2. Causes of Skin Pigmentation
2.1. Genetics
Unexpectedly, 125 genes can influence skin tone. The production of melanin, as depicted in
Figure 1, is governed by genes and hormones. A person has control over his or her skin’s ability to function and live, as well as how much pheomelanin or eumelanin they produce by, for instance, deciding how much sun exposure they receive, or the amount of drugs and cosmetics they use. These elements could alter the tone of skin over time
[1]. Thus, one of the most frequent reasons for skin color is genetics. Genetics may be able to predict how many melanocytes each individual will have. It is melanocytes, which are skin cells, that make melanin. However, during hyperpigmentation and tanning, melanosomes (the organelles that contain melanin) must be transported and expanded, but during hypopigmentation, melanosomes decrease
[11]. Melanin, the pigment that gives skin its color, is more likely to be present in larger concentrations in people with darker skin tones. For example, individuals with darker skin tones frequently have higher melanin levels than those with lighter skin tones
[12][13][14][12,13,14].
2.2. Sun Exposure
Sun exposure is a common cause of skin pigmentation. The body produces more melanin, in order to defend itself against UV rays from the sun. This may make the skin more pigmented, to shield it from the sun’s rays.
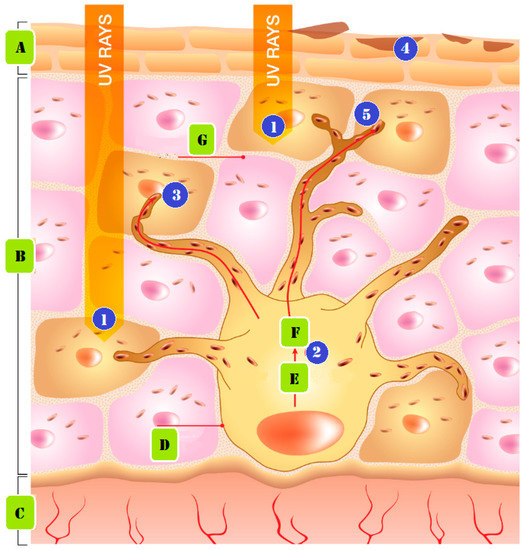
Figure 2 demonstrates how persistent UV exposure leads to the emergence of pigmentation. The following phases make up the formation mechanism. (1) UV radiation produces free radicals. (2) The free radicals and UV light activate biological agents that impact melanocytes, the cells responsible for creating pigment. (3) The enzyme tyrosinase transforms the amino acid tyrosine into melanin pigments, which can be either red or brown in color. (4) Biological substances act to increase the activity of the enzyme Tyrosinase, which generates pigment. (5) Melanin is lost from the skin, as skin cells travel to the surface layers and are shed during the skin’s natural exfoliation process. Melanin is delivered as granules from nearby keratinocytes, to give the skin its color
[4][14][15][4,14,15].
Figure 2.
Pigmentation from prolonged UV exposure formed: (A) stratum corneum, (B) epidermis, (C) dermis, (D) melanocyte cell, (E) tyrosinase and tyrosine, (F) melanin, and (G) keratinocyte cell.
2.3. Medications
Several medications may also lighten the skin’s pigment. One class of drugs, antibiotics, can boost melanin synthesis, increasing skin color. When certain medications, such as birth control pills, are taken together, skin pigmentation may also intensify. A person taking medicine should speak with their doctor to find out if the medication could impact the color of their skin
[16][17][16,17].
3. Types of Pigmentation Disorders
While they are ill, a person’s skin tone may alter, becoming lighter (hypopigmentation) or darker (hyperpigmentation). Melanin, the pigment that regulates skin color, is produced less frequently by the body, which results in hypopigmentation. Hyperpigmentation, on the other hand, is an increase in melanin synthesis
[4][5][18][4,5,18].
3.1. Causes of Hypopigmentation
Prior skin trauma, including skin sores such as blisters, infections, burns, exposure to chemicals, and other wounds, is the most common cause of low melanin content (hypopigmentation). After an injury has healed, the skin will be paler than the surrounding skin surface
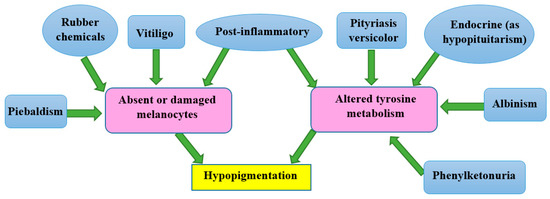
[19]. Other genetic diseases can result in hypopigmentation in different parts of the skin. Hereditary disorders such as albinism, melasma, fungal infections, pityriasis versicolor, pityriasis alba, and vitiligo can result in hypopigmentation, as seen in the mechanism in
Figure 3. At birth, albinism is caused by a genetic abnormality known as low melanin concentration. The prevalent physical traits of albinos include a white complexion, dark blue eyes, and white hair
[20][21][20,21]. The genetic melasma condition can cause brown or blue-gray spots to develop on a person’s arms or face. Hormones, sun exposure, or contraceptive medication may bring it on
[22][23][22,23].
Figure 3. The mechanisms involved in some types of hypopigmentation.
Despite the fact that the Malassezia genus is responsible for the widespread fungal infection known as tinea versicolor, also known as pityriasis versicolor, it is possible for fungi to infect humans, and change the color of their skin. Small regions of discoloration are brought on by Malassezia’s alteration of the skin’s normal melanin pigmentation. The patches on the shoulders and buttocks may be lighter or darker than the overall healthy skin tone
[24][25]. Pityriasis alba is a skin condition that typically affects adolescents and teenagers, and is characterized by oval or circular hypopigmented lesions with soft scales. Lesions on the face, upper body, and arms, which are more noticeable in those with darker skin tones, may be modestly erythematous, before becoming hypopigmented
[25][26].
Depigmentation, which happens when the skin entirely loses pigment and turns white, is another prevalent hypopigmented skin disease. An example of this is the auto-immune condition vitiligo, which is characterized by macules of a white chalky substance on the skin, and melanocyte loss, a common cause of depigmentation. Vitiligo causes smooth, white patches to appear on the skin. Many times, vitiligo is dismissed as a minor problem
[26][27][27,28].
3.2. Causes of Hyperpigmentation
A rise in melanin production causes hyperpigmentation. Examples C and D in
Figure 3, and other situations where melanin synthesis increases, primarily result from sun exposure, dermatological conditions, hormones, age, hereditary factors, skin injuries or inflammation, and acne
[28][24]. The most frequent cause of hyperpigmentation is exposure to the sun, which heavily stimulates melanin production. A recent study (
Figure 2) demonstrated how early sun exposure might worsen dark spots, by making them resemble melasma, post-inflammatory spots, and age spots
[28][24]. Two examples of hyperpigmentation brought on by hormonal factors are chloasma and melasma. It has been established that the female sex hormones estrogen and progesterone, which boost melanin formation when the body is exposed to sunshine, are to blame for this disease, which is prevalent in women. Hormone replacement therapy has the adverse effect of hyperpigmentation
[29].
Melanocyte counts decline with age, but those that are still present grow and specialize. These physiological alterations show how aging becomes increasingly obvious in people over 40
[30]. Genetics has an impact on pigmentation. The development of the melanocyte function, which impacts skin color, requires particular genes
[31]. According to the term “post-inflammatory hyperpigmentation”, this appears following several types of skin inflammation or injury, including chemical exposure, burns, wounds, psoriasis or atopic dermatitis, and acne. The skin looks more discolored and blacker after the lesion has healed
[27][28]. The innermost layer of the skin, the dermis, can get infected by papules, pustules, and acne. Unusually dark spots form when skin diseases induce an abnormally high melanin synthesis. Similarly to this, the real causes of the hyper-pigmentation problem are infections of the fatty glands and hair follicles. Mild acne typically doesn’t cause hyperpigmentation. Acne lesions that have been squeezed, squashed, or penetrated will also darken and become more pigmented
[32]. Some causes of hyperpigmentation include pregnancy-related birthmarks, age spots, acne scars, and a number of drugs, including antibiotics, birth control pills, antimalarials, and tricyclic antidepressants. A rare condition called Addison’s disease results in black skin patches and decreased adrenal gland activity. Hyperpigmentation can occasionally occur after laser or light treatment
[33].
4. Drugs for Treatment of Skin Pigmentation
Despite being well-recognized for many years, drugs for skin pigmentation have only recently become more widely available. Topical creams and oral pills are the primary medications for skin pigmentation. It would be best to balance the advantages and disadvantages of both medicines to choose which is most beneficial
[33][34][33,34].
4.1. Oral Medications
Oral medicines are a potential substitute for treating skin ailments, and modifying skin tone. Such drugs are beneficial because they are more potent than topical creams, and do not need to be applied or disposed of as frequently as topical creams. However, there are certain drawbacks to taking oral medications. They can be expensive and cause more significant side effects than topical therapies
[35].
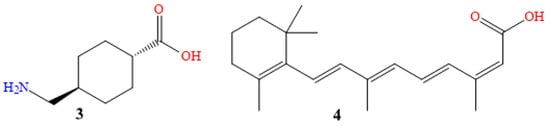
Compound
3 in
Figure 4 is tranexamic acid (Traxamac
® 250 mg), one of several coagulation modifiers. In addition to its use on eczema, melasma, other associated ailments, toxic reactions, and urticaria, and its effects on erythema, itching, swelling, and other recognized symptoms, it has also been used to treat various illnesses. A plasmin inhibitor, tranexamic acid prevents the plasminogen activator from converting plasminogen to plasmin, by reversibly shutting off lysine binding sites on plasminogen molecules. This reduces atypical fibrinolysis, and prevents blood loss. According to recent studies, tranexamic acid helps tyrosinase to untangle tangles. It might avoid and stop hyperpigmentation, by reducing melanin production. It is a widely used pharmaceutical technique that is easily accessible and effective against pigment spots. Although it inhibits the effects of tyrosinase, and changes the relationship between keratinocytes and melanocytes, it decreases dermal vascularity, and lessens melanin production
[36][37][38][39][40][36,37,38,39,40].
Figure 4. Chemical structures of tranexamic acid (3), and isotretinoin (4).
Using tranexamic acid orally, in a dosage of 250 mg twice daily for six months, on 75 patients, a clinical and photographic evaluation revealed an initial decline in melasma after the first month for 82.4% of patients, and 94.6% in the second month. The development of pigmentation had been used to measure the treatment’s success (excellent if >90%, good if >60%, fair if >30%, and poor if 30%). After six months, the overall development rate was 95.9%, with 10.8% being excellent, 54% being good, and 31.1% being fair, which is evidence that oral tranexamic acid is a safe and effective melasma treatment
[41][42][41,42].
Mexameter
® was utilized to evaluate the suggested lesional melanin index (MI) ranks, and the erythema index (EI) scores, for 25 patients who received 1500 mg twice daily for two months. Both of these scores fell off dramatically. Histological examination confirmed significant decreases in mast cell counts, vessels, and epidermal pigmentation. Here is an illustration of how oral tranexamic acid reversed melasma-related dermal changes, including increased vascularity, decreased mast cell populations, and decreased melasma-related epidermal pigmentation
[43][44][43,44].
25 women, certain sides of the face received twice-daily applications of 5% topical tranexamic acid for 12 weeks, as a melasma treatment. The Mexameter and Melasma Area and Severity Index (MASI) results revealed a notable drop in the MI and MASI scores. Additionally, for 12 weeks, 23 melasma patients applied a 2% tranexamic acid emulsion twice daily to their whole faces. With a rise in the lightness values, and a decrease in the erythema values, the mMASI and chromameter results showed a significant improvement in the fourth and eighth weeks
[45][46][47][45,46,47].
Isotretinoin is the 13-cis-retinoic acid derivative of vitamin A (Isotane
® 20 mg, molecule
4 in
Figure 6)
[48][49][50][48,49,50]. In treating acne vulgaris, oral isotretinoin exerts its effects by reducing sebaceous gland activity, the development of
Propionibacterium acnes, and inflammation. This facilitates pore cleaning, and inhibits the growth of new lesions
[51][52][53][51,52,53].
The administration of 20 mg of Accutane (isotretinoin) orally was randomly assigned to 60 patients (aged 35 to 65); 42 of the women, and 18 of the men. It was administered three times a week for no more than two months, and tracking continued for months after the study was over. The 60 patients reported reductions in their wrinkles, pore thickness, and pore size. They noticed that the skin became significantly smoother and lighter in color. Both the elasticity and the tone of the skin improved. Additionally, they noticed a decrease in pigmented lesions and hyperpigmentation
[54][55][54,55].
The severity of acne was assessed using the MASI for 30 individuals of either sex who were receiving 20 mg of isotretinoin as a monotherapy, and were between the ages of 18 and 25. A reduction of roughly 73.4% was seen in patients who took 20 mg of oral isotretinoin for 16 weeks
[56][57][56,57].
4.2. Topical Creams
Topical creams are the most common type of drug used to treat skin pigmentation. They are applied directly to the affected area, and can lighten or darken the skin. The main advantage of topical creams is that they can be used at home, and do not require a trip to the doctor. Additionally, they are typically less expensive than oral medications. Topical cream application, however, comes with several drawbacks. They can be messy and time-consuming to apply, and they may only sometimes be as effective as oral medications
[58][59][58,59].
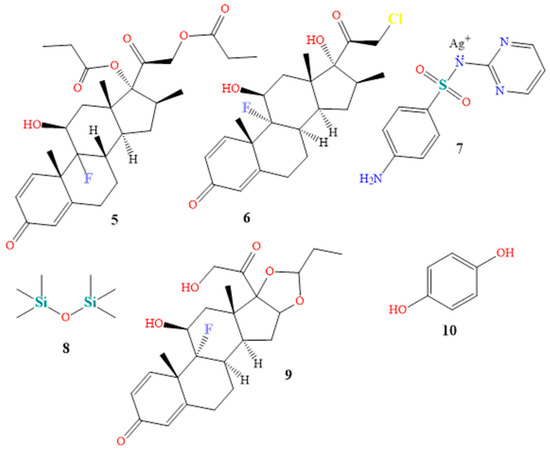
Topical steroids are the most often recommended drug in dermatology. They are prescribed for various conditions, including eczema, psoriasis, atopic dermatitis, lichen simplex chronicus, intertrigo, and psoriasis, due to their immunosuppressive, anti-mitogenic, and anti-inflammatory characteristics. The dosage varies from one to three times per day. Betamethasone 0.05% (Betnovate-N
®, chemical
5 in
Figure 5) and clobetasol 0.05% (Dermovate
®, compound
6 in
Figure 5) are examples of topical steroids. The NF-Kappa B inhibitors betamethasone and clobetasol are glucocorticoids that prevent neutrophil apoptosis and demarginating. Betamethasone and clobetasol are phospholipase A2 inhibitors, which also reduce the production of arachidonic acid derivatives. Additionally, glucocorticoids encourage the anti-inflammatory gene interleukin-10
[60][61][62][60,61,62], a common ingredient in cream or ointment treatments. Numerous local and systemic adverse effects of topical steroids have been attributed to their continuous use
[63][64][65][63,64,65].
Figure 5. Chemical structures of betamethasone (5), clobetasol (6), silver sulfadiazine (7), dimethicone (8), triamcinolone (9), and hydroquinone (10).
A total of 15 vitiligo patients of both sexes (F:M 1.14:1) utilized betamethasone cream 0.05% twice daily throughout a three-month study. Based on a patient’s degree of minimal pigmentation/no reaction, moderate, noticeable pigmentation, or outstanding pigmentation, the improvement of each patient was rated as (25%), (25–50%), (50–75%), or (>75%), respectively. Compared to 40.0% of patients with limited pigmentation or no reaction, 46.7% and 13.3% showed a moderate or outstanding pigmentation response after therapy
[66][67][66,67].
A total of 731 patients with moderate to severe plaque psoriasis, with 3% to 20% body surface area, participated in the 4-week Clobetasol Spray trial, which used two doses of clobetasol propionate spray 0.05% twice daily as treatment. The change in target plaque severity was the primary outcome measure. According to the major outcome measures scale, 80.0% of the patients in the therapy group were clear or nearly unambiguous, and showed a decrease in severity from the beginning
[68][69][68,69].
A topical anti-infective cream, silver sulfadiazine (Silvadene
®, chemical
7 in
Figure 5) is primarily used to prevent and cure burn injuries. Silver sulfadiazine solution with 1% API dissolves in water. Proteins become denaturized and enzyme activity is reduced by silver ions. Additionally, silver ions bind to proteins and surface membranes, leading to membrane proton leakage and cell death. Sulfadiazine competitively inhibits PABA, a naturally occurring bacterial substance that acts as a substrate for the dihydropteroate synthase enzyme. These organisms must carry out the blocked process to produce folic acid
[70]. Silver sulfadiazine exhibits broad-spectrum action against both gram-positive and gram-negative pathogens. It has been demonstrated that it promotes wound and injury repair, and has anti-infective qualities
[71][72][71,72]. Twenty-seven individuals with 2° burn injuries were randomly assigned to receive silver sulfadiazine throughout a 4-week study. After four weeks of treatment, the healing condition of 2° deep dermal burn wounds were determined to be (0–25%), (26–50%), (51–75%), or (76–100%), respectively, as poor healing, moderate healing, fast healing, or excellent healing. While eight and thirteen patients showed a mild and quick recovery, respectively, six patients with 2° deep dermal burn lesions showed poor healing
[73]. Mixtures of creams, shampoos, powders, mouthwash, and gels contain both an anti-infective and a steroid component, to treat skin or scalp infections
[74]. Triamcinolone and dimethicone are ingredients in the drug TriHeal80
® (see components
8 and
9 in
Figure 5). Topical corticosteroids produce similar antipruritic, anti-inflammatory, and vasoconstrictive effects
[75].
Triamcinolone is a phospholipase A2 inhibitor that acts on cell membranes, to prevent the lysosomal membranes of leukocytes from rupturing. This prevents the production of arachidonic acid, which in turn lowers lipoxygenase and cyclooxygenase, while inhibiting the production of prostaglandins and leukotrienes
[76][77][76,77]. Dimethicone, a silicone oil, exhibits viscoelastic qualities. It has moisturizing properties, and is utilized as a surfactant, antifoaming agent, and lubricant to cure skin irritation. To reduce the rate of water evaporation, dimethicone is used topically
[78][79][78,79]. When used four times per day for two months, and monitored for another two months, triamcinolone 0.1% mouthwash successfully treated oral lichen planus in 20 patients. All effectiveness endpoints, assessed using the visual analog scale, the verbal health impact profile score, and the objective clinical score, revealed a significant improvement in the patients
[80][81][82][80,81,82].
Under the brand name Tri-Luma
®, a triple combination cream is sold that includes the active components tretinoin, hydroquinone, and fluocinolone in concentrations of 0.01%, 4%, and 0.05%
[83]. Hydroquinone is the most frquently used skin-lightening or depigmenting substance (compound
10 in
Figure 5). It treats dyschromic skin diseases such as melasma, chloasma, freckles, and post-inflammatory hyperpigmentation, by suppressing melanin production. It stops tyrosinase from converting L-3,4-dihydroxyphenylalanine into melanin, due to its structural similarity to a specific analog of melanin
[83][84][85][83,84,85]. Fluocinolone (molecule
11 in
Figure 6) treats symptoms, including itchiness, swelling, and redness caused by skin problems
[86][87][86,87]. Retinol (compound
12 in
Figure 6) cures skin aging. It has been shown that it might be beneficial for concerns related to skin aging. The most remarkable feature is that treatment results manifest eight to twelve months after using the tretinoin 0.1% cream preparation. The most frequent side effects of tretinoin include very slight skin irritability, and a transient, mild, and clinically uncomfortable burning sensation
[85][88][89][85,88,89]. Sixty patients with moderate (grade 2) or severe (grade 3) melasma received treatment for eight weeks with the triple combination cream. At weeks 4, 6, and 8, the triple combination cream significantly improved the overall results, with an improvement rate of 73% (44/60). The percentage of participants who thought the triple combination cream was “excellent” as a treatment was 50%, while the most frequently mentioned adverse effects were erythema, burning, and desquamation
[90].
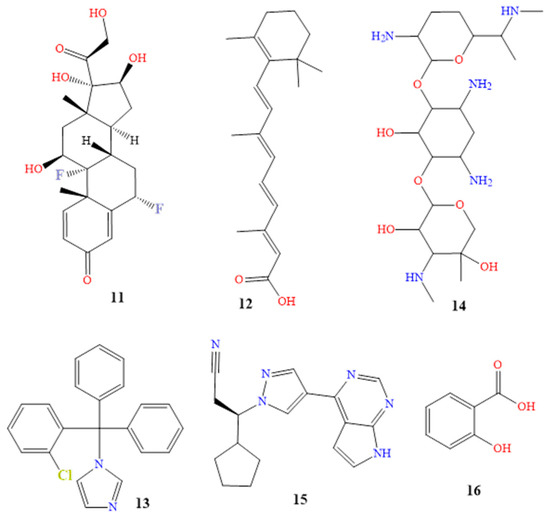
Figure 6. Chemical structures of fluocinolone (11), tretinoin (12), clotrimazole (13), gentamicin (14), ruxolitinib (15) and salicylic acid (16).
Additionally, a 12-week open-label trial was created, to gauge the effectiveness and safety of applying topical retinol 0.15% twice daily. At the fourth, eighth, and twelve weeks, it was found that 39%, 77%, and 77% of patients, respectively, showed significant improvement. When using topical retinol, dryness, erythema, peeling, stinging, and burning were some side effects that were reported
[91].
Dermatitis, eczema, rashes, and allergies are just a few of the skin conditions that TriDerm
® is used to treat. The swelling, redness, and itching that are brought on by these various disorders are reduced by triamcinolone. It includes corticosteroids that range in strength from mild to potent. The mechanism of action of TriDerm is composed of betamethasone, clotrimazole, and gentamicin (compounds
13 and
14 in
Figure 6). This results in the antipruritic, anti-inflammatory, and vasoconstrictive effects of betamethasone, as well as the broad-spectrum bactericidal antibiotic effect of gentamicin, and the broad-spectrum antifungal effect of clotrimazole. The contents of the cell leak out when clotrimazole reacts with the fungal cell membrane. Gentamicin is an effective topical skin therapy for bacterial infections
[91][92][93][94][95][91,92,93,94,95]. A study included 68 patients with itchy dermatoses, including atopic dermatitis, contact dermatitis, and true eczema. Of the patients, 33 received a twice-daily application of a topical cream containing betamethasone, clotrimazole, and gentamicin on the affected body parts. The effectiveness of the therapy was assessed after 7, 14, and 28 days. On the seventh day of treatment, there was a reduction in the inflammatory process and subjective symptoms. Of the 33 patients, 5 saw a scientific recovery on the fourteenth day of receiving treatment. After 28 days of therapy, the patients had fully recovered medically
[96].
The main component of the topical anti-cancer drug Opzelura
® is ruxolitinib (compound
15 in
Figure 6). A class of drugs known as Janus kinase inhibitors, which includes roxolitinib, has an effect on the immune system. JAK inhibitors may reduce the immune system’s ability to fight off infections
[97][98][99][100][97,98,99,100]. JAKs serve a variety of purposes. JAK1 and JAK3 increase lymphocyte existence and differentiation, whilst JAK2 increases the signal transduction of thrombopoietin and erythropoietin. JAKs are located in the cytoplasmic region of cytokine and growth factor receptors. JAKs are also activated, and undergo cross- and tyrosine phosphorylation. Ruxolitinib has a low affinity for JAK3, but is a solid and selective inhibitor of JAK2 and JAK1. Ruxolitinib reduces the plasma levels of pro-inflammatory cytokines, and inhibits myeloproliferative neoplasms by downregulating the JAK-STAT pathway
[101][102][101,102].
Randomized controlled trials recommended using ruxolitinib 1.5% cream for treating vitiligo twice daily in various patients. This was shown to demonstrate clinically excellent re-pigmentation of all body areas, including the acral region, after 24 weeks, with continued improvement through week 52. It was tolerated well in patients with long-standing high contamination
[103][104][103,104].
Salicylic acid (Salvax
®, compound
16 in
Figure 6), podophyllum resin (Podocon-25
®, compound
17 in
Figure 7), and podofilox (Condylox
®, compound
18 in
Figure 7) are a few examples of topical keratolytics that are administered topically to the skin, to soften keratin. This facilitates the peeling of skin cells, supports the skin’s capacity to retain moisture, and aids in the treatment of dry skin conditions, and is generally used to treat skin diseases, such as psoriasis, warts, keratoses, and acne
[105][106][105,106].
Figure 7. Structures of podophyllum resin (17), podofilox (18), aloin (19), kojic acid (20) phlorotannins (21), octaphlorethol A (22), fucoidan (23), and fucoxanthin (24).
Because of its keratolytic qualities, salicylic acid, a lipophilic B-hydroxy acid, is frequently used in cosmetic product formulations as a skin scaler for lightening. Arachidonic acid is reduced from converted prostaglandins and thromboxanes by COX-1 and COX-2 inhibitors. Salicylic acid also has anti-inflammatory and antibacterial effects
[107][108][107,108]. Twenty Latin American women over the age of 18 with moderate to severe bilateral melasma participated in a small, potential randomized controlled trial to compare the efficacy of salicylic acid 20–30% scaler every two weeks, followed by up to eight weeks, in combination with hydroquinone 4% twice daily for 14 weeks, versus hydroquinone 4% alone. A narrowband reflectance spectrophotometer (Mexameter MX-16) was used to quantify the degree of pigmentation on the affected and unaffected skin on each face. The Melasma Area and Severity Index (MASI) was used to assess the severity of the melasma. Of the patients, 33% were regarded as showing a mild development and slight improvement, with 44% showing more significant progress on the peeled side. One patient (6%) was noted to show only slightly more growth on the unpeeled side. The peeled side had advanced more than the unpeeled side, according to 83% of the nonblinded patients (four somewhat, seven moderately, and four significantly). One patient (6%) thought the unpeeled side was more advanced, whereas twelve percent (12%) believed there was no difference.
5. Natural Hyperpigmentation Treatment
Despite the wide range of therapies available, a growing number of people are choosing plants and natural items as alternatives. Plant-based and natural remedies have long been used to treat skin issues, and they are gaining popularity as a secure and efficient method to treat skin hyperpigmentation
[87][109][110][111][112][87,116,117,118,119].
Vitamins A, B, C, and E can all be used to address skin pigmentation problems, and are necessary for healthy skin. Each vitamin, which can be obtained from foods or supplements, has specific advantages
[113][114][120,121].
Niacin, pantothenic acid, and biotin are the B vitamins most frequently found in skincare products. Niacin, also known as niacinamide, is a vitamin that is used in face creams and masks, to minimize the appearance of enlarged pores, fine lines, and dullness. Pantothenic acid is also applied to dry, flaky skin, as a moisturizer. Numerous hair, nail, and skincare products include biotin
[115][116][122,123]. Ascorbic acid (vitamin C), an antioxidant, inhibits tyrosinase by binding to copper, and suppressing the oxidative polymerization of melanin precursors, which prevents melanin synthesis in the melanogenesis pathway
[117][118][124,125]. A statistically significant decrease from the baseline to week 16 was observed in a trial on 39 patients, using 25% L-ascorbic acid dissolved in Nmethyl-2-pyrrolidone and dimethyl isosorbide, as indicated by MASI values and mexameter data
[119][120][111,112]. A particular type of vitamin E is alpha-tocopheryl acetate. When fat is subjected to oxidation, and during the spread of free radical reactions, vitamin E, a powerful chain-breaking antioxidant, prevents the synthesis of reactive oxygen species molecules
[121][122][123][126,127,128].
Artocarpus lakoocha and
Glycyrrhiza glabra extracts have been reported to exhibit tyrosinase inhibitory effects and melanin pigment reduction. For the treatment of hyperpigmentation, the combination of 9:1
Artocarpus lakoocha and
Glycyrrhiza glabra decreased melanin pigment by up to 53% in B16 cells, by lowering the production of tyrosinase (TYR), microphthalmia-associated transcription factor (MITF), and tyrosinase-related protein-2 (TRP-2)
[124][125][126][129,130,131].
Antioxidants and fatty acids included in oils such as rosehip, jojoba, and argan oil aid in reducing inflammation, and brightening the skin. Natural oils can also shield the skin from the effects of the environment, preventing further discoloration. Aloe vera also includes aloin (compound
19 in
Figure 7), which has been demonstrated to lighten skin, and function well as a nontoxic hyperpigmentation therapy. Sharique described aloe vera as a natural depigmenting ingredient
[127][128][129][132,133,134].
When used as an emollient, jojoba oil exhibits first-rate lubricity, without having an oily or greasy texture, in single-segment and emulsion structures. It can also contribute to the skin’s effective water regulation during transpiration, reducing evaporation without obstructing the passage of gases or water vapor
[130][131][132][133][135,136,137,138]. According to a study, jojoba oil (or its ozonized or hydrogenated derivatives) has emollient properties. The study discovered that a significant increase in skin surface flexibility developed within 5 min and persisted for hours, suggesting a potential application in solutions for dry skin
[134][139]. Jojoba liquid wax was found to be just as effective at treating diaper rash as triamcinolone acetonide, nystatin, neomycin, and gramicidin. Jojoba oil is also an anti-inflammatory. Due to the absence of systemic adverse effects, jojoba has the benefit of being safer
[135][140]. Additionally, it has anti-acne and anti-psoriasis qualities, which allow the dissolution of sebum deposits through the hair follicles, due to its capacity to infiltrate the follicles, eliminate the comedones, and clear the skin
[136][141].
In a research study, ten women used argan oil as a bandage on their skin for 28 days. None of the women experienced itching, or noticed any skin irritation or redness, demonstrating the oil’s efficacy in reducing the amount of pigmentation. These women did observe a minor decrease in melanin content in the vicinity of the bandage, though, which lends credence to the idea that the oil lessens pigmentation
[137][138][139][113,114,115]. Licorice root extract, turmeric extract, and green tea extract are other herbal extracts high in antioxidants that help to reduce inflammation and brighten the skin.
Since ancient times, licorice root extract has been utilized for its medical benefits, particularly for skin care. It contains glycyrrhizin, which has been shown to have antioxidant and anti-inflammatory properties
[140][142]. Given that it is thought to help enhance skin appearance and treat some skin disorders, these qualities make it a popular ingredient in skincare products
[141][143]. Several research studies have been conducted to determine whether licorice root extract is effective for treating skin conditions. According to a study, licorice root extract is useful for reducing hyperpigmentation and lightening the skin
[142][144]. Atopic dermatitis symptoms may be lessened by licorice root extract, according to a different study
[143][145]. James M. Spencer also demonstrated in his research that licorice root extract was efficient in lessening the severity of rosacea, melasma, and acne
[144][146]. Additionally, licorice root extract reduced the appearance of black spots and redness, as was discovered in a 2019 study by Maria Yusuf Dhariwala
[145][147].
Since ancient times, turmeric extract has been valued for its therapeutic benefits. It has a yellow tint, and various health advantages, due to the presence of the active component curcumin, when it comes to pigmentation and skin conditions. The strong anti-inflammatory qualities found in curcumin can help lessen the skin inflammation brought on by a variety of skin conditions, including psoriasis and eczema
[146][147][148][149][148,149,150,151]. Antioxidants included in turmeric extract reduce oxidative damage that can cause skin aging, and pigmentation disorders such as melasma, by neutralizing free radicals
[150][152]. Curcumin also has skin-lightening qualities. By preventing the formation of the melanin-producing enzyme tyrosinase, it can lessen hyperpigmentation, and make the skin lighter
[151][153]. Curcuminoids, which are found in turmeric, have exfoliating qualities that aid in gently removing dead skin cells, and encourage skin regeneration, minimizing the appearance of hyperpigmentation and dark patches
[152][154]. The use of turmeric extract to treat skin issues was the subject of a 2018 study by Alexandra R. Vaughn. In psoriasis, eczema, and acne patients, the study found that turmeric extract was beneficial in lowering skin inflammation, and enhancing skin health
[153][155]. According to a 2018 study by Penelope J. Kallis
[154][156], a topical cream with turmeric extract proved successful in lowering the severity of acne in patients after four weeks of treatment.
Another organic component that has been investigated for its therapeutic advantages for the skin is green tea extract. It has many polyphenols and antioxidants, as well as anti-inflammatory and skin-protective qualities
[155][156][157][157,158,159]. Green tea extract works in a variety of ways, to treat pigmentation issues and skin problems. Catechins and epigallocatechin gallate (EGCG), two antioxidants found in green tea, work to combat free radicals that can damage skin and speed up the aging process
[158][160]. Green tea extract also has strong anti-inflammatory qualities that can help lessen the skin irritation brought on by a variety of skin diseases, such acne, eczema, and rosacea
[159][161]. The EGCG in green tea extract can help inhibit tyrosinase activity, reducing the production of melanin, and thus lightening the skin
[160][162]. Furthermore, green tea extract has been shown to offer some protection against UV radiation, which can cause skin damage and contribute to pigmentation disorders
[161][163]. A clinical study was conducted on 11 patients to investigate the use of green tea extract in treating acne; this found that green tea extract was effective in reducing the number of acne lesions and improving overall skin health
[162][164]. Another study, published in 2018, found that green tea extract effectively reduced the appearance of fine lines and wrinkles in the skin
[163][165].
Kojic acid (Enshine
® cream 2%, compound
20 in
Figure 7) has been found to be effective in treating various skin disorders and pigmentation issues, due to its mechanism of action. It works by inhibiting the activity of tyrosinase, which reduces the production of melanin, which can help to fade dark spots and hyperpigmentation
[164][165][166][166,167,168]. In addition to its tyrosinase-inhibiting properties, kojic acid has antioxidant and anti-inflammatory properties; these can be particularly beneficial to individuals with acne, rosacea, and other inflammatory skin conditions
[167][168][169][170][169,170,171,172]. One study, published in 2016 by Peter J. Gust, evaluated the efficacy of a cream containing 2% kojic acid, 10% glycolic acid, and 2% hydroquinone for treating melasma. The study involved 40 participants, who applied the cream twice daily for 12 weeks. The results showed a significant reduction in the severity of melasma in the treated group, compared to the control group, with no reported adverse effects
[171][173]. In another study, Tamara Searle investigated the use of a cream containing 2% kojic acid, 1% arbutin, and 5% vitamin C to treat age spots. The study involved 60 participants, who applied the cream twice daily for 12 weeks. The results showed a significant reduction in the number and severity of age spots in the treated group, compared to the control group, with no reported adverse effects
[172][174].
Phlorotannins (compound
21 in
Figure 7) from brown algae (brown seaweed) play a crucial role in the reduction of hyperpigmented effects, and the prevention of premature skin aging. They protect the skin from the sun’s infrared and blue rays.
Additionally, they promote cellular energy generation, which raises the oxygenation of the skin. Through this technique, the skin’s overall appearance and cell innovation are improved. Their antioxidant action prevents the collagen that firms the skin from degenerating
[173][174][175][175,176,177]. Phlorotannins have been studied for their impact on skin conditions and pigmentation, in clinical trials and meta-analyses. A randomized, double-blind, placebo-controlled study in 2022 discovered that women with dry skin saw improvements in skin hydration, suppleness, and wrinkle formation with an Ecklonia cava (Phaeophyceae) extract high in phlorotannins. Another randomized, double-blind, placebo-controlled study discovered that a phlorotannin-rich Ascophyllum nodosum extract reduced face pigmentation, and enhanced skin suppleness, in women with age spots
[176][177][178,179].
Researchers have looked into the potential for marine-derived compounds from Undaria pinnatifida, Octopus vulgaris, and Sargassum polycystum, to improve skin pigmentation, as well as to possess antioxidant, anti-inflammatory, and immunomodulatory capabilities. These substances (compounds
22–
24 in
Figure 7) also contain octaphlorethol A, fucoidan, and fucoxanthin
[178][179][180][181][182][183][180,181,182,183,184,185]. Numerous studies have looked into how octaphlor-ethol A affects skin conditions and pigmentation. According to one study, in human melanoma cells, octaphlorethol A inhibited the formation of melanin, and decreased skin pigmentation. In a different study, mice with atopic dermatitis showed enhanced skin barrier function and reduced inflammation when treated with octaphlorethol A
[177][184][179,186]. Additionally, a cream containing fucoidan and marine collagen enhanced skin hydration, suppleness, and wrinkle formation in women with dry skin, according to a randomized, double-blind, placebo-controlled research study
[185][187]. Additionally, a cream containing fucoidan and marine collagen enhanced skin hydration, suppleness, and wrinkle formation in women with dry skin, according to a randomized, double-blind, placebo-controlled research study
[186][188]. Fucoxanthin, a carotenoid pigment, was found to be associated with a significant decrease in the severity of melasma in a review of 11 randomized controlled studies. To corroborate these findings, more research is required, as the authors stated that the quality of the inclusive studies was generally low
[187][188][189][189,190,191].
6. Modern Skin Pigmentation Treatments and Promising New Technologies
The preferred method of treatment for problems with skin pigmentation has long been laser therapy. The melanin in the skin can be reduced and evened out by lasering the afflicted area, leading to a more even complexion. As time goes on, technological developments mean that lasers are more and more efficient. Today, pigmentation can be targeted in deeper, more covert locations, thanks to laser technology. For instance, lasers can now be used to target pigment under the skin’s surface, without causing irritation or damage to the skin! As a result, problems such as age spots and sun damage can be treated without any negative consequences or discomfort. To remove obstinate pigmentation, the most recent lasers combine optical energy with intense pulsed light (IPL). This is an exciting development, as it makes it possible to treat patients more quickly and effectively than ever before
[190][191][192][205,206,207].
Topical creams and serums are among the newest and most promising therapies for skin pigmentation. These remedies include substances such as niacinamide, kojic acid, licorice extract, and mulberry extract that are especially made to fight pigmentation. These cutting-edge chemicals have the potential to significantly reduce dark spots, lighten skin tone, and enhance the skin’s overall clarity and texture. For instance, kojic acid can limit tyrosinase activity, which helps to prevent hyperpigmentation from occurring, and niacinamide can suppress melanin formation, which helps to reduce skin discoloration. In order to prevent the skin from experiencing any unpleasant reactions or side effects, the treatment should also be free of parabens and other harmful preservatives
[193][194][195][208,209,210]. In order to diminish pigmentation, micro-needling is a process used to increase the skin’s natural collagen and elastin production. In order to provide a more exact therapy, the technique now involves using specialized instruments. Small needles are used in the procedure, to puncture the skin and create microscopic channels that can only be seen under a microscope. This straightforward procedure enhances collagen synthesis, while promoting the skin’s natural ability to mend itself. Overall, with excellent outcomes, micro-needling is quickly rising to the top of the list of popular methods for lightening skin
[196][197][198][211,212,213]. Typically, chemical peels are used to remove the top layers of skin, which lessens the visibility of dark patches. Combination treatments, however, are far more effective for the skin. Combination therapies are proving to be even more effective at minimizing dark spots. These combination treatments include several acids, such as glycolic acid and lactic acid, which, when used together, can be much more potent than when used separately. These combined therapies, which neither lasers nor light-based devices can currently offer, can help with both facial discoloration, and uneven pigmentation on other parts of the body, with only one treatment
[199][200][214,215].
With the development of new technology, the future of skin pigmentation therapies appears to be more promising than ever. One of the most promising new therapies for diseases of skin pigmentation is plasma pen therapy. Freckles, age spots, sunspots, and melasma can all be treated using this technique, which removes pigment from the skin by means of a targeted plasma energy beam. Compared to previous therapies, this one is less intrusive, and has fewer adverse effects
[201][202][203][216,217,218].
The use of radiofrequency therapies to treat diseases of skin pigmentation is growing in popularity. The appearance of dark areas, and the overall tone and texture of the skin, can be improved by this technology, which uses radio waves to break down melanin deposits in the skin. Radiofrequency treatments are quick, non-invasive, safe, and do not entail a long recovery time
[203][204][218,219].