2. The Past and Present of SGCs
2.1. The General Histopathological Prognostic Factors for SGCs
2.1.1. The Histological Types
Histological diagnosis reflects biological behavior in several cases. The current WHO classification (5th edition) describes the grading system for MEC, AdCC, salivary carcinoma, and NOS
[4][1]. Other tumors that show similar classification include carcinoma ex pleomorphic adenoma (CXPA) and intraductal carcinoma (IDC). The WHO classification detaches grades from tumor names since tumors with the same features of a cancer type do not necessarily have the same severity or aggressiveness, allowing for flexibility in describing tumors
[1][4][5][1,2,5] (Bishop, J.A. et al. pp. 31–51). Each tumor’s histological features are subsequently discussed.
2.1.2. High-Grade Transformation (Dedifferentiation)
Dedifferentiation is a regression from a more differentiated to a less differentiated state (stem-cell-like). In particular, in a malignant tumor, a differentiated cell loses its specific form or function
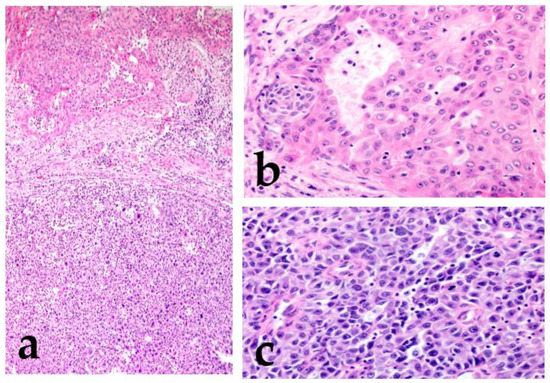
[6][7][6,7]. Histopathologically, dedifferentiation is observed as the abrupt transformation of a well-differentiated tumor into high-grade morphology (poorly differentiated or anaplastic/undifferentiated), lacking the original morphology (
Figure 1)
[8].
Figure 1. Mucoepidermoid carcinoma (MEC) with high-grade transformation. There is intermediate-grade MEC in the upper region, and the lower region shows high-grade transformation (a). Intermediate-grade MEC forms glandular or solid structures and consists mainly of intermediate cells with moderate atypia (increased nuclear size with an obvious nucleus) (b). The high-grade region shows undifferentiated features, and the cells lack the original morphology (c).
In the high-grade region, the tumor cells show anaplastic cells with large vesicular pleomorphic nuclei, prominent nucleoli, an increased mitoses/Ki67 labeling index, and necrosis
[8][9][8,9]. The term “dedifferentiation” is occasionally used in malignant soft tissue tumors, such as dedifferentiated liposarcoma or dedifferentiated chondrosarcoma
[10][11][10,11]. However, in SGCs, a malignant tumor is rarely replaced by a completely different histological morphology, and the original morphological features usually remain. Therefore, the term high-grade transformation is used to describe this phenomenon
[8][12][8,12]. This transformation is reported not only in variable low-grade malignant tumors (acinic cell carcinoma, MEC, secretory carcinoma, hyalinizing clear cell carcinoma, myoepithelial carcinoma, epithelial–myoepithelial carcinoma, and polymorphous adenocarcinoma) but also in high-grade tumors, including AdCC
[12][13][14][15][16][17][18][19][20][21][12,13,14,15,16,17,18,19,20,21]. Tumors with this finding have an even worse prognosis.
2.1.3. Micropapillary Pattern
Invasive micropapillary carcinoma (IMPC) was first reported in the breast
[22]. Neoplastic cell nests are uniformly distributed throughout a reticulated interstitium and exhibit a reverse polarity or “inside-out” growth pattern. This histological finding is observed in other malignant tumors of the urinary bladder, lung, stomach, colon, and bile duct
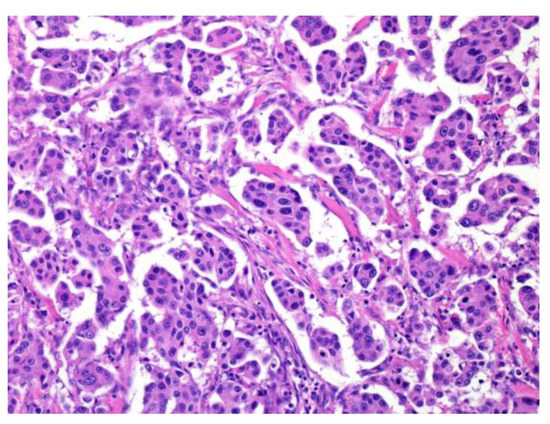
[23][24][25][26][27][23,24,25,26,27]. IMPC, a tumor with a micropapillary pattern, frequently shows lymphatic invasion and lymph node metastasis, and its prognosis is very poor. Among SGCs, micropapillary salivary duct carcinoma (SDC) is the most prevalent; nonetheless, micropapillary AdCC and intraductal papillary mucinous neoplasm (IPMN) have also been reported (
Figure 2)
[21][28][29][21,28,29].
Figure 2. Micropapillary salivary duct carcinoma (SDC). The tumor forms many micropapillary nests that consist of eosinophilic cytoplasm and irregular nuclear-like SDC.
2.1.4. Other Histologic Findings
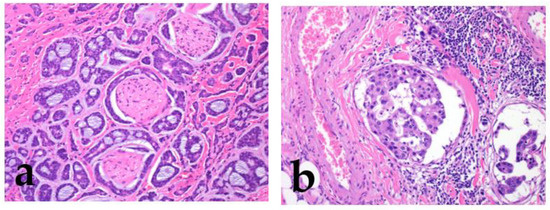
Strong prognostic factors prevalent in many tumors include increased cellular atypia, perineural invasion, lymphovascular invasion, an increased mitoses/Ki67 labeling index, necrosis, local recurrence/distant metastasis, and poor surgical margin (
Figure 3)
[1][2][3][5][2,3,4,5] (Bishop, J.A. et al. pp. 31–51).
Figure 3. Perineural invasion and lymphatic invasion. Adenoid cystic carcinoma shows frequent perineural invasion (a), and salivary duct carcinoma shows lymphatic invasion (b).
For lymph node metastasis, important prognostic factors include the number of nodes, foci size, unilateral/bilateral involvement, extranodal extension, and stromal reaction
[30][31][32][30,31,32]. Lombardi reported that intraparotid node metastasis implies an increased risk of lateral neck involvement and impact on the survival of patients with SGCs
[33]. More specifically, the overall number (0 vs. 1–3 vs. ≥4) and diameter (<20 mm vs. ≥20 mm) of the node metastasis represent major prognostic factors for overall survival
[33]. Additionally, for parotid gland carcinoma, facial nerve paralysis and tumor adhesion/immobility could be the predictive factors for high-grade SGCs
[34].
2.2. Other Related Factors
Although not directly involved histopathologically, the most predictive factors for tumor recurrence are advanced age, male sex, large tumor size, and high clinical stage
[1][35][36][37][2,35,36,37] (Bishop, J.A. et al. pp. 31–51). Concerning the site of tumor origin, small salivary glands have a high frequency of SGC occurrence, and the sublingual salivary gland has the highest frequency of malignancy
[1][38][2,38] (Bishop, J.A. et al. pp. 31–51).
3. Validated Grading Systems for Individual SGCs and Similar Diseases
3.1. Grading System in the WHO Classification
3.1.1. Mucoepidermoid Carcinoma (MEC)
MEC is characterized by mucous, as
rwe
searchers intermediate and epidermoid/squamoid tumor cells. However, in some tumors, intermediate cells are predominant. MEC forms cystic and solid growth patterns that are usually associated with
MAML2 rearrangement
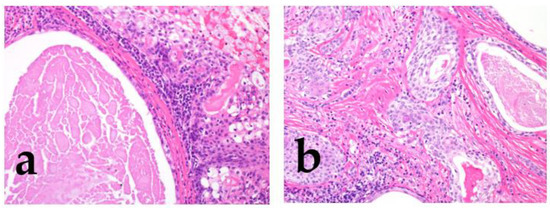
[1][39][2,39] (Bishop, J.A. et al. pp. 265–290); therefore, some reports describe the histological features for grading (
Figure 4)
[1][39][40][41][42][43][2,39,40,41,42,43], which include structural atypia (cystic/solid component, border invasion pattern, lymphovascular/perineural invasion, and necrosis) and cytological atypia (nuclear anaplasia/pleomorphism and mitoses)
[1][36][37][38][39][40][41][42][43][2,36,37,38,39,40,41,42,43]. According to these gradings, MEC should be graded as low, intermediate, or high. The higher the grade, the greater the possibility of metastasis or recurrence
[1][39][2,39] (Bishop, J.A. et al. pp. 265–290).
Figure 4. The morphological features of low/intermediate mucoepidermoid carcinoma (MEC). The tumor forms cystic (a; low grade) and solid growth patterns (b; intermediate). In both cases, tumor cell atypia is mild, but the intermediate category shows slightly different nuclear sizes with mitosis.
The Armed Forces Institute of Pathology (AFIP) grading system was previously used; however, this system may not necessarily indicate the actual degree of some aggressive cases
[1][40][2,40] (Bishop, J.A. et al. pp. 265–290); hence, the Brandwein system was introduced to classify these cases from the viewpoint of anaplasia
[42]. Nevertheless, high-grade MEC is very rare, and there is no difference in outcome between low and intermediate grades using any grading system. Another study reported that mitosis and necrosis may be helpful in the classification of tumor grade
[43].
3.1.2. Adenoid Cystic Carcinoma (AdCC)
AdCC consists of two main cell types: ductal cells located in the inner part and myoepithelial cells located in the outer part of the duct. The ductal cells have eosinophilic cytoplasm and uniformly round nuclei, while the myoepithelial cells have a clear cytoplasm and hyperchromatic angular nuclei
[1][44][2,44] (Bishop, J.A. et al. pp. 337–356). Perineural invasion is an AdCC hallmark, and genetically, it is characterized by
MYB or related gene translocations. Typically, AdCC comprises pseudocysts and true glandular lumina. AdCC shows three growth patterns: tubular, cribriform, and solid
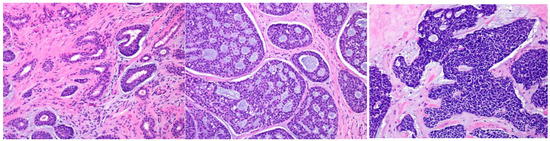
[1][44][2,44] (Bishop, J.A. et al. pp. 337–356). Consequently, the following histological grading is used for its classification: tubular predominant as grade Ⅰ, cribriform predominant as grade Ⅱ, and solid predominant as grade Ⅲ (
Figure 5)
[1][44][45][2,44,45].
Figure 5.
The histological grade of adenoid cystic carcinoma (AdCC). The tumor shows tubular (
left
), cribriform (
middle
), and solid (
right
) growth patterns.
Although AdCCs with >30% solid components have been shown to be more aggressive, any solid tumor component may be a high-grade tumor, as described in the minAmax system
[46][47][48][46,47,48]. Necrosis, marked pleomorphism, or high levels of mitoses are only seen in the solid pattern and are not utilized in the grading system
[1][2] (pp. 337–356).
3.1.3. Salivary Carcinoma, NOS (Adenocarcinoma, Not Otherwise Specified (NOS), Formerly)
In the current WHO classification (5th edition), adenocarcinoma, NOS, is renamed as salivary carcinoma, NOS, and
reswe
archers have used the same term herein
[49]. It includes the subtypes of oncocytic and intestinal-type adenocarcinoma. The term salivary carcinoma, NOS, should be used for tumors arising in major/minor salivary glands; however, this category is a heterogeneous spectrum of carcinomas showing ductal and/or glandular differentiation. It represents an exclusive diagnosis of otherwise defined salivary gland carcinoma entities (adenocarcinoma with nonspecific appearance)
[1][49][50][2,49,50]. Due to differences in this carcinoma’s interpretation, the percentage or case numbers have varied in previous reports, and the pure entity adenocarcinoma, NOS, now accounts for approximately 10% of SGCs
[36][51][52][53][54][55][36,51,52,53,54,55]. Adenocarcinoma, NOS, was considered a heterogeneous group of tumors; however, the strictly selected cases were considered as the pure group
[56]. The histological grading system was based on a previous report published in 1982 by Spiro et al., and the tumors were classified as low-, intermediate-, or high-grade
[1][49][54][55][2,49,54,55] (Bishop, J.A. et al. pp. 290–303). They defined anaplastic or high-grade lesions as grade Ⅲ, which are arranged in close clumps and broad bands composed of small glandular tumor cells. The tumor cell nests are separated by collagen connective tissue stroma, similar to that in seen during scirrhous formation. In addition, they are divided into low- (grade Ⅰ) or intermediate-grade (grade II); the low-grade variant shows no stromal invasion, whereas the intermediate grade shows definite stromal infiltration. Grade Ⅱ lesions have prominent sheets or cords of some polymorphic glandular cells with a pale cytoplasm
[54]. Although this classification reflected the tumor prognosis at that time, it is still somewhat reasonably useful today; however, it should be revised owing to the differences in current diagnostic criteria.
3.2. Carcinoma ex Pleomorphic Adenoma (CXPA)
CXPA is an epithelial and/or myoepithelial malignancy arising in a primary or recurrent pleomorphic adenoma (PA)
[1][57][2,57] (Bishop, J.A. et al. pp. 374–400). Reflecting the presence of PA, the typical clinical presentation is a long-term painless mass with recent rapid progression or previous PA diagnosis. PA presents as ductal and myoepithelial cells arranged in bilayered tubular structures, while the stroma is typically mucoid, myxoid, hyalinized, or chondroid. Usually, the transition from PA to the malignant component is distinct; however, some cases may have heavy stromal/hyalinized collagen bundles or chondroid/myxoid stroma only. The common malignancies are SDC, epithelial–myoepithelial carcinoma, salivary carcinoma, NOS, and myoepithelial carcinoma; in contrast, carcinosarcoma is rare
[58]. Most carcinosarcomas arise from PA through the intraductal or myoepithelial pathway, the multistep adenoma–carcinoma–sarcoma sequence
[59]. The relevant observations are the histological subtype/grade, the proportion of carcinoma (>50%), and the extent of invasion
[1][58][59][60][2,58,59,60] (Bishop, J.A. et al. pp. 374–400). The malignant component progresses from an encapsulated neoplasm to extracapsular invasion. The term “encapsulated” has been rephrased by various alternatives, such as “intracapsular”, “in situ”, “preinvasive”, “intramural”, or “noninvasive”; however, the term intracapsular is preferred. CXPA is subclassified based on the extent of invasion beyond the PA as follows: intracapsular, minimally invasive (the carcinoma invades <4–6 mm beyond the PA borders), and invasive (invasion beyond the PA capsule ≥6 mm)
[57]. However, evaluating the fibrous capsule is occasionally challenging because the tumor forms the capsule or the capsule outline is vague, especially in primary minor salivary glands. Several specimen preparations are needed for a precise diagnosis.
3.3. Intraductal Carcinoma (IDC)
IDC is a salivary gland malignancy located entirely or predominantly intraductally
[1][61][2,61] (Bishop, J.A. et al. pp. 461–475). It has papillary, cribriform, and solid structures mimicking atypical ductal hyperplasia or ductal carcinoma in situ of the breast
[1][61][2,61] (Bishop, J.A. et al. pp. 461–475). It shows four subtypes based on the tumor cells: intercalated duct, apocrine, oncocytic, and mixed IDC; hence, tumors in this category are heterogeneous. Usually, intercalated duct and oncocytic IDC are low-grade, whereas apocrine and mixed IDC are low- or high-grade
[1][61][2,61] (Bishop, J.A. et al. pp. 461–475). Independent of tumor cell subtype, pure IDC behaves indolently, although invasive carcinomas ex-IDC (arising from IDC) can behave aggressively
[62][63][62,63]. Therefore, these tumors may be reassessed as “IDC, noninvasive (low-grade IDC)”, “IDC, noninvasive (high-grade IDC)”, or “IDC, invasive”, similar to intraductal papillary mucinous neoplasm (IPMN) of the pancreas or CXPA of the salivary gland.