Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by U UBAIDILLAH and Version 2 by Jessie Wu.
A prosthetic is an artificial device to replace missing or lost limbs; these instances are mainly contributed to amputation.
- prosthetic devices
- metamaterials
- prosthetics
- limb
1. Introduction
Amputation is a surgical process to remove a segment of a body part. Infection, disease (related to the circulatory system), and traumatic events (falling, being crushed or blasted). Different cases of amputation require different types of prosthetic device based on the level of amputation. In general, prosthetics can be classified into upper limb prosthetics and lower limb prosthetics. Upper limb prosthetics are designed to replace bodily parts above the hip (i.e., trans-radial and elbow disarticulation). On the contrary, lower limb prosthetics are designed to replace bodily parts below the hip (i.e., transtibial, transfemoral) [1][2]. In prosthetic development, aesthetics and function are two parameters that cannot be separated. Therefore, the development of prosthetics has been extensively studied to provide a better solution for the amputee. The latest development in the field of prosthetics provides not only a primary function but, to some degree, a return for the amputee to the lifestyle they were used to before amputation [2][3].
Egyptian civilization is known as the first pioneer of developing prosthetic devices, dating from 2750 to 2625 AD. Their prosthetics are mainly made of fibre and used primarily for appearance rather than function; an exception to this is a prosthetic finger found on an Egyptian mummy that is believed to provide a functional and non-functional purpose [3][4]. Another instance in our history regarding the use or development of prosthetics is from the Punic War (218–210 AD), where a Roman soldier used an iron hand to replace his missing arm [4][5]. The year 1871 saw a significant increase in amputation numbers following the conclusion of the American Civil War. James Edward Hanger developed an above-knee prosthetic (patented as a “Hanger limb”) with the implementation of a rubber bumper to replace the standard catgut tendons and designed with a hinge at the knee and ankle [5][6]. Later major wars, such as WW1 and WW2, did not see a significant advancement of prosthetic technology caused by the higher demands for the development of military technology. Later on, to solve this problem, in February 1945, the US National Academy of Sciences (NAS) initiated and planned a research and development (R&D) program aimed at developing prosthetic improvements by applying technology from other specialized fields. This event was soon followed by significant developments such as the first hydraulic knee in 1947, the SACH (solid ankle cushion heel) introduced by Anthony Staros in 1957, a computer-aided robotic arm in 1980, and a motor-powered lower limb prosthetic in 2012 [6][7]. Subsequently, researchers aimed to implement the unique properties of the MR (magnetorheological) effect as a brake for lower limb prosthetics [7][8]; by 2020, Brown et al. had conducted research to improve the comfort of amputees by proposing the use of metamaterials as a liner in the socket for a transtibial prosthetic [8][9]. The diagram within Figure 1 illustrates the development of prosthetics.
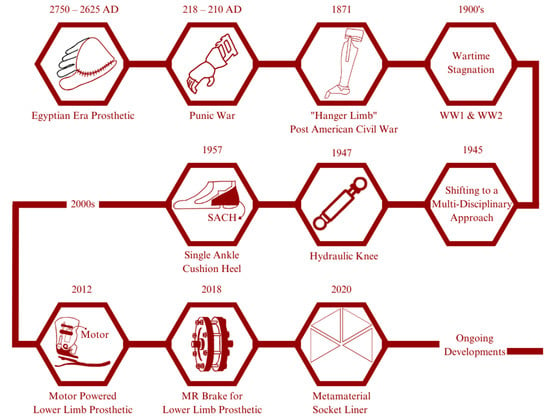
Figure 1. Historical development of prosthetics: In ancient Egypt, wooden prosthetic toes and feet were crafted for amputees. These prosthetics were not functional but were designed to mimic the appearance of a real foot or toe. Similarly, in ancient Greece and Rome, prosthetics were made from wood and bronze and were designed primarily for aesthetic purposes. In recent years, advancements in robotics and computer technology have led to the development of advanced prosthetic limbs that can be controlled using neural signals from the user’s brain. These “bionic” limbs are capable of incredibly life-like movement and have revolutionized the field of prosthetics. The development of prosthetics has been a long and fascinating journey, with significant advancements being made over the centuries. Today, prosthetic technology continues to advance rapidly, offering new hope and possibilities for amputees around the world.
Metamaterial is derived from the Greek word “meta” which means “to be beyond”. Hence, a metamaterial is defined as a unique material with effective properties that are beyond its conventional counterparts. The effective properties of a metamaterial originate from its bulk material properties and structural arrangement or design. These effective properties are varied based on the class of the metamaterial and its purpose. Mechanical, acoustic [9][10], electromagnetic [10][11], optical [11][12][12,13], and thermal [13][14] metamaterials are the five general classes of metamaterial. Mechanical metamaterials, also known as auxetic metamaterials, are metamaterials exhibiting the unique property of a negative Poisson’s ratio (NPR) or the ability to laterally enlarge when longitudinally stretched. Lakes first studied this unique property in 1987 [14][15], which was then coined as “auxetic” to shorten the term “having a negative Poisson’s ratio” by Evans et al. [15][16]. The word auxetic is also derived from the Greek meaning “growing” or “having the tendency to grow.” Since then, the concept of auxetic metamaterial has been extensively researched and is increasing even now.
Early on, the research was mostly focused on developing a better structural arrangement and analysing its properties (i.e., Poisson’s ratio, effective modulus, stiffness, and energy absorption). In terms of its structural arrangement, unique geometries are based on a re-entrant hexagon [16][17], double-V [17][18], double-U [18][19], chiral [19][20], and even major changes to the already established re-entrant hexagon by adding an additional horizontal component between the vertical parts [20][21]. Lately, the focus of research in the field of auxetics has gradually shifted to a more practical approach. These research works include an auxetic nail [21][22], an anti-blast and anti-impact protection [22][23], an auxetic stent for circulatory disease [23][24], an auxetic implant [24][25], and an improvement in foot prosthetic performance [25][26].
2. Regarding Prosthetics
As mentioned in the Introduction earlier, a prosthetic is an artificial device to replace missing or lost limbs [26][102]. These instances are mainly attributed to amputation. Amputation is a process of disarticulating limbs or body parts. Common causes for amputations are diabetes, cancer, traumatic events, hypertension, hyperlipidaemia, and in rare cases include congenital limb deficiencies [27][103]. Diabetes is a disease caused by a drastic elevation in the blood sugar level in the circulation system. This condition often leads to damage to blood vessels and nerves and impairs the circulatory system. An impaired circulatory system prevents the body from properly circulating blood. An improper circulatory system is particularly dangerous. Should the patient experience a traumatic experience that could lead to an injury, wound, or broken certain body parts, it cannot heal properly. Improperly healed wounds or injuries require immediate treatment as the wound can be a starting point of infection which could quickly spread to other body parts. In order to prevent the spread of infection, disarticulating infected body parts (amputation) is required [28][104].
Traumatic amputation is an immediate disarticulation of body parts resulting from an accident or injury. Replantation is a surgical procedure to reattach or replant already disarticulated limbs or body parts. There are some factors that need to be taken into consideration to choose between replantation and amputation, this consideration and factors are listed in Figure 2 [29][30][31][32][33][105,106,107,108,109].
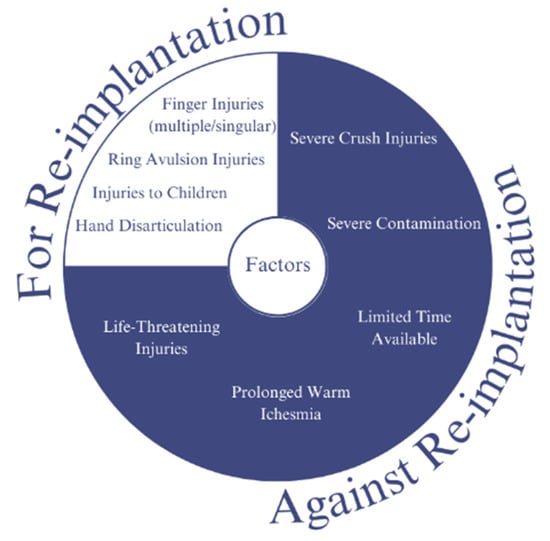
Figure 2. Consideration of replantation for post-traumatic disarticulation: Replantation is a surgical procedure that involves reattaching a body part, such as a finger or limb, that has been completely severed from the body. Post-traumatic disarticulation refers to the loss of a limb or body part as a result of a traumatic injury. In cases where replantation is not possible or not recommended, other treatment options, such as prosthetics or physical therapy, may be considered to help patients regain function and improve their quality of life. Ultimately, the decision to pursue replantation must be made on a case-by-case basis, with careful consideration of the patient’s individual circumstances and needs.
Amputation level is closely related to the classification of prosthetic devices. Generally, prosthetic devices are classified into two main categories which are lower-extremity and upper-extremity prosthetics. Figure 3 illustrates the classification of prosthetic devices based on the level of amputation [34][110].
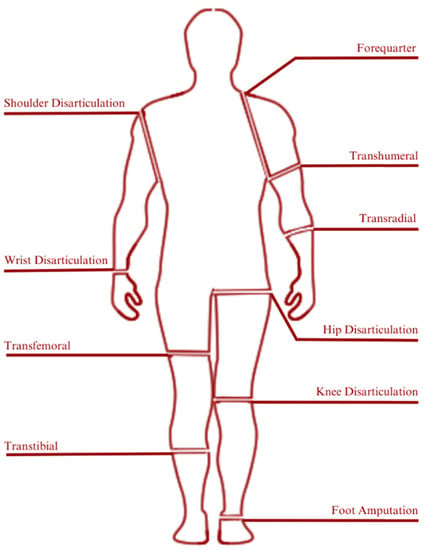
Figure 3. Prosthetic classification based on amputation/disarticulation levels: Prosthetics are artificial devices that replace missing body parts or limbs. Prosthetic limbs are designed to compensate for the loss of a limb, and the type of prosthetic required often depends on the level of amputation or disarticulation. The level of amputation or disarticulation determines the type of prosthetic limb that is required, and the prosthetic must be carefully fitted and adjusted to the individual’s needs to ensure the best possible function and comfort. Of the existing prosthetic classifications, transtibial is under discussion in this resviearchw. The transtibial prosthetic has several parts. Of the several existing parts, metamaterials are used in the development of prosthetic technology. These include parts of the sole, socket, foot, and suspension parts.
The ratio of lower limb amputation compared with upper limb amputation could reach a ratio of 11:1 [35][111]. A transtibial prosthetic is divided into an interface, suspension, shank, joint, and foot part. To better visualize the composition of transtibial prosthetics, refer to Figure 4[26][102].
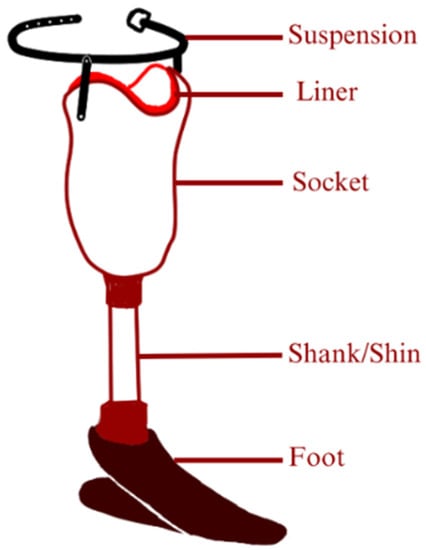
Figure 4. Composition of transtibial prosthetic: It is possible to develop the components of a transtibial prosthetic using auxetic metamaterials, but it would depend on the specific application and requirements of the prosthetic. Auxetic materials are unique in that they have a negative Poisson’s ratio, meaning that they expand in all directions when stretched. This property can be advantageous for certain applications, such as providing better shock absorption or improving energy return. For example, auxetic materials have been studied for use in prosthetic sockets to provide improved comfort and stability for amputees. The unique expansion properties of the auxetic material can help distribute pressure more evenly over the residual limb, reducing discomfort and the risk of injury. However, it is important to note that the design and development of prosthetic components using auxetic metamaterials is still a relatively new area of research, and there are many factors to consider when selecting materials and designing components for prosthetics. These include factors such as strength, durability, weight, and cost, among others.
An interface is a part of the prosthetic having the role of connecting the residual limb to the prosthetic. An interface must be able to provide fitting, cushion, and shock absorption. The interface part is divided based on the material into hard material (such as wood), and soft material (such as closed-cell foam). Materials such as wood are used early on thanks to their simple manufacturing methods and abundant, easy-to-find materials. In terms of maintenance, this type of interface material is relatively easy to maintain thanks to its high durability. Despite its ease of production, this type of interface material comes with inherent disadvantages, mainly its lack of cushioning. This disadvantage is the reason for later consideration of a soft material interface. Common materials used for soft interface materials include closed-cell foam. This material is used because of its waterproof properties, accompanied by its malleability which makes it a material that is easy to mould based on user characteristics [36][112]. Suspension refers to the part which holds the prosthetic in place when worn. A good suspension should be able to provide zero relative movements against the residual limb. A badly fitted suspension would cause a condition known as “pistoning”. Pistoning can and does cause pain, skin breakdown, irritation, and non-responsive prosthetic movement.
The choice of the best type of suspension (waist belt, joint and corset, and sleeve) and interface parts for a transtibial prosthetic is different from person to person. Essentially, other than to replace a missing ambulatory capability, a prosthetic is also aimed at the comfort of its user. This means that the best choice lies in what makes the user most comfortable. Whichever type of interface is chosen, there has to be an accurate impression technique to support it. Such impression techniques consist of hand casting, pressure casting, and optical scanning. Apart from the impression, another aspect of fitting a prosthetic involves the act of alignment. The bench alignment method is one of the most common methods of alignment, although there exists a more advanced and accurate alignment technology known as electronic alignment. This method requires the use of sensors fitted into the prosthetic to provide data in terms of user gait behaviour when wearing the prosthetic. This method is capable of providing data that are unavailable from bench alignment, such as the socket load over a period of time walking.