Osteoarthritis (OA) affects one in three people over the age of 65, and it is more common among women than men. This multifactorial disease leads to structural changes of the joint, and it is connected to chronic conditions. OA is characterized by pain, stiffness, and decreased range of motion (ROM). These factors lead to poor quality of life—insomnia, depression, lack of confidence, and limitations in daily activities, work, or hobbies. OA causes very serious problems for patients and significant social and economic costs.
1. Overview
Worldwide tendencies to perform large numbers of total hip arthroplasties in the treatment of osteoarthritis are observable over a long period of time. Every year, there is an observable increase in the number of these procedures performed. The outcomes are good but not ideal, especially in groups of patients with spine problems. In recent years, a growing interest in this field may be observed, since spinopelvic alignment seems to have a significant impact on total hip replacement (THR) results. The aim of this study is to describe relations between spine and pelvic alignment and provide practical information about its impact on total hip replacement. The authors performed a literature review based on PubMed, Embase, and Medline and provide practical guidelines based on them and their own experience.
2. Osteoarthritis
Osteoarthritis (OA) affects one in three people over the age of 65, and it is more common among women than men. This multifactorial disease leads to structural changes of the joint, and it is connected to chronic conditions. OA is characterized by pain, stiffness, and decreased range of motion (ROM). These factors lead to poor quality of life—insomnia, depression, lack of confidence, and limitations in daily activities, work, or hobbies. OA causes very serious problems for patients and significant social and economic costs
[1].
Total hip replacement (THR) was a revolutionary method used for the treatment of an end-stage osteoarthritis in the hip. The aim of this operation is to increase the patient’s range of motion and activity level, alleviate pain, reduce limitations in everyday life, and, ultimately, improve the patients’ standard of living
[2]. Although the first steps in modern THR date back to the 1940s
[3], this technique is constantly enhanced. It should also be pointed out that indications of THR have changed throughout the years. In the past, this procedure was reserved for infirm, ailing people having major difficulties walking. Nowadays, the range of indications is much wider. Contemporary technologies are able to deliver highly advanced implants to meet even the most demanding requirements and assure patients’ fully functioning life, full of challenging activities
[4]. Our knowledge of total hip replacement, according to the records, is enriched with the classification of architectural hip deformities
[5], perioperative care
[6], and the use of alternative types of articulations, e.g., dual mobility components
[7]. Currently, we can also feature many different bearing types used for THR
[8], which improves patient outcomes after an operation.
Despite great advancements and fantastic results of the majority of operations, approximately 10% of patients are still not satisfied with the effect of THR
[9][10]. Searching for the reasons of discontent, the following problems seem to play a vital role: insufficient restoration of ROM, perceptible distinction between the length of lower extremities
[5], dislocation of prosthesis elements, and need for revision surgery. The key to achieve satisfaction of patients and perform successful THR with positive results is a traditional or digital preoperative strategy, which has been emphasized by many authors throughout the years
[5][11][12][13][14].
During the last few years, there has been a growing interest in parameters called “spinopelvic alignment”. When it comes to preoperative planning before total hip replacement, hip–spine relations seem to play a big role and have been underestimated during recent years. Interest in that relation is growing as it becomes more clear that it has major clinical consequences
[15], especially in the risk of dislocations
[16]. This study is designed to provide practical advice on preoperative planning for total hip replacement.
3. What May Influence the Spinopelvic Alignment?
The hip and spine coexist in a biomechanical chain, and require special coordination between them. The lumbosacral joint connects the pelvis with the spine. On each side of the body, the hip joint and sacroiliac joint form spine–pelvic–hip connections, which are crucial in pelvic motion and maintaining appropriate balance during bipedal locomotion. Every ongoing disease process associated with joints mentioned before restricts mobility, decreases stability, and makes activities of daily life difficult.
With age, and due to other conditions, such as osteoarthritis, osteoporosis, or fractures, spinal curvatures evolve, mostly causing an incorrect spinal position and imbalance. The sagittal imbalance has a connection with disability and pain and occurs as a result of decreased lumbar lordosis, increased thoracic kyphosis, contractures in hips or knees, and changes in pelvic parameters mentioned above. Human organisms adjust to the environment and develop compensatory mechanisms to prevent consequences of disbalance
[17]. Over the course of a lifetime, compensatory mechanisms are exhausted, which causes pelvic retroversion—the pelvis becomes more horizontal, thinner, and wider. Cervical lordosis, lumbar lordosis, and thoracic kyphosis may become shallower or deeper. Most frequently, lumbar hypolordosis, resulting in hip extension, knee flexion, and ankle flexion
[18][19], thoracic hyperkyphosis, and anterior spinal instability occur. This results in inevitable pathologies involving the axial skeleton, hip joints, knee joints, and ankles.
The interaction of the spine with the lower limbs occurs through the pelvis. The mobility of the pelvis acts as a “hinge” between the spine and the hip—it allows one to move upright on the lower limbs
[20].
Medical procedures performed on patients should also be taken into account. It was demonstrated that spinal fusion before THR might increase the risk of dislocation and impingement by increasing posterior pelvic tilt
[1]. Nevertheless, the more segments are involved, the higher the limitations and the more dysfunctional the hip–spine biomechanics are
[1][2].
4. Problems Associated with Improper Spinopelvic Mobility and THR
Dislocation of a hip prosthesis is a common complication occurring after the THR. The rate varies from 0.2 to 10% per year
[21]. Even in 1980, there were reports of the impact of neuromuscular and cognitive disorders or excessive intake of alcohol beverages on the prevalence of single or recurrent dislocation
[22]. Dislocations have a range of other risk factors, such as older age
[23], gender, comorbidities such as rheumatoid arthritis (RA)
[24], or surgical approach
[25]. Another very important role in dislocations after THR is cup and stem position. The reports indicate a correlation between prevalence of posterior dislocation and low cup anteversion
[23]. The size of the femoral head articulation is also instrumental in decreasing the risk of dislocation. Larger, 36 mm femoral heads, compared with smaller, 28 mm articulations, lower the incidence of displacement during the first year after primary THR
[26].
The “safe zone” (anteversion 15° ± 10°, inclination 40° ± 10° of acetabular cup), defined by Lewinnek, was designed to decrease the risk of dislocation after primary THR
[16]. However, dislocations still occur
[27]. One of the main reasons for that is probably the spine dynamics. Patients with a sagittal spinal deformity (SSD) are not protected by the “safe zone”
[28]. SSD means abnormal kyphosis or lordosis, which can result in abnormalities within the pelvis
[29].
Since spine dynamics are not the only risk factor, surgeons must be aware of the other ones. Unfortunately, almost all of them cannot be fixed by preoperative planning and special positioning of implants. That is why the surgeon should pay special attention to spine dynamics—one of the most important factors, and one of very few amenable to change by the orthopedic surgeon.
5. Anatomy and Imaging
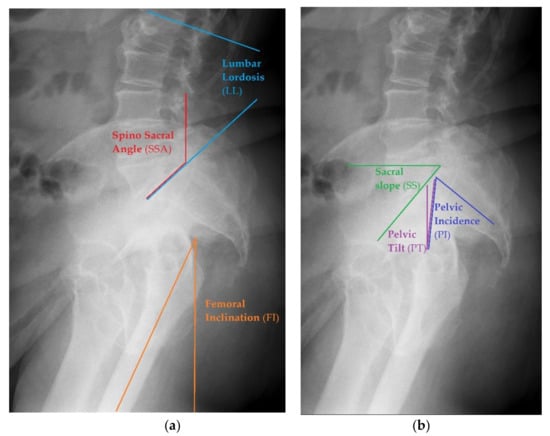
Before starting the operation, proper planning should be done. Normally, the whole process is done based on antero-posterior pelvic X-ray. In case of any suspicion of abnormalities with spinopelvic alignment, special lateral views could also be useful, as they allow one to perform measurements of more sophisticated parameters of pelvic alignment. This should visualize a part of the body from L1 to the proximal femur, including the pelvis. Example of such X-rays are seen in Figure 1.
Figure 1. Examples of different pelvic measurements performed on lateral X-rays of the pelvis with lumbar spine view. (a) Spino Sacral Angle, Lumbar Lordosis and femoral Inclination presented on lateral X-ray. (b) Sacral Slope, Pelvic Incidence and Pelvic Tilt presented on lateral X-ray.
Radiographic Measurements
-
Sacral Slope (SS)—to measure this angle, one needs to draw the straight line of the S1 superior endplate and a leveled line at a right angle to the gravitational force direction (horizontal reference line)
[30]. The normal value ranges between 32 and 49°
[31].
-
Pelvic Tilt (PT)—an angle between the reference vertical line and the line joining the middle of S1 upper endplate and the center of the femoral head. The normal value ranges from 7 to 19°
[31].
-
Pelvic Incidence (PI)— the angle between the line that is formed by connecting the upper endplate of S1 (at its midpoint) to the femoral head axis. The normal value ranges from 38 to 56°
[31].
-
Pelvic Femoral Angle (PFA)—the position of the femur in relation to the pelvis. It is the angle centered at the femoral head, between the mid sacral base and down femoral shaft. The normal value ranges from 1 to 17°
[31].
-
Lumbar Lordosis (LL)—the segmental angle of spinal segment in lordosis, measured between the line on the upper endplate of L1 and the line on the upper endplate of S1(L1 -L5). The normal value ranges from 40 to 58°
[31].
-
Femoral Inclination (FI)—the angle between a vertical reference line and the axis of the femur. The normal value ranges from 0 to 8°
[31].
-
Sacro Femoral Angle (SFA)—the angle between the line of the upper endplate of S1 and the axis of the femur. The normal value ranges from 43 to 61°
[31]
-
Spino Sacral Angle (SSA)—the angle between the line of the upper endplate of S1 and a reference vertical line. The normal value ranges from 119 to 133°
[31].
All angles mentioned above refer to an X-ray in standing position, which is the most common way to take radiographs for preoperative planning. It is also advisable to take the radiographs in sitting upright position to view the changing relations between the angles. It should be taken into account that the position of the torso during sitting may influence spinopelvic alignment and have an impact on the hip joint
[32].
 +1 point
+1 point