Magnesium (Mg2+) is one of the most important ions in health and is the second most abundant cation in the cell with a concentration estimated between 10 and 30 mM. Due to its importance, Mg2+, requires a specific transport system. In Mammals, several transporters have been identified (TRPM6/7, CNNM1/2/3/4, MAGT1, SLC41A1, MRS2). There is numerous evidence suggesting an association between Mg2+ intake and digestive cancer risk and/or development.
- magnesium transporters
- digestive cancers
1. Magnesium
Magnesium (Mg2+) is one of the most important ions in health and is the second most abundant cation in the cell with a concentration estimated between 10 and 30 mM. Due to the binding to different partners like ATP, ribosomes, or nucleotides, the free intracellular Mg2+ levels lower to 0.5 to 1.2 mM [1][11]. Mg2+ is essential in almost all cellular processes, acting as a cofactor and activator for various enzymes [1][11]. For example, Mg2+ is essential in DNA stabilization, DNA repair mechanisms, or even protein synthesis [2][3][4][5][12,13,14,15]. New interactions are still being discovered, expanding the importance of this cation [6][16].
Normal Mg2+ in blood serum levels for healthy people is about 0.7–1 mM, corresponding to an average daily intake (ADI) of 320–420 mg/day [7][8][17,18]. This Mg2+ intake is absorbed mostly in the small intestine by two mechanisms: paracellular transport and via the expression of membrane transporters (Figure 1). Paracellular transport is predominant, mainly because of low expression of claudins in the small intestine [9][10][19,20]. Numerous Mg2+ transporters are also present in the plasma membrane of intestine cells for Mg2+ absorption. An average of 100 mg is absorbed in the intestine, depending on the daily Mg2+ intake [1][11]. Kidneys filters around 2400 mg of Mg2+ per day in the glomeruli, where most of the Mg2+ (2300 mg) is reabsorbed in the thick ascending limb of Henle’s loop. Mg2+ is mainly stored in bones but also in muscles and soft tissues. [1][11][11,21]. This organization allows the Mg2+ homeostasis balance, maintaining a constant 0.7–1 mM Mg2+ serum level in normal conditions.
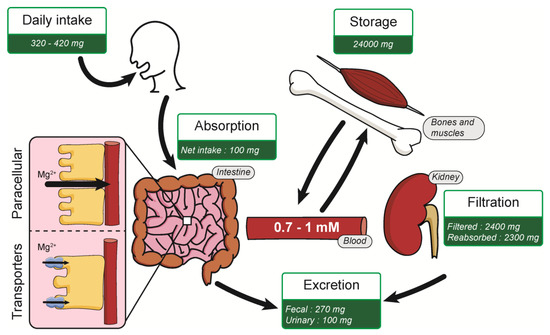
Figure 1. Summary of Mg2+ homeostasis.
Unfortunately, our alimentation contains nowadays less Mg2+ because of the development of the food industry and changes in soils due to intensive farming [12][13][22,23]. Along with the modifications of our eating habits and the prevalence of processed foods, it is shown that a large number of adults do not reach the recommended Mg2+ average daily intake [14][24]. Hypomagnesemia is characterized by Mg2+ serum levels <0.7 mM, but it is often underestimated because the serum levels are not representative of the whole Mg2+ availability [15][25]. Hypomagnesemia is associated with several health issues such as epilepsy, cystic fibrosis, atherosclerosis, and type 2 diabetes [16][17][18][19][26,27,28,29].
Several studies suggest that calcium (Ca2+) and Mg2+ can compete during intestinal absorption, leading to the consideration also of the Ca2+/Mg2+ ratio for assessing Ca2+ and Mg2+ intakes [20][30].
Due to its importance, Mg2+, requires a specific transport system. The first magnesium transporters were identified in prokaryotes, with the identification of the proteins magnesium/cobalt transporter (CorA), magnesium-transporting ATPase (MgtA/B/E) [21][31]. Subsequently, Mg2+ transporters were identified and cloned in other models (Figure 2). In Mammals, several transporters have been identified and will be described in this manuscript.
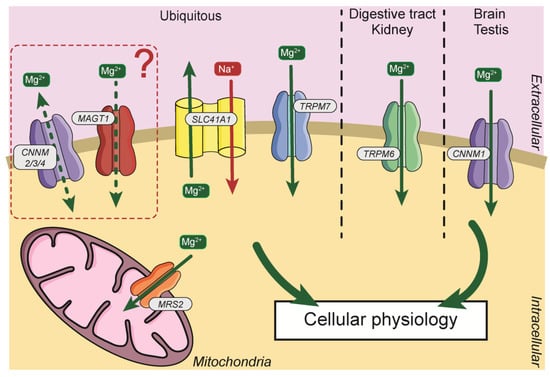
Figure 2. General distribution and localization of Mg2+ transporters in cells. Mg2+, magnesium; Na+, sodium; CNNM2/3/4, Cyclin and CBS Domain Divalent Metal Cation Transport Mediator2/3/4; MAGT1, Magnesium Transporter 1; SLC41A1, Solute Carrier Family 41, Member 1; TRPM7, Transient Receptor Potential Cation Channel Subfamily M Member 7; TRPM6, Transient Receptor Potential Cation Channel Subfamily M Member 6; CNNM1, Cyclin and CBS Domain Divalent Metal Cation Transport Mediator1; MRS2, Mitochondrial RNA Splicing Protein 2.
2. Mg2+ Intake and Digestive Cancers
There is much evidence suggesting an association between Mg2+ intake and digestive cancer risk and/or development. For example, high Mg2+ intake and particularly low Ca2+/Mg2+ ratio protects against reflux esophagitis and Barret’s esophagus, two precursors of ESAC. However, no significant associations were observed between Mg2+ intake and ESAC incidence [60]. However, the association is less evident for GC because there is only a suggestive trend for a preventive effect of high Mg2+ intake in non-cardia GC depending of gender and dietary source of Mg2+ [61].
In PDAC, a first study from 2012 in a large cohort (142,203 men and 334,999 women) recruited between 1992 and 2000 shows no association between Mg2+ intake and cancer risk [22][62]. Another study has investigated the association between nutrients intake from fruit and vegetable and PDAC risk [23][63]. The results show an inverse association between PDAC risk and nutrient intake, including Mg2+, in a dose-dependent manner. Importantly, Dibaba et al. have shown in a large cohort, followed from 2000 to 2008, that every 100 mg per day decrement in Mg2+ intake was associated with a 24% increase in PDAC incidence [24][64]. Moreover, analysis of metallomics in PDAC reveals a lower concentration of Mg2+ in urine of patients with PDAC [25][65].
Mg2+ intake was associated with a lower risk for CRC, particularly in people with low Ca2+/Mg2+ intake ratio [26] [66]. Importantly, Dai et al. also show that the Thr1482Ile polymorphism in the TRPM7 gene increases the risk for adenomatous and hyperplastic polyps [27][66]. It was also shown that Mg2+ intake around 400 mg per day has a protective effect for CRC incidence in postmenopausal women [28][67]. A meta-analysis from 29 studies published on PubMed, Web of Science and the Chinese National Knowledge Infrastructure confirms that the high intake of Mg2+ is inversely associated with the risk of CRC [29][68]. Assessment of Mg2+ concentration in serum showed an inverse association with CRC risk in female but not in male. Moreover, no significant association was detected between dietary Mg2+ and CRC risk in this study [30][69]. Finally, Wesselink et al. suggested that an interaction between normal 25-hydroxyvitamin D3 concentration and high Mg2+ intake is essential for reducing the risk of mortality by CRC [31][70].
To summarize, these epidemiologic studies suggested that high Mg2+ intake by diet and/or supplemental compounds is inversely associated with CRC, PDAC and possibly ESAC risk, but not with GC risk.