RBM-007 is an anti-FGF2 aptamer composed of 37 nucleotides, whose ribose 2′ positions are modified to resist ribonucleases, in addition to being 5′-PEGylated and 3′-conjugated with an inverted dT to confer an advantageous pharmacokinetic profile. RBM-007 binds strongly and specifically to FGF2 and does not cross-react with other FGF family proteins or heparin-binding proteins, blocking the interaction between human FGF2 and its receptors FGFR1 through FGFR4. The dissociation constant (KD) of the non-PEGylated form of RBM-007 to human FGF2 protein is 2 pM, compared to 5, 7, and 27 pM in rat, mouse, and rabbit protein, respectively, showing the high affinity of RBM-007 for different FGF2s regardless of the species difference.
1. Introduction
In mammals, fibroblast growth factors (FGF) have 22 known members that exert important functions in regulating cell proliferation, differentiation, and migration
[1][2]. Upon binding to tyrosine kinase FGF receptors FGFR1–FGFR4, FGFs activate essential signaling pathways, such as the mitogen-activated protein kinase (MAPK)/ERK and JNK pathways, that are centrally involved in angiogenesis, tissue remodeling, and regeneration, including the repair of neuronal damage, skin wound healing, joint protection, and the control of hypertension. Among the FGFs, human FGF2 is an 18-kDa non-glycosylated polypeptide composed of 146 amino acids
[3].
FGF2 generally plays a positive role in bone health; however, several in vitro studies have demonstrated the adverse role of FGF2 in the progression of bone disease
[4][5][6][7]. Recent advances in understanding the role of FGF2 in bone formation alternatively posit that the pharmaceutical manipulation of FGF2 signaling may be a promising approach for bone disease therapy. In the literature, a number of anti-FGF2 neutralizing monoclonal antibodies (mAbs) have been reported
[8][9][10][11][12], while no anti-FGF2 mAbs have been investigated for the clinical potency.
Focusing on the therapeutic potential in inhibiting FGF2, we developed the inhibitory RNA aptamer, RBM-007
[13]. In the literature, a few aptamers (DNA & RNA-based) against FGF2 (or bFGF) were described in the 1990s, but there appeared no subsequent studies on these aptamers. Aptamers are single-stranded short oligonucleotides selected in vitro from a large random sequence library, and are applicable to therapies because of several pharmaceutical advantages, such as a medium size between small molecules and antibodies, chemical synthesis, production cost, and low antigenicity
[14]. Aptamers are built on the foundation of targeted molecules using the systematic evolution of ligands by exponential enrichment (SELEX)
[15][16]. The concept relies on the potential of short oligonucleotides to fold, in the presence of a target, unique tertiary structures that bind with high specificity and affinity. We highlight the broad therapeutic potential of RBM-007 and the multifunctionality of FGF2 (
Figure 1) in the treatments of wet AMD, achondroplasia, cancer pain and lung cancer, respectively.
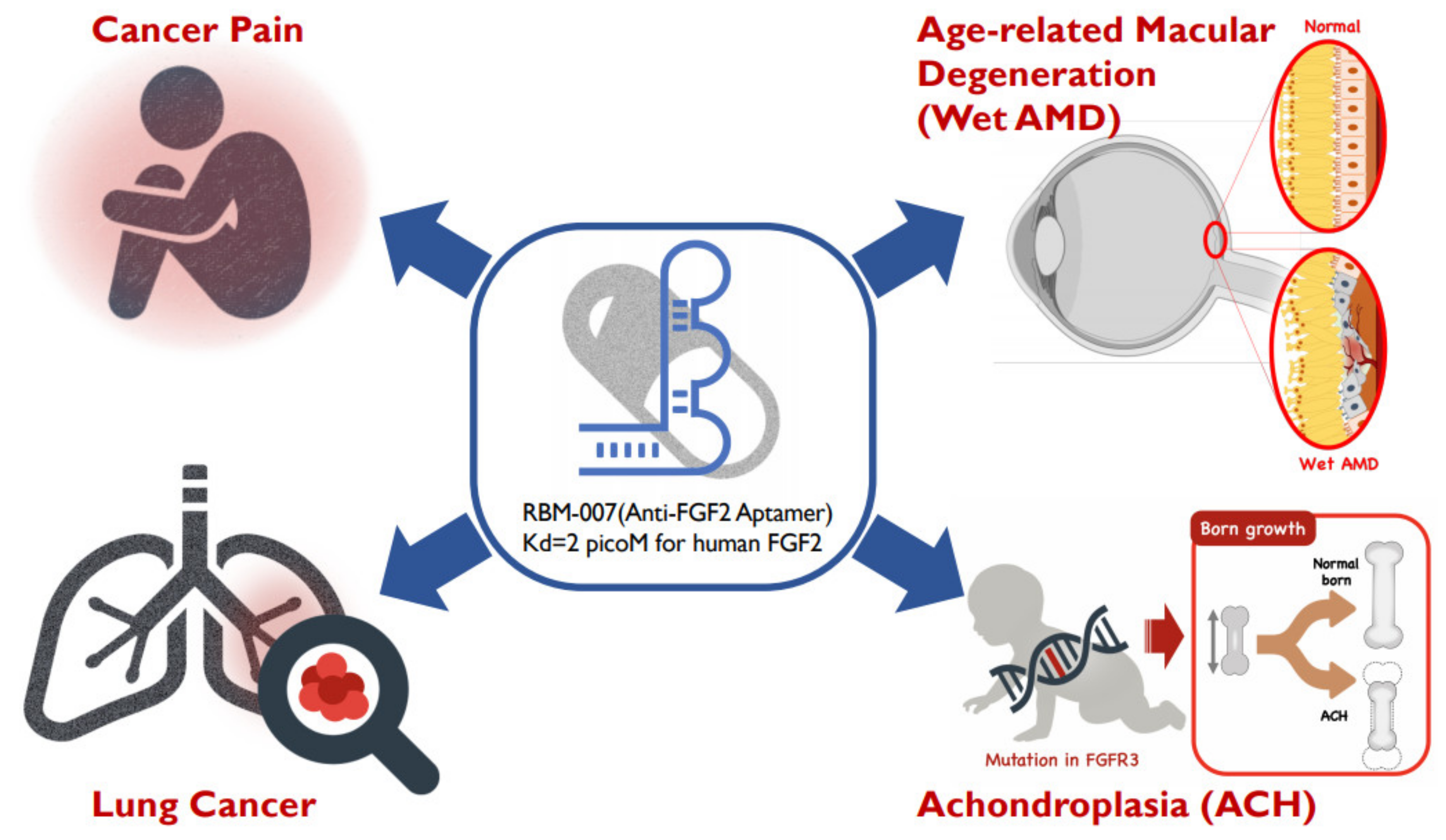 Figure 1.
Figure 1. Diverse therapeutic applications of RBM-007 (anti-FGF2 aptamer).
2. Facts about RBM-007
Aptamers prefer to interact with positively charged surfaces of the target proteins due to the negatively charged nature of backbone linkages. We have shown previously that a 23-nucleotide (nt) RNA aptamer interacting with the Fc domain of human IgG1 (hFc1), which lacks positive charges on the surface, can achieve strong and specific affinity to hFc1 through multiple non-electrostatic forces, such as hydrogen bonds and hydrophobic interactions
[17]. This strong affinity relies on the shape complementarity between aptamers and targets
[18]. Therefore, the aptamer technology is applicable not only for positively charged molecules, but also for relatively neutral molecules.
In our laboratory, we have raised therapeutic RNA aptamers to a variety of human proteins and forwarded some of them to preclinical or clinical studies. Although aptamers share many properties with antibodies, the aptamers exhibited some superior features, such as higher affinity, medium size between small molecules and antibodies, chemical synthesis, production cost, and low antigenicity. This review summarized the properties of one such aptamer, RBM-007, against FGF2, with pre-clinical and clinical development. Reflecting the multifunctional properties of FGF2, excess FGF2 activity is involved in disease progression. Four therapeutic applications have been described here, including the treatment of wet AMD, achondroplasia, bone cancer pain, and lung cancer—all of which show RBM-007 as an expected, overall candidate for the therapeutic treatment of diseases affected by excess FGF2.
Regarding wet AMD, we have shown in vitro and in vivo evidence that excess FGF2 plays a vital role in wet AMD by promoting angiogenesis, and that RBM-007 blocks both choroidal neovascularization and subretinal fibrosis. Moreover, combined treatment of RBM-007 and ranibizumab (Lucentis
®) showed a synergistic effect in preventing CNV
[19] although the action mechanisms remain to be clarified. This therapeutic array is further supported by the finding that FGF receptor double-conditional knockout (
Fgfr1/2) mice showed a marked reduction in CNV accompanied by a decrease in the FGF2 level upon laser injury
[20]. Additionally, FGF2 was the only essential ligand in the in vivo models of CNV, showing that FGF2 regulates pathogenic angiogenesis via the STAT3 pathway
[21].
The therapeutic applicability of RBM-007 for achondroplasia was first suggested in an ovariectomized (OVX) rat model, a well-established model for osteoporosis; severe disruption of the epiphyseal growth plate occurred in OVX rats and RBM-007 sharply blocked the disruption of the epiphyseal growth plate in a dose-dependent manner
[16]. This finding suggests that RBM-007 might ameliorate the epiphyseal growth plate and prevent skeletal dysplasias, including achondroplasia, which is related to excessive FGFR3 activation.
In future, a long-lasting modification of RBM-007 will offer potential for extended therapeutic duration that could be beneficial for wet AMD patients who in “real-world” clinical management receive less frequent intravitreal injections, as well as for ACH young patients who receive subcutaneous injections for the entire medication period from childhood for 12–14 years. Ongoing and further clinical studies along these lines should provide us with a novel therapy for unmet medical needs and other applications, such as to diagnostics or for immune modulation.
 +1 point
+1 point





