1000/1000
Hot
Most Recent
 +1 point
+1 point
Bile salt hydrolase (BSH; EC 3.5.1.24) is an enzyme produced by the intestinal microbiota that catalyzes the hydrolysis of amide bonds in conjugated BAs, resulting in the release of free amino acids. These enzymes belong to the N-terminal nucleophilic (Ntn) hydrolase superfamily and share a similar αββα-core structure to an N-terminal catalytic cysteine residue. This residue is critical to the catalysis mechanism and acts both as a nucleophile and a proton donor. The N-terminal amino group serves as the proton acceptor and activates the nucleophilic thiol group of the cysteine side chain. Besides the cysteine residue, other amino acids conserved in most BSHs are also relevant to the catalytic reaction, including Arg18, Asp21, Asn82, Asn175, and Arg228.
The gastrointestinal tract hosts a large and complex community of microorganisms, collectively known as the gut microbiota. This community consists of around 1014 microorganisms and is dominated by the presence of about 500–1000 different bacterial species [1][2]. The gut microbiota lives in a close relationship with the host and is crucial for many physiological processes [3][4]. Several mechanisms have been proposed to mediate the effects of these microorganisms on metabolic health. One important function carried out by the human gut microbiota is the deconjugation of primary bile acids (BAs) by BSH enzymes and their impact on host health [5][6]. The presence of active BSHs has long been recognized as a selection criterion for defining potential probiotics. BAs are amphipathic molecules that are initially produced by the host and subsequently transformed by the gut microbiota. Host primary BAs (CA, cholic acid; CDCA, chenodeoxycholic acid) are synthesized from cholesterol and conjugated with glycine or taurine in the liver (GCA and GCDCA, glycocholic acid and glycochenodeoxycholic acid; TCA and TCDCA, taurocholic acid and taurochenodeoxycholic acid). Conjugation improves the solubility of such hydrophobic BAs and reduces the potential damage of the cell membranes. Conjugated BAs are then excreted into the duodenum from the biliary duct, where they contribute to the solubilization of dietary lipids and their absorption through the small intestine and colon [7][8]. Around 95% of BAs are reabsorbed in the distal ileum. They are further effluxed into portal circulation, redirected, and stored in the liver through the enterohepatic cycle (EHC). The remaining primary BAs that escape EHC undergo further microbial biotransformations, including deconjugation, oxidation, epimerization, 7-dehydroxylation, esterification, and desulfatation by the gut microbiota [9]. The prominent secondary BAs are comprised of deoxycholic acid (DCA) and lithocholic acid (LCA), which result from the dehydroxylation of CA and CDCA, respectively [10][11]. Both primary and secondary BAs serve as signaling molecules that influence several processes, including lipid, glucose, and energy metabolism as well as inflammation [12][13].
Recently, increasing attention has been paid to better explore (i) the variety of enzymes catalyzing BA biotransformation, (ii) their distribution, and (iii) their relevance to the host’s health and to disease [14][15][16][17][18][19].
Many reports described that most studied BSHs are encoded by lactic acid bacteria and are used as probiotics to prevent mainly metabolic disorders in humans [20][21][22]. Recently, it was demonstrated that the human gut microbiota plays key a role in contributing to host health [23]. Among these microbial functions, the deconjugation of BAs by BSH enzymes comprises an imperative gateway reaction in the metabolism of BAs [6]. Considering the importance of BAs as biomolecules, gaps in our knowledge of these enzymes need to be filled. To uncover BSH gene abundance and their activity distribution in the gut microbiota, different approaches such as biochemical assays and metagenomic analysis are currently used; however, both approaches have inherent limitations. Indeed, standard biochemical assays that measure substrate consumption or product generation are unsuitable for defining and characterizing BSH enzymatic activities from complex biological samples. Through functional and comparative metagenomic analysis, Jones et al. highlighted the presence of BSH activity in all major bacterial divisions and the enrichment of BSHs in the human gut metagenomes of healthy subjects. Indeed, most metagenomic BSH-active clones were found to belong to Firmicutes, Bacteroidetes, and Actinobacteria [24]. Recently, taxonomic analyses among 11 different worldwide healthy populations have revealed 591 BSH enzymes, which are distributed over 117 genera and 447 bacterial strains [25]. The majority of the identified BSHs in the study belong to five genera, namely Bacteroides, Blautia, Eubacterium, Clostridium, and Roseburia. Around 27% of BSH-encoding bacteria behave as paralogs and are mainly assigned to Bacteroides. Given that the presence of paralogs introduces significant BSH sequence dissimilarity, Song et al. proposed an eight phylotype classification based on a phylogenetic tree as a more rational alternative than the classification by genera. A multivariable regression analysis showed that the relative abundance of BSHs does not significantly correlate with gender, age, and body mass index (BMI), while BSH distribution varies among populations from different geographical regions. At the biochemical level, enzyme activity assays highlighted different deconjugation selectivity between the phylotypes, in agreement with previous reports [25][26]. For example, while the T0 (Clostridium, Intestinibacter, Lactobacillus, Enterococcus), T1 (Eubacterium, Blautia, Clostridium, Roseburia, Ruminococcus), T3 (Lactobacillus), T4 (Bifidobacterium and Collinsella), and T7 (mainly Blautia) groups have significant specific activity for most bile salts, the T5 and T6 groups (assigned to Bacteroides) exhibit lower specificity towards GCA and both GCA/TCA, respectively. In contrast, the T1, T3, and T4 groups display the highest specific activities with GCA. When GCDCA and TCDCA are used as substrates, the highest specific activity is observed for group T2. Using a chemoproteomic approach to target BSH activities in the gut, Parasar et al. (2019) showed that this activity increases during intestinal inflammation, which results in higher deconjugated BAs [27]. Further studies are required to understand the relevance of gut BSH activities in host diseases.
Several studies have investigated BSH-active bacteria for their clinical efficacy in lowering hypercholesterolemia [15][28][29]. These bacteria have been shown to increase BA deconjugation, which in turn decreases cholesterol absorption by enterocytes and enhances its fecal excretion [14]. Increased BSH activity was suggested to affect bile acid composition and to influence farnesoid X receptor (FXR) signaling. It has been demonstrated that reduced FXR activity promotes the downregulation of the small heterodimer partner (SHP) and increases the synthesis of BAs from cholesterol through the rate-limiting enzyme cholesterol 7α-hydroxylase (CYP7A1) [30] (Figure 1). The downregulation of the SHP elicits the activation of the liver X receptor (LXR), which in turn upregulates the adenosine triphosphate-binding cassette transporters G5 and G8 (ABCG5/G8) and promotes cholesterol transport into the bile [31][32] (Figure 1). The effect of BSH activity may be extended to weight gain through FXR signaling and the membrane receptor TGR-5. Previous studies demonstrated that the use of Tempol, an anti-oxidant, prevents obesity in mice through the reduction of BSH activity, resulting in FXR inhibition via the accumulation of tauro-β-muricholic acid. Furthermore, high-fat diet-fed FXR null mice showed reduced diet-induced obesity [12][33]. On the other hand, the activation of TGR-5 by BAs induced a significant weight reduction in mice on a high-fat diet. [34]. Obesity may also be associated with several liver-related diseases, including steatosis, hepatic cancer, and non-alcoholic fatty liver disease (NAFLD), which are linked to altered gut microbiota communities. NAFLD is a chronic liver disease with inflammation, hepatocyte injury, steatosis, and fibrosis as pathological features. Strategies for NAFLD treatment target the gut microbiota based on its ability to modulate insulin sensitivity and metabolism related to host energy, choline, and BAs. Of note, a clinical trial showed that VSL#3, a combination of eight probiotics, improves NAFLD through the increase in glucagon-like peptide-1 (GLP-1) [35]. Other probiotics, tested either in combination or isolated, also showed beneficial effects on NAFLD improvement [36][37]. Recently, Huang et al. demonstrated that Lactobacillus plantarum AR113 and L. casei pWQH0, which both display high BSH activity, decrease hepatic lipid accumulation in NAFLD cell models, which is potentially mediated by the BSH activity [38]. Besides cholesterol and lipid metabolism, BSH activity may be linked to inflammatory disorders. Gut metagenomic analysis revealed a reduced abundance in the BSH gene in patients suffering from inflammatory bowel diseases (IBD) and type 2 diabetes [39][40]. In the IBD context, the induced modification of the BA profile was suggested to alter the protective effect on the intestinal barrier mediated by FXR [40]. Repression of secondary BA metabolism via the modulation of BSH activity may represent a new therapeutic method for hepatic cancer treatment. In fact, primary BAs have been shown to stimulate the liver’s accumulation of hepatic NKT cells and antitumor immunity, thus inhibiting tumorigenesis in a mice model [41]. Besides host–microbiome crosstalk, BSHs are suggested to protect commensal bacteria from BA toxicity and to contribute to bacterial survival and gut colonization [42][43][44]. They are also believed to confer a nutritional advantage since released amino acids might be used as sources of nitrogen, carbon, and energy [14]. Altogether, these data stress the importance of BSH activity and BA receptors as therapeutic targets in numerous diseases.
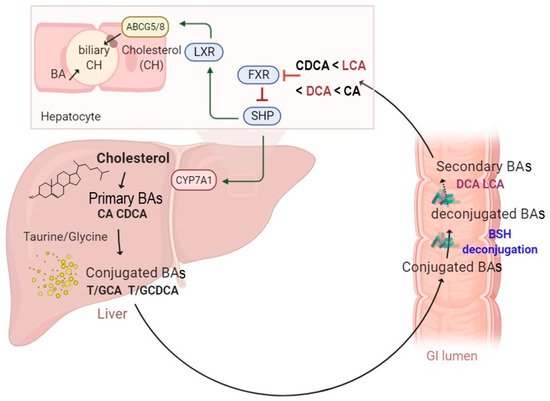
Figure 1. A schematic illustration of enterohepatic circulation and intestinal BA metabolism by BSH enzymes. The BAs are synthesized and conjugated with either taurine or glycine in the liver. They are further spilled over from the enterohepatic circulation and deconjugated by BSH-active gut bacteria. The hydrolysis of the conjugated BAs to deconjugated BAs and subsequent production of the secondary BAs can modulate several functions, including farnesoid X receptor (FXR), small heterodimer partner (SHP), cholesterol 7 alpha-hydroxylase (CYP7A1), liver X receptor (LXR), and ATP-binding cassette transporters G5/G8 heterodimer (ABCG5/8), which transports cholesterol into the bile canaliculi.
This global overview leads us to focus on the analysis of the relevant roles of BSHs on human health and their potential as therapeutic alternatives to treat human diseases.
Hypercholesterolemia is reflected by high plasma levels of both the total and LDL-cholesterol (LDL-c), while the HDL-cholesterol (HDL-c) levels decrease. High cholesterol levels are a major risk factor in the development of atherosclerosis and cardiovascular disease (CVD), the leading cause of mortality in the world [45]. Nowadays, BSH-active bacteria represent the main candidate for the prevention of hypercholesterolemia [14][46][47][48]. Several studies aiming to characterize the BSH encoding members of the gut microbiota were reported [24][26][49]. Not surprisingly, numerous potential probiotics with high BSH activity significantly reduce circulating cholesterol levels. This includes specific Lactobacillus and bifidobacterial species such as B. longum, L. salivarius, L. plantarum, and L. reuteri [16][28][47][50]. Interestingly, Sridevi et al. (2009) demonstrated that the oral administration of immobilized BSH from Lactobacillus buchneri significantly reduced both triglycerides and serum cholesterol using a rodent model of hypercholesterolemia [51]. Using a placebo-controlled, randomized study, Ooi et al. (2010) reported that the administration of a symbiotic capsule containing a BSH-active strain of L. gasseri with inulin resulted in significant reductions in total cholesterol and LDL-c compared to the placebo group [29]. Similar results were obtained with the L. reuteri strains. The effect of yogurts containing microencapsulated L. reuteri NCIMB 30242 was evaluated using a randomized, double-blinded study on hypercholesterolemic subjects. BSH-positive Lactobacillus reuteri NCIMB 30242 consumption over 6 and 9 weeks in [15][52], respectively, resulted in higher plasma deconjugated bile acid levels but lower total cholesterol, LDL-c, and non-HDL-c compared to the placebo group. Of note, Lactobacillus reuteri NCIMB30242 was the first strain of probiotics to be marketed (Cardioviva®) for cholesterol-reducing purposes based on BSH and the bile salt deconjugation mechanism. In another clinical trial, the consumption of yogurt containing L. reuteri CRL 1098 significantly decreased the total circulating cholesterol and LDL-c as well, while levels of HDL and triglycerides were unchanged [53]. Overall, these studies show that microbial BSH activity is able to impact lipid metabolism and reduce hypercholesterolemia. Most Lactobacillus species described as having a hypocholesterolemic effect in human trials have been patented [54][55][56][57]. The obtained hypocholesterolemic effects rely on the ability of BSH activity to deconjugate the primary intestinal BAs, thereby reducing cholesterol reabsorption [58].
In addition to cholesterol-lowering, accumulating research has been conducted to establish potential interplay between weight gain and/or obesity and gut microbiota-encoded BSHs through FXR signaling. Indeed, increasing evidence demonstrates that the microbiota, BAs, and FXR signaling are mandatory to induce obesity [12][59]. Additionally, the gut microbiota analysis of antibiotic-treated children revealed a correlation between body weight gain and prolonged reduction in overall BSH gene abundance [60]. In line with these findings, numerous BSH-expressing probiotics were shown to protect mice from weight gain and obesity as well as to influence the BA pool by modulating FXR signaling [61][62]. Advanced clinical studies showed that fecal microbiota transplantation in obese subjects did not reduce BMI but resulted in a BA profile similar to that of the donor [63][64]. Overall, these data support the hypothesis that targeted BSH enzymes can be delivered in order to control host lipidemia and to protect against weight gain. These effects may be particularly relevant seeing as some Lactobacillus and Bifidobacterium strains exhibiting BSH activity are regularly used in dairy products. In recognition of the importance of ensuring the host’s safety, these strains are commonly subjected to extensive characterization [65]. Furthermore, new therapeutic directions are focused on semi-synthetic FXR agonists, derived from the CDCA molecule [66]. Owing to the emergence of new BSH active probiotics, these strains can be tested to generate deconjugated BAs as FXR agonists.
On the other hand, previous reports have suggested potential adverse effects of increased BSH activity in the intestine. High BSH activity is believed to generate significant amounts of unconjugated BAs, which may result in lipid malabsorption and trigger steatorrhea [67]. Increased BSH activity may also compromise lipid metabolism and colonic mucosal functions, thereby contributing to gallstone formation and colon cancer [68][69].
Giardia duodenalis (also named G. lamblia or G. intestinalis) is a protozoan parasite that infects humans and many animals through oro-fecal transmission [70][71][72]. G. duodenalis is widely distributed in the environment as a resistant cystic form; once ingested, these cysts differentiate into trophozoite (a flagelled replicative form) by excystation in the correct GI tract conditions [73]. The resulting enteropathogen can reach the colon and can cause giardiasis, one of the most common intestinal infectious diseases worldwide [74][75]. Considered a public health concern, several anti-infectious molecules have been developed to treat giardiasis [72]. However, the emergence of drug resistant strains limits the efficacy of the available treatments [72]. Recent reports established a strong interaction between G. duodenalis and the gut microbiota. In fact, it was highlighted that giardiasis susceptibility is highly influenced by the composition of the gut microbiota [76][77][78]. In turn, G. duodenalis colonization leads to gut microbiota composition changes [77]. Intriguingly, Riba et al. (2020) reported that Giardia infection alters the enteric microbiota composition in neonatal mice and modulates BAs and lipid metabolism, leading to reduced body weight gain and growth, as noted in infected infants [79]. Previous studies investigated the effect of probiotic bacteria (L. johnsonii La1, L. gasseri CNCM I-4884) in the field of giardiasis [80][81][82]. Both strains promote immune response, protect against Giardia-mediated tissue injury, and prevent trophozoite proliferation in murin models [80][82]. Of note, L. gasseri is more effective in vivo than L. jonshoni since L. gasseri reduces the cystic pool of the parasite [80]. Other lactobacillus strains, including L. casei MTCC 1423 and L. rhamnosus, have been tested in a murine model, showed similar protective effects, and reduced the severity/duration of giardiasis [83][84][85]. Interestingly, Shukla et al. (2020) reported an anti-giardia effect and enhanced mucosal immunity by the probiotic protein from L. rhamnosus as well as the heat-killed strain [86]. Although the underlying mechanism remains poorly understood [87][88][89], recent reports demonstrate a potential association between BSH activity and the protective effect against G. duodenalis infection [90][91]. As BSH activity allows for the conversion of primary BAs into deconjugated bile acids, it was suggested that the subsequent release of secondary BAs has a toxic effect and may alter parasite growth and survival. To address this hypothesis, the direct effects of conjugated and deconjugated BAs on the parasite were tested. Both tauro- and glyco-conjugated BAs were inert and did not inhibit parasite growth, while deconjugated BAs (DC and CDC) were toxic in a dose-dependent manner and exhibited a significant deleterious effect on the parasite [90]. Moreover, the simultaneous incubation of G. duodenalis with unconjugated BAs and BSH from C. perfringens allowed for the conversion of incubated BAs into their conjugated forms and consequently led to a killing effect on the parasite [90]. In addition, engineered E. coli to express BSH from L. johnsonii confirmed that BSH antagonized Giardia proliferation in vitro in a dose dependent manner as well as in vivo [91]. Altogether, these results support the promising prospect of using BSH active probiotics as a new therapeutic strategy to treat/prevent G. dudenalis infection.
Another example of a gastrointestinal infectious disease includes Clostridioides difficile infection (CDI). C. difficile is a spore-forming pathogen that might colonize the gut of patients treated by broad-spectrum antibiotics [92][93]. CDI includes a broad range of disorders ranging from diarrhea to colitis and toxic megacolon [92]. Their incidence, severity, and costs are in continuous increase. In addition, they have evolved as a significant cause of mortality during the past decade [92][94][95]. Upon germination, vegetative cells are generated from spores, and the bacterium produces toxins that result in tissues damage, inflammation, and diarrhea [96][97]. In the GI tract, the germination process is mediated by a host-derived molecule including BA sensing through the bile acid germinant receptor [96][98][99][100]. In fact, TCA, CA, and DCA activate germination, while CDCA acts as a competitive inhibitor [101]. Other studies indicate that DCA is a potent inhibitor of this process, as reported with C. scindens. Upon administration, this strain enhances the resistance to infection in a DCA dependent fashion [102]. Recent reports revealed that severe and relapsing CDI patients display high levels of TCA, followed by a reduced abundance of BSH-producing species [103][104]. However, fecal transplantation is effective in treating these patients and increases their resistance to CDI [103][104][105]. Further analysis demonstrates that, following FMT, key bacterial genera responsible for BSH production are recovered, BSH activity and BSH gene copy numbers are balanced, and secondary BAs are restored [103][104]. Interestingly, unlike patients pre-FMT, the BA profiles, similar to that in patients post-FMT, were able to inhibit spores outgrowth into vegetative forms [106]. In addition, supernatants from either engineered E. coli expressing highly active BSH or naturally BSH-producing organisms (Bacteroides ovatus, Collinsella aerofaciens, Bacteroides vulgatus, and Blautia obeum) effectively reduced TCA-mediated C. difficile germination. These effects were also confirmed in a recurrent CDI mouse model, using the recombinant E. coli strain for BSH [103]. These distinctive features pave the way towards the potential use of BSH active probiotics to treat CDI. However, active research must be conducted in this field to unravel the molecular mechanism of how secondary BAs may inhibit C. difficile outgrowth, colonization, and the subsequent inhibition of infection.
Several reports highlighted the association of many human disorders to BA dysregulation. In this context, we recently demonstrated the impact of the gut microbiota, cholesterol, and BA metabolism in hypercholesterolemia and cardiovascular diseases [107]. Furthermore, IBD, including ulcerative colitis and Crohn’s disease, are chronic immune-mediated inflammatory diseases that affect the gastrointestinal system. Targeted drugs are directed at the overactive immune response in these diseases [108]. Interestingly, several reports have suggested BA dysmetabolism as a contributing factor in IBD and irritable bowel syndrome (IBS) pathogenesis [109][110][111][112]. Among the potential mechanisms, the modification of the gut microbiota composition may lead to altered BA transformations in the gut and modulation of the circulating BAs. Direct enzyme activity assays in IBD patients revealed impaired deconjugation, dehydroxylation and, desulfation [113]. Otherwise, cholestasic diseases are also linked to changes in Bas, which are characterized by accumulated BAs levels in the biliary system. This dysfunction causes liver inflammation and injury [114].
Recently, the effect of ursodeoxycholic acid (UDCA) was studied in the context of the intrahepatic cholestasis of pregnancy (ICP) [115]. The reported results demonstrated that this BA counterbalances higher levels of BAs [115][116]. A recent study examined the clinical responses of the efficacy of the biotherapeutical agent UDCA in the case of the ICP cohort [115]. In this work, the authors were interested in the reaction mechanism associated with the effectiveness of UDCA, which counterbalances higher levels of BAs [115]. Such beneficial effects of UDCA were mediated by the gut microbiota through the enrichment of the BSH-expressing bacteria belonging to the Bacteroidetes phylum.
Modification of the BA metabolism is also linked to other human diseases such as liver disorders, including the primary sclerosing cholangitis (PSC). In this context, the gut microbiota and bile acid composition were analyzed in a mice model and demonstrated that the illness severity was increased in germ-free mice [117]. Moreover, Tabibian et al. (2016) described that PSC is reduced by the addition of UDCA, highlighting the protective potential of the gut microbiota and BA against PSC [117].





