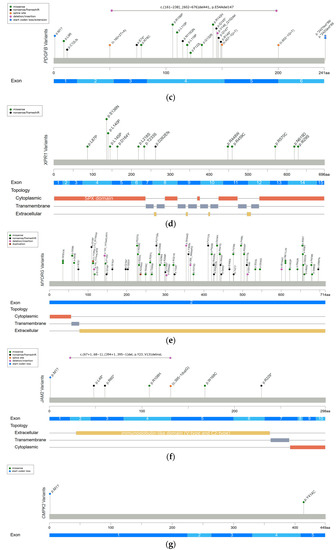
Figure 1. Reported variants in seven genes linked to PFBC along the protein sequence and their topologic protein models. (a) The reported variants in the SLC20A2 gene and topology protein model of PiT2. (b) PDGFRB gene and PDGF-Rβ. (c) PDGFB gene. (d) XPR1 gene and XPR1. (e) MYORG gene and MYORG. (f) JAM2 gene and JAM2. (g) CMPK2 gene. There is no obvious hotspot for SLC20A2, MYORG, and JAM2 genes. The variants tend to cluster in the tyrosine kinase domain of the PDGFRB gene, the mature protein product between positions 82 and 190 of the PDGFB gene, and in the SPX domain of the XPR1 gene. Meaning of symbols: *, stop codon; ?, unknown (a variant affecting the initiation codon cannot be predicted).
3. PDGFRB
The PDGFRB gene was identified in PFBC patients in 2013 [2][7], and it is located on chromosome 5 and encodes for platelet-derived growth factor receptor-β (PDGF-Rβ). The structure of PDGF-Rβ includes five extracellular immunoglobulin-like C2 type domains, a transmembrane domain, and a tyrosine kinase domain. PDGF-Rβ is a cell-surface tyrosine kinase receptor for members of the platelet-derived growth factor (PDGF) family, with a high affinity for homodimeric PDGF-B and PDGF-D. At the tissue level, the PDGFRB gene is highly expressed in the brain, especially in the basal ganglia and dentate nucleus of the cerebellum. At the cellular level, the PDGFRB gene is expressed in neurons, vascular smooth muscle cells (SCMs), and pericytes. The signal transduction of PDGF-Rβ and its ligand is essential for the proliferation and migration of vascular SCMs and pericytes, and subsequently, the angiogenesis and formation of the BBB [2][9][18][2,7,16]. Heterozygous variants in the PDGFRB gene have been identified in 5% of genetically confirmed PFBC patients [10][3]. The missense change is currently the only variant type to be identified in the PDGFRB gene. The variants tend to cluster in the tyrosine kinase domain (Figure 1b) [2][10][21][32][69][70][3,7,21,56,93,94], and they are likely to cause haploinsufficiency and affect the kinase function of the protein [13][43]. The functional loss of PDGF-Rβ may lead to pericytes dysfunction, which would impact BBB integrity and secondarily induce calcium depositions in the vessel walls or perivascular space. Several studies have shown that homodimeric PDGF-B can directly induce vascular SCM calcification via enhancing the expression of inorganic phosphate transporter 1 (PiT1) [71][72][95,96]. Hence, Nicolas et al. hypothesized that activating variants in PDGFRB may impact the PDGF-PiT1 pathway and cause vascular calcification [2][7]. Interestingly, PiT1 is encoded by the SLC20A1 gene, which is one of two type III sodium-dependent Pi transporters. The other is PiT2 encoded by SLC20A2 [2][70][7,94]. However, there is no further evidence supporting this hypothesis [73][14].
4. PDGFB
The PDGFB gene was also reported in 2013 [3][8], and it is located on chromosome 22 and encodes for the PDGF-B precursor protein. This precursor protein is cleaved at positions 81 and 191, and subsequently forms a homodimer through disulfide bonds, which is the main ligand of PDGF-Rβ [18][16]. The PDGFB gene is expressed in neurons and endothelial cells in the brain [3][8]. PDGF-B is a growth factor for mesenchymal cells and plays a crucial role in the proliferation and recruitment of pericytes and vascular SMCs. [14][15][44,45]. Heterozygous variants in the PDGFB gene have been identified in 12% of genetically confirmed PFBC patients [10][3]. The missense change is the most common variant type in the PDGFB gene, followed by nonsense, splice site, and extension variants. The variants cluster between protein positions 82 and 190, which are retained in the mature PDGF-B protein (Figure 1c) [3][10][19][32][35][45][58][74][75][76][77][78][79][80][81][82][3,8,17,56,59,69,82,97,98,99,100,101,102,103,104,105]. The same as PDGFRB does, PDGFB variants also cause haploinsufficiency, either by deleting critical parts of protein or disrupting normal protein function. The loss of normal PDGF-B function leads to BBB impairment via PDGF-Rβ, and then triggers the process of calcification [3][9][2,8].
5. XPR1
The XPR1 gene was identified in 2015 [4][9], and it is located on chromosome 1 and encodes for xenotropic and polytropic retrovirus receptor 1 (XPR1). XPR contains eight transmembrane domains and an amino-terminal SPX domain [18][16]. This protein mediates Pi efflux from cells [4][9][2,9]. XPR1 is expressed universally, and a high XPR1 mRNA level has been demonstrated in mouse brains, especially in the cerebellum and striatum [16][46]. Heterozygous variants in the XPR1 gene have been identified in 6% of genetically confirmed PFBC patients [10][3]. The missense change is the most common variant in XPR1-related PFBC patients, which tends to cluster in the SPX domain (Figure 1d) [4][10][29][32][83][84][85][3,9,19,53,56,106,107]. XPR1 variants may cause haploinsufficiency, leading to the intracellular accumulation of Pi and formation of calcium phosphate [4][9]. Interestingly, mutual interactions between XPR1 and PDGFRB were found in a recent immunoprecipitation study [16][46]. It is hypothesized that these two proteins may form a complex on the cell membrane, further suggesting that PDGFRB may be the upstream regulator of XPR1 [16][46].
6. MYORG
In 2018, the first and most common autosomal recessive PFBC-causative gene, MYORG, was identified. MYORG is located on chromosome 9 and encodes for myogenesis-regulating glycosidase (MYORG). It contains a short cytoplasm domain at the N-terminal, a transmembrane domain, and a long luminal fragment with a glycosidase domain at the C-terminal. MYORG is a member of the glycosyl hydrolase 31 family, and its function is to regulate protein glycosylation. In the brain, the MYORG gene is highly expressed in the cerebellum, specifically in the endoplasmic reticulum of the astrocytes [5][10]. Biallelic variants in the MYORG gene have been identified in 13% of genetically confirmed PFBC patients [10][3]. The missense change is the most common variant type in the MYORG gene, followed by in-frame indels, nonsense, and frameshift variations. There is no obvious hotspot of pathogenic variants (Figure 1e) [5][10][86][87][88][89][90][91][92][93][94][95][96][97][98][99][100][101][102][3,10,22,24,25,26,27,30,108,109,110,111,112,113,114,115,116,117,118]. Pathogenic variants cause the loss of the glycosidase function of MYORG, which may lead to abnormal protein glycosylation and metabolic disturbance. It is believed that MYORG variants can induce astrocyte dysfunction, which then disturbs the association between astrocytes and pericytes, resulting in neurovascular unit (NVU) dysfunction and subsequently causing the formation of brain calcification [5][10]. However, the exact linkage between the loss of protein glycosylation and astrocyte dysfunction remains to be elucidated.
7. JAM2
In 2020, another autosomal recessive PFBC-causative gene, JAM2, was identified. JAM2 is located on chromosome 21 and encodes for junctional-adhesion-molecule-2 (JAM2). The structure of JAM2 includes two immunoglobulin-like domains (V-type and C2-type). JAM2 is a member of the junctional adhesion molecule family, and it plays crucial roles in the regulation of cell polarity, endothelium permeability, leukocyte migration, and BBB function [6][7][11,12]. In the brain, JAM2 is highly expressed in the caudate nuclei. At the cellular level, JAM2 is specifically expressed in endothelial cells and astrocytes [7][12]. Biallelic variants in the JAM2 gene have been identified in 2% of genetically confirmed PFBC patients [10][3]. The nonsense change is the most common variant type in the JAM2 gene. Missense, frameshift, and structural variants have also been reported, without a mutation hotspot (Figure 1f) [6][7][10][3,11,12]. Variants of JAM2 gene cause the loss of cell–cell adhesion and the dysfunction of the solute passage, which may contribute to the formation of brain calcification [6][7][11,12].
8. CMPK2
The CMPK2 gene is the latest autosomal recessive PFBC-causative gene to be identified at the end of 2022 [8][13]. This gene is located on chromosome 2 and encodes for uridine monophosphate-cytidine monophosphate kinase 2 (UMP-CMPK2), which can be separated into N-terminal and C-terminal domains according to the sequence properties. CMPK2 is a member of the nucleoside monophosphate kinase family and participates in the salvage pathway for the phosphorylation of dCMP, dUMP, CMP, and UMP in the mitochondria [17][47]. In the brain, the CMPK2 gene is highly expressed in the hippocampus and cerebellum. At the cellular level, CMPK2 is specifically expressed in neurons and vascular endothelial cells [8][13]. To date, biallelic variants in the CMPK2 gene have only been reported in two PFBC families, which carry missense and start-codon loss variants (Figure 1g) [8][13]. The loss of UMP-CMPK2 function leads to a reduction in mitochondrial genome DNA copy numbers, the downregulation of the expression of mitochondrial protein, the decrease in ATP production, and the disturbance of mitochondrial cristae morphology. The disturbance of mitochondrial function is believed to cause impairment of energy homeostasis and the upregulation of intracellular phosphate levels, subsequently triggering the development of brain calcification [8][13].