Breast cancer (BC) is one of the most common causes of female mortality around the globe. It is the second most common cancer and the fifth leading cause of death from cancer in the world. It accounts for around 25% of all female cancers. The worldwide incidence of BC in 2012 was 1.67 million, which is alarming. The incidence may increase to 3.2 million by 2050. Males may also develop BC, but this is very rare, accounting for <1% of diagnosed BCs worldwide. BC may be of different types, based on various factors including etiology, location, and clinical and molecular characteristics. Based on location, BC may be of two types; namely, non-invasive and invasive. Non-invasive BC does not extend away from the lobules or duct where it is located. Invasive BC, on the other hand, reaches out from the lobules and ducts to the nearby mammary tissue.
1. Overview
Breast cancer (BC) is one of the most common type of cancer and an important contributor to female mortality. Several genes and epigenetic modifications are involved in the development and progression of BC. Research in phytochemistry, nutrigenomics, and nutrigenetics has provided strong evidence that certain phytonutrients are able to modulate gene expression at transcriptional and post-transcriptional levels. Such phytonutrients may also be beneficial to prevent and treat BC. In this review, we will focus on the nutrigenomic effects of various phytochemicals including polyphenols, phytosterols, terpenoids, alkaloids, and other compounds from different sources. Overall, these phytonutrients are found to inhibit BC cell proliferation, differentiation, invasion, metastasis, angiogenesis, and induce apoptotic cell death by targeting various molecular pathways. They also alter epigenetic mechanisms and enhance the chemosensitivity and radiosensitivity of cancer cells. Such phytochemicals may be used for the effective management of BC patients in the clinical setting in the future. The present article aims to summarize the specific molecular pathways involved in the genetic effects of phytochemicals in BC.
2. Phytochemicals
Breast cancer (BC) is one of the most common causes of female mortality around the globe. It is the second most common cancer and the fifth leading cause of death from cancer in the world
[1]. It accounts for around 25% of all female cancers
[2]. The worldwide incidence of BC in 2012 was 1.67 million, which is alarming
[3]. The incidence may increase to 3.2 million by 2050
[4][5]. Males may also develop BC, but this is very rare, accounting for <1% of diagnosed BCs worldwide
[6]. BC may be of different types, based on various factors including etiology, location, and clinical and molecular characteristics. Based on location, BC may be of two types; namely, non-invasive and invasive
[7]. Non-invasive BC does not extend away from the lobules or duct where it is located. Invasive BC, on the other hand, reaches out from the lobules and ducts to the nearby mammary tissue
[7].
BC may be further classified based on the expression of estrogen receptors (ER) into two broad groups; namely, ER-positive and ER-negative
[8]. Other molecular characteristics, such as expression of progesterone receptors (PR)
[9] and human epidermal growth factor receptor 2 (HER2),
[10] are also used for categorization of BC. Such hormone receptor positive BCs maybe treated with aromatase inhibitors or hormonal therapy
[11]. BCs that do not exhibit increased expression of any of these three hormone receptors are known as triple negative BCs (TNBCs)
[12]. TNBC does not respond to hormonal therapy.
The common approaches used in the management of BCs include chemotherapy, radiotherapy, and surgical interventions, which often results in significant side effects
[13]. Increase in drug resistance further limits the therapeutic potentials of many of these interventions. Thus, researchers are continuously searching for novel alternative strategies for dealing with such conditions in a more effective way.
Long before the discovery of modern medicine, herbal remedies were used by ancient people for managing a wide range of diseases under traditional medicine systems, such as Chinese medicine, Tibetan medicine, Ayurveda, Siddha, Unani, Roman medicine, Greek medicine, Mesopotamian medicine, Egyptian medicine
[14], etc. Due to their potent biological activities, research on medicinal plants and phytochemistry has gained much importance in recent days. Phytochemicals are unique bioactive organic compounds, which are mostly secondary metabolites obtained from plant sources
[15][16]. Almost all plant sources are rich in such phytochemicals, which are involved in defense systems of plants and help in the interaction with the biotic environment. More than 5000 unique phytochemicals have been isolated from various plant sources including fruits, vegetables, grains, traditional herbs, etc.
[17]. Much more phytochemicals are yet to be discovered.
Many of these phytochemicals are being used as pharmaceuticals, nutraceuticals, coloring agents, flavoring agents, food additives, agrochemicals, cosmetics, etc. These compounds exert their biological effects mainly by modulating certain molecular targets including cellular receptors, neuroreceptors, ion channels, ion pumps, cytoskeleton, transcription machinery, etc.
[18][19]. Such properties maybe useful for preventing and treating various ailments such as cancer
[20][21], diabetes
[22][23], heart disease
[24], neurodegeneration
[25][26], pre- and post-menopausal manifestations
[27][28][29], skin disease and wound healing
[30], etc. Certain phytochemicals are found to exert anti-BC effects by modulating some genes and signal transduction pathways. These phytochemicals inhibit breast carcinoma mostly by reducing cell proliferation, inducing apoptosis, decreasing metastasis, suppressing angiogenesis, and reducing the migratory properties of cancer cells
[31][32]. These compounds are also found to enhance the therapeutic efficiency of other anti-cancer drugs, sensitization to radiation, and prevent drug resistance in cancerous tissue
[31].
As previously mentioned, phytochemicals are proven natural ingredients with the ability to treat/ameliorate various diseases. In the case of BC, it has been reported that, with the strong activity of phytochemicals, the incidence rate and recurrence of BC could be greatly reduced. This article aims to summarize the specific molecular pathways involved in the genetic effects of phytochemicals in BC. On the other hand, phytochemicals reported for the treatment and management of BC require more supportive clinical data for confirmation. The field of natural substances (of vegetal origin) being very diverse implies the need for extensive studies to confirm the action and therapeutic role of phytochemicals; in consequence, another purpose of this research was also to provide valuable data as the most informative and recent background support necessary for the further development of BC research and treatment.
3. Genetics of Breast Cancer
Several genes are found to be involved in BC, which significantly influence their screening and follow-up strategies. Heredity does play an important role in BC, but <30% of patients with a family history of BC have specific predisposing genes
[33]. The majority of hereditary cases (up to 25%) are attributed to the mutations in some specific highly penetrant and rare genes, which confer an 80% life time risk of BC
[33]. Such genes include BC genes A1 (
BRCA1) and A2 (
BRCA2), phosphatase and tensin homolog (
PTEN), tumor protein p53 (
TP53), cadherin-1 (
CDH1), and serine/threonine kinase-11 (
STK11)
[33]. Specific clinical guidelines are available for the management of such patients. Mutations in some moderately penetrant and rare genes such as checkpoint kinase-2 (
CHEK2), BRCA1-interacting protein-1 (
BRIP1), ataxia telangiectasia mutated (
ATM), and partner and localizer of BRCA2 (
PALB2) are also involved in the development of BC in a minority of cases (2 to 3%)
[33]. Such mutations may increase the risk two-fold.
Additionally, mutations in some low-penetrant and common genes may also be involved
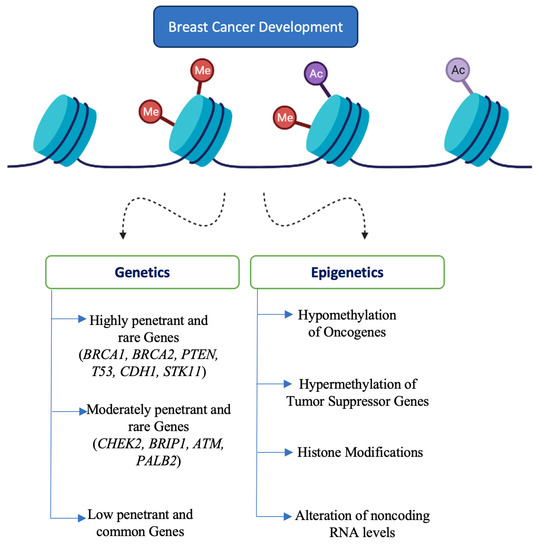
[18]. Identification of such minor genes is not performed routinely in the clinical setting. In addition to genetic factors, epigenetic factors may also influence the development of BC. Certain epigenetic factors, including methylation of tumor suppressor genes, hypomethylation of oncogenes and repetitive DNAs, stabilization of repressive chromosome looping, downregulation of tumor suppressing micro RNAs, upregulation of metastamiRs and oncomiRs, altered histone modifications, etc., may lead to tumorigenesis in BC
[34][35]. Genetic and epigenetic contributors of BC are represented in
Figure 1.
Figure 1. Genetic and epigenetic contributors of breast cancer. Legend: breast cancer gene A (BRCA), phosphatase and tensin homolog (PTEN), tumor protein p53 (TP53), cadherin-1 (CDH1) and serine/threonine kinase-11 (STK11), checkpoint kinase 2 (CHEK2), BRCA1-interacting protein-1 (BRIP1), ataxia telangiectasia mutated (ATM), partner and localizer of BRCA2 (PALB2).
4. Conclusions
Phytochemicals upregulate the expression of tumor suppressors and downregulate the oncogenes. They prevent cell proliferation, differentiation, metastasis, migration, invasion, and angiogenesis, induce apoptosis, and sensitize cancer cells to chemotherapy and radiotherapy. They also cause epigenetic modifications of gene expression by altering DNA methylation, histone acetylation, and non-coding RNA levels. Such effects make them ideal leads for anti-BC drug development.
However, the bioavailability and metabolism of these phytochemicals are not well established. Newer technologies such as nano-encapsulation, nano-emulsion, and other nano-formulation based drug delivery systems may be utilized for targeted delivery of such phytochemicals and increased efficiency. Huge amounts of unique phytochemicals are present in nature and, thus, in silico studies may further accelerate the identification process for drug development. These phytochemicals are also found to enhance the efficacy of conventional therapies. It is thus essential to evaluate the effectiveness of these phytochemicals in combination with various chemotherapeutics. Moreover, the exact molecular pathways and gene expression patterns associated with the beneficial effects of these phytochemicals should be determined by proper preclinical and clinical studies.
 +1 point
+1 point