Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Sonia Morè and Version 2 by Lindsay Dong.
Belantamab Mafodotin, a first-in-class anti-B cell maturation antigen (BCMA) antibody–drug conjugate, demonstrated good efficacy and safety profile in triple-refractory patients in the phase 2 DREAMM-2 trial, and it was approved for the treatment of MM triple-exposed patients with >4 prior lines of therapy.
- multiple myeloma
- belantamab mafodotin
- antibody–drug conjugate
1. Introduction
Multiple myeloma (MM) is the second most common hematological disease accounting for approximately 10% of all hematological malignancies, and its typically an elderly hematologic disease, with the median age of patients at the diagnosis of about 65 years [1].
MM is characterized by abnormal plasma cell proliferation in the bone marrow, which produces an excess of monoclonal protein (M-protein) detected in blood and urine. This M-protein causes specific organ damage resulting in MM signs and symptoms, typically hypercalcemia, renal insufficiency, anemia and osteolytic bone lesions [2].
The therapeutical landscape of effective anti-myeloma drugs has widely expanded in the last decade thanks to the introduction of proteasome inhibitors (PIs, such as bortezomib, carfilzomib and ixazomib), immunomodulatory drugs (IMiDs, such as thalidomide, lenalidomide and pomalidomide) and, recently, monoclonal antibodies (mAbs), such as elotuzumab, daratumumab and isatuximab [2]. The introduction of these agents has translated into prolonged progression-free survival (PFS) as well as overall survival (OS) with significantly fewer toxicities and improved quality of life. Currently, thanks to the therapeutic first-line approaches, including quadruplet induction combination, high-dose chemotherapy, followed by autologous hematopoietic stem-cells transplantation (ASCT), and consolidation–maintenance, the 10-year OS probability is about 60% in patients eligible for ASCT. [3]. In non-transplant eligible (NTE) patients, therapeutical first-line approaches based on doublet or triplet combination with PIs, IMiDs and mAbs result in a prolonged OS, with a median OS of 5 years.
However, MM still remains largely an incurable disease with poor outcomes, especially among patients who become resistant to therapies [4].
Immunotherapeutic approaches, both passive, for example, mAbs and cellular products targeting clonal plasma cells, or active (when a patient’s immune system is stimulated to induce an immune response against plasma cells), have been investigated to harness the patients’ immune system to destroy clonal plasma cells and, nowadays, represent an effective strategy for the treatment of MM [2].
Clonal plasma cells express several antigens on their surface, with the most important molecule under investigation as potential targets for mAbs, such as CD38, CD40, CD138, CD56, CD54, PD1, kappa light chain, B-cell maturation antigen (BCMA) and the signaling lymphocyte activation molecule F7 (SLAMF7). To date, novel immunotherapies, including antibody–drug conjugates (ADC), bispecific antibodies and chimeric antigen receptor T-cell (CAR-T), represent an important option for relapsed or refractory disease resulting in high-quality, deep and durable responses [5].
More recently, based on the results of the pivotal phase III MAIA trial, daratumumab was approved, in combination with Rd, in newly diagnosed MM not eligible for ASCT [6][16]. Another daratumumab-based combination therapy has been recently approved, D-VMP, for newly diagnosed MM patients not eligible for ASCT [7][17].
Isatuximab, an IgG-k chimeric monoclonal antibody targeting a specific epitope on CD38, was investigated in combination with other drugs in relapsed/refractory settings. Based on the efficacy results, in terms of ORR and PFS, of the phase III ICARIA study, the combination of isatuximab plus Pd was approved for RRMM patients who have received at least two prior lines of therapy, including lenalidomide [8][19].
Selinexor, melfulflen, cerebron E3 ligase modulators (CELMoDs) and venetoclax represent very promising drugs for RRMM patients’ treatment.
The first-in-class oral selective inhibitor of nuclear export targeting exportin-1, selinexor, received FDA approval in combination with bortezomib and dexamethasone (SVd) for RRMM patients after the first line of therapy [9][23]. The median PFS for patients treated with SVd was 13.9 months compared to 9.5 months for patients treated with Vd. In addition, selinexor was approved in combination with dexamethasone for triple refractory patients [10][24]. Melfuflen (melfuflen-flufenamide) is the first-in-class peptide-drug conjugate targeting aminopeptidases and releasing alkylating agents into clonal plasma cells [11][25]. The phase II HORIZON trial demonstrated melfuflen efficacy in association with dexamethasone, with a median PFS of 4.2 months in a very heavily pretreated population [12][26].
Frequent, deep, and durable responses to BCMA-directed CAR-T cells (idecabtagene–vicleucel) have been recently reported in MM patients who were triple-class exposed and refractory to their last regimen in the multicenter pivotal phase II KarMMa-2 trial [13][29]. This has led to the rapid approval by FDA and by EMA of the first product (idecabtagene–vicleucel) for RR MM patients after three lines of therapy. On February 2022, FDA approved a second product, ciltacabtagene–autoleucel, for the treatment of RR MM patients after four or more lines of therapy, based on the results of the phase 1b/2 study CARTITUDE-1 [14][30].
2. Belantamab Mafodotin
Belantamab Mafodotin is the first-in-class ADC targeting BCMA that obtained FDA accelerated approval in August 2020, based on the results of phase II DREAMM-2 trial, for patients with RRMM who have received at least four prior lines of therapy, including a proteasome inhibitor, an immunomodulatory agent and an anti-CD38 monoclonal antibody [15][32]. On November 2022, FDA announced that the process for the withdrawal of the US marketing authorization for belantamab mafodotin had been initiated. This action is based on the results of the DREAMM-3 trial (NCT04162210), in which the primary endpoint of PFS was not met, with a hazard ratio of 1.03 (95% confidence interval, 0.72–1.47) in a head-to-head comparison of belantamab mafodotin versus Pd.2.1. Mechanism of Action
ADCs, an evolution of naked mAbs, consist of a mAb attached to a specific cytotoxic payload covalently conjugated through chemical linkers. The mechanism of action of ADCs is unique, whereby the mAb binds a tumor-specific antigen on clonal plasma cells resulting in cytotoxic payload internalization. Once the ADCs are intracellular, lysosomal degradation occurs, causing the release of the toxic payload within the plasma cells. Then, the free toxic payload enters the cytoplasm and/or nucleus, exerting its effect and causing apoptosis and cell death [16][33]. BCMA is a member of the TNF receptor superfamily and can be an optimal target for ADCs in MM due to its high expression on clonal plasma cells. Indeed, it is a cell-surface receptor protein expressed almost in end-stage B lymphocytes and clonal plasma cells. Because of its unique expression on MM cells, BCMA has become of interest to developing specifically targeted immunotherapies for MM. During the malignant transformation of immature plasma cells, the BCMA receptor and its ligand, named a proliferation-inducing ligand (APRIL) and B-cell activating factor (BAFF), overexpression activate several signal transduction pathways involved in oncogenesis, including nuclear factor kappa-light-chain-enhancer of activated B cells (NF-kB), protein kinase B (AKT), signal transducer and activator of transcription 3 (STAT3), phosphoinositide 3-kinase (PI3K) and mitogen-activated protein kinases (MAPK) cascades. The most common naked mAbs used in MM treatment are humanized antibodies or fully human immunoglobulin G subtype thanks to its long-circulating half-life in the bloodstream and lower immunogenicity. For ADCs, the choice of the ideal antibody is important. However, for the choice of ideal ADCs, it is important, beyond the antibody structure, the covalent linker because, as mentioned, linkers play a crucial role in releasing the potent drug at target tumor cells. Indeed, it has to be able to avoid premature degradation in the plasma because it can cause the release of cytotoxic payload with off-target effects on healthy cells. But, at the same time, it has to be able to degrade the cytotoxic component in the pathologic cells once the ADC can be internalized in the malignant target cell [16][33]. ADCs linkers are classified according to different categories in terms of the mechanism of drug release and their stability in circulation, including cleavable linkers and non-cleavable linkers. Cleavable linkers are designed to respond to a specific physiological environment, such as there being high glutathione concentrations, low pH, and special protease, which could assist the linkers in enabling chemical or biochemical reactions by way of hydrolyzation or proteolysis. The second group is non-cleavable linkers that rely on the monoclonal antibody degradation after ADCs’ internalization within the lysosomes and endosomes to generate the metabolites containing the active cytotoxic drugs with or without a portion of the linkers [17][35]. Belantamab mafodotin, also called belamaf (GSK2587916), is the first-in-class humanized IgG1 ADC that targets BCMA, approved for RRMM patients after four prior lines of therapy. This ADC is composed of an antibody that is able to bind BCMA, conjugated to a cytotoxic agent, monometil auristatin F (mafodotin), by a protease-resistant maleimidocaproyl linker. After binding BCMA on target cells, Belamaf is internalized and undergoes a process of proteolytic cleavage, releasing mafodotin. The released mafodotin disrupts the microtubular cell network leading to cell cycle arrest and apoptosis [15][32] (Figure 1).Figure 1. Mechanism of action of belantamab mafodotin. After binding to BCMA on plasmacell, ADC is degraded in the lysosome with release of MMAF that leads to G2/M arrest and caspase 3 dependent apoptosis. Belamaf exerts antibody-dependent cell-mediated cytotoxicity (ADCC) and antibody-dependent cellular phagocytosis (ADCP).
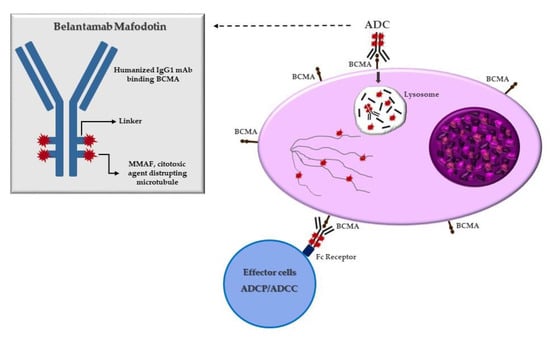
Belantamab mafodotin, also called belamaf (GSK2587916), is the first-in-class humanized IgG1 ADC that targets BCMA, approved for RRMM patients after four prior lines of therapy. This ADC is composed of an antibody that is able to bind BCMA, conjugated to a cytotoxic agent, monometil auristatin F (mafodotin), by a protease-resistant maleimidocaproyl linker. After binding BCMA on target cells, Belamaf is internalized and undergoes a process of proteolytic cleavage, releasing mafodotin. The released mafodotin disrupts the microtubular cell network leading to cell cycle arrest and apoptosis [15][32] (Figure 1).
Figure 1. Mechanism of action of belantamab mafodotin. After binding to BCMA on plasmacell, ADC is degraded in the lysosome with release of MMAF that leads to G2/M arrest and caspase 3 dependent apoptosis. Belamaf exerts antibody-dependent cell-mediated cytotoxicity (ADCC) and antibody-dependent cellular phagocytosis (ADCP).