1000/1000
Hot
Most Recent
 +1 point
+1 point
As more approved COVID-19 vaccines are made available and supply meets or exceeds demand, medical and public health professionals will increasingly be faced with the challenge of vaccine hesitancy. This article describes a demand creation strategy to overcome COVID-19 vaccine hesitancy using methods and evidence from behavioral science and social marketing, and describes a specific campaign aimed at increasing vaccination rates in high supply settings.
As more approved COVID-19 vaccines are made available and supply meets or exceeds demand, medical and public health professionals will increasingly be faced with the challenge of vaccine hesitancy [1][2]. There is an urgent need to create demand in groups that are either uninformed, vaccine hesitant, or actively resistant to COVID-19 vaccination. This paper reviews theory, evidence, and practice recommendations from the fields of health communication, health promotion, health education, behavioral economics, and social marketing to develop a vaccine demand creation strategy.
Specifically, authors focus on key elements including supply side confidence [3], vaccine brand promotion strategy [4][5], service marketing [6], and competition (i.e., the promotion of unproven alternatives to vaccination) [7]. We recommend a demand creation strategy for COVID-19 vaccination based on a combined approach of building a positive brand identity for vaccination behavior together with the use of proven behavioral sciences approaches (e.g., nudges) [8][9] combined with strategic social marketing planning. Success will also be dependent on the brand characteristics and brand equity of the vaccine products themselves, which differ and have received varying levels of coverage both positive and negative in traditional news and social media [10].
Authors present a prototype COVID-19 brand identity based on the reality that there are multiple vaccine brands in the market and a need for specific marketing to build confidence and demand for them both collectively and for individual vaccines. Such communications and marketing approaches aimed at persuasion should follow World Health Organization guidance, outlined in the paper [11]. Within the suggested strategy, we also include a review of and recommendations for the use of both incentives and disincentives that can augment other efforts and give examples of interventions that can misfire when using incentives and disincentives [12]. The paper also makes recommendations about factors that need to be considered in relation to vaccine delivery services and systems that if done badly may reduce vaccine uptake or result in the creation of more vaccine hesitancy. We argue for tactics, including formative research (i.e., to create more effective vaccine promotion strategies and tactics), to avoid common failings of incentive schemes that can arise if the degree of and reasons for specific population vaccine hesitancy is not understood in advance [13]. In summary, we argue for the need for well researched and tested demand creation strategies that use a mix of interventions that integrate communication campaigns with brand strategy, supply side issues, competition strategy, and service delivery considerations.
Brands build relationships between consumers and products, services, or lifestyles by providing beneficial exchanges and adding value to their objects [14]. Effective branding clearly frames the choices facings consumers and creates an identity that promotes brand choice over alternatives. In the health domain, this encompasses both product (e.g., vaccine) choice as well as behavior change (e.g., choosing to get vaccinated) [15]. Vaccine branding is needed for short term promotional purposes and to inform long-term strategic planning in both high supply and low supply situations.
The early stages of vaccine rollout in many countries have been characterized by an emphasis on building confidence in vaccines generically and appeals to social solidarity (i.e., getting vaccinated is normative, or the right thing to do, and that vaccines are safe and effective). In addition, governments have also focused on making access easy, and at low or no cost. However, as time goes on and supply is in equilibrium or exceeds demand considerations beyond safety, effectiveness and social solidarity will be needed to promote uptake among the hesitant [16].
Diffusion of innovation (DOI) theory offers guidance here [17]. We envision a diffusion curve ranging from the early adopters who actively seek vaccination, to those who are unsure or hesitant, to those who actively resist and or are actively opposed to vaccination. In the short-term, COVID-19 demand creation will be relatively easy as the early adopters, (i.e., the enthusiastic) will come forward without much persuasive effort. However, as time goes on, in high-supply countries, those who are hesitant will come to represent more of the unvaccinated. As the hesitant come to the front of the queue there will be a need for more targeted approaches that speaks to the concerns held by these groups.
The same is true for low-supply countries, with the difference being the hesitant as a proportion of the community. One way to delay lower demand in both situations is, in the short term, to adopt a selective targeting strategy aimed at specific high-risk groups who also exhibit high demand (e.g., older adults with co-morbidities and/or front-line health workers).
Brand development always occurs in the context of competition and barrier analysis (another of the ten key guidelines set out above). Choosing one product, or service, or health behavior over another involves comparisons of costs and benefits, and overcoming barriers to purchase, adoption, and the value associated with the product, service or behavior [18]. For COVID-19 vaccination, this will critically involve where a population stands on the diffusion curve for vaccine uptake from enthusiastic to resistant.
Inevitably, as the vaccine rolls out and the remaining unvaccinated population is increasingly hesitant and resistant, vaccine demand creation will need to move from the generic “get vaccinated” branding towards a more specific vaccine product brand promotion approach. In a competitive and potentially crowded market place with many vaccines behind developed and approved we will enter a situation in which people in some countries (mainly the richer ones) will potentially have an individual choice of vaccine products each with varying reported levels of effectiveness, side effects, and other potential factors that may influence both preference and hesitancy. Before we reach this stage, governments and public health agencies must make decisions about which vaccines to procure for their population. Decisions about which vaccines to procure may well need to be tied increasingly into target group confidence in particular vaccine brands as well as maintaining confidence in a generic concept of the benefits of vaccination.
In brief, authors need a clearly identified generic demand strategy and then increasingly specific brand promotion strategies to overcome hesitancy. Based on these market-level considerations, we propose a conceptual model for approaching and overcoming COVID-19 vaccination hesitancy (see Figure 1).
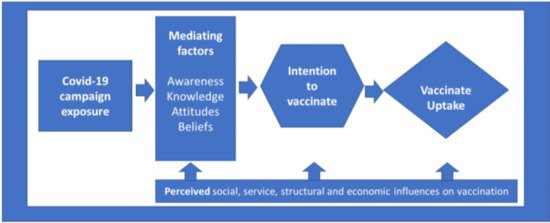
Figure 1. Social, service, structural, and economic influences on vaccination.
In the early phases of vaccination in 2021–2022, there will in many countries be more demand than supply. However, as time passes and there is more supply than demand, hesitancy will increasingly be a key (if not the most important) factor in achieving global population protection. Hesitancy has many causes and the hesitant are not a uniform group, reasons vary by context and history. As many vaccines emerge and are approved the potential to add to hesitancy will emerge in the form of preferences for one vaccine over another and depending on in-country availability hesitancy may be increased if access is not available to what citizens believe are the post effective/safe vaccines due to issues such as cost or political alignment between suppler counties and receiving countries.
COVID-19 has the potential to reverse many of the advances seen in recent decades in reducing inequality and promoting wellbeing both within and between rich and low and middle in countries. One of the key disparities is between rich and poor countries speed of access to vaccines [19]. Both cost and supply will factor in in-country availability but so will confidence in which vaccine is acquired for mass distribution [20]. Such vaccines will need to be safe, effective, practice (e.g., little need for a cold chain) and have a strong trusted brand. For example, it is unlikely that in countries where Russia is perceived to be a less trustworthy country that people will be happy to uptake the Sputnik V vaccine, regardless of its efficacy. Similarly, in countries such as China that want to promote their own vaccine developers, it is unlikely that people will have high demand for Western vaccine brands such as Pfizer or AstraZeneca.
The speed of COVID-19 vaccine development in 2020–2021 was unprecedented [21]. As of the time of this writing, there are a growing number of vaccines approved and in many more in the development pipeline. The sheer number of vaccines that will be available will lead to a need to discriminate which vaccine is most appropriate in a given country setting. Vaccine brand characteristics such as effectiveness, type of regulatory approval, need for cold storage, price, viability, security of supply, origin of manufacture, time of supply, public confidence, and professional confidence will all play into decisions about which vaccines governments will seek to acquire and distribute. Factors such as public trust and affiliation with specific brands will also need to be considered.





